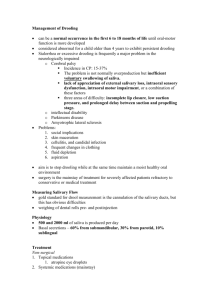
Evaluation and Management of Drooling
advertisement

Drooling surgical options Watad waseem Submandibular and Sublingual gland innervation Superior salivatory nucleus - nervus intermedius - facial nerve - chorda tympani - lingual nerve - submandibular ganglion submandibular/lingual glands Parotid innervation Inferior salivatory nucleus glossopharyngeal nerve - Jacobsen’s nerve lesser superficial petrosal nerve - otic ganglion - auriculotemporal nerve Salivary gland innervation Parasympathetic system stimulation causes an increase in saliva flow from all glands Sympathetic system stimulation causes increase in saliva flow from submandibular gland but has no effect on parotid flow Treatment Options Multidisciplinary approach Non-invasive modalities Trial of medication Surgery Surgical options Reduction of salivary flow Relocation of salivary flow combination Surgical options Submandibular gland excision Parotid duct ligation Transtympanic neurectomy Submandibular duct rerouting Parotid duct rerouting Surgical indications Age 5-6 Failed non-surgical management > 6 months Stable neurological status Drooling with non-operative patient Surgical contra-indications High risk for operation unilateral HL for tympanic neurectomy Rerouting of salivary duct in esophagus disoerder, ch. aspiration Pre-operative assessment Lat neck x-ray , F.O for adenoids adenoidectomy if necessary Barium audiometrey Wilke procedure - 1967 Bil. submandibular gland exc. And bil. Parotd duct relocation. Success rate 85% Postoperative complication (35%) and high morbidity Modification of the procedure Submandibular Gland Excision + partid duct ligation High success rate(85 – 100%)- (Shot) Very common Low morbidity Mild swelling of face, external scars, xerostomia , parotitis Parotid duct ligation Location of the pappila , insert lacrimal probe Elliptical incision made around the parotid duct. Duct dissected for 1 cm, suture ligated and resected. The buccal mucosa is then repaired. Rerouting of submandibular duct Cuff of mucosa dissected around duct and marked medially and laterally Duct dissected 3-4 cm or until gland reached Tonsil used to create a tunnel just posterior to anterior tonsillar pillar and sutures passed with duct Tonsillectomy performed if obstructive tonsils Rerouting of submandibular duct(cont’d) relocation in base of ant. Pillar : no need for TE , less infection Rate success 80-100% Sublingual gland exc. Advantages: Decreased xerostomia, problems with taste and dysphagia Disadv: Ranula, sialoadenitis, sialolithiasis, aspiration pneumonia Studies on submandibular duct rerouting Crysdale - 8% ranula rate O’Dywer - 15 year follow -up study, 94% of parents stated their child benefited, 50% had complete cessation of drooling Transtympanic neurectomies 80% success rate Must take both chorda and tympanic plexus Hypotympanic branch in 50% of patients Low speed drill Loss of taste in anterior 2/3 of tongue and xerostomia Contraindicated in unilateral SNHL Transtympanic neurectomies of drooling – regeneration of tympanic nerves Use for completion the surgery therapy for drooling Recurrence Laser photocoagulation of parotid duct No scars no xerostomia 40/48 patient improvement (chang – 2001) Swelling of parotis, hematoma, infection