Generalized-Anxiety-Disorder-Andel-2013
advertisement

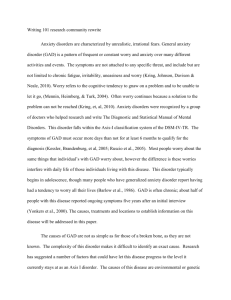
Pediatric Generalized Anxiety Disorder Andel V. Nicasio, MSEd University of Central Florida 7936 Child Psychopathology October 23, 2013 Aims of this presentation 1. 2. 3. 4. 5. Illustrate the historical evolution of Generalized Anxiety Disorder (GAD) Review the DSM-5 taxonomy for GAD Explain etiology, onset, prevalence and course of GAD Review the main theoretical and conceptual models of GAD Present a new theoretical model for pediatric GAD Aim 1 • Illustrate the historical evolution of Generalized Anxiety Disorder (GAD) Nosology and Historical Developments 18th Century - Anxiety was considered a medical illness (Berrios, 1996). 19th Century - Freud viewed Anxiety as resulting from sexual libido unable to find discharge either because of inadequate sexual activity or by inhibitions due to repression (Haggard et al. 2008). Distinguished between Anxiety Neurosis from Neurasthenia, a condition first described by George Beard in 1868. Neurasthenia at the time was a common diagnosis that broadly included anxiety symptoms among other symptoms (e.g., easy fatigability), many of which are now characteristics of chronic fatigue syndrome. Later, Freud modified his theory - “Anxiety was more closely related to fear, occurring in response to perceived dangers, either external or internal. This led to focus on the ego, one of whose functions is to anticipate and negotiate danger situations” (Haggard et al. 2008 , p. 471). GAD in the DSM DSM-I Anxiety Reaction DSM-II Anxiety Neurosis DSM-III GAD (1 month duration) Panic Disorder DSM-IV GAD (6 month duration) Includes Overanxious Disorders of Childhood Anxiety Disorders NOS Diagnostic criteria for GAD in DSM-III A - Generalized persistent anxiety is manifested by symptoms from three of the following four categories: (1) Motor tension: shakiness, jitteriness, jumpiness, trembling, tension, muscle aches, fatigability, inability to relax, eyelid twitch, furrowed brow, strained face, fidgeting, restlessness, easy startle (2) Autonomic hyperactivity: sweating, heart pounding or racing, cold, clammy hands, dry mouth, dizziness, light-headedness, paresthesias (tingling in hands or feet), upset stomach, hot or cold spells, frequent urination, diarrhea, discomfort in the pit of the stomach, lump in the throat, flushing, pallor, high resting pulse and respiration rate (3) Apprehensive expectation: anxiety, worry, fear, rumination, and anticipation of misfortune to self or others (4) Vigilance and scanning: hyperattentiveness resulting in distractibility, difficulty in concentrating, insomnia, feeling “on edge,” irritability, impatience B - The anxious mood has been continuous for at least one month. C - Not due to another mental disorder, such as a depressive disorder or schizophrenia. D - At least 18 years of age Diagnostic criteria for GAD in DSM-III-R A - Unrealistic or excessive anxiety and worry (apprehensive expectation) about two or more life circumstances, e.g., worry about possible misfortune to one’s child (who is in no danger) and worry about finances (for no good reason), for a period of six months or longer, during which the person has been bothered more days than not by these concerns. In children and adolescents, this may take the form of anxiety and worry about academic, athletic, and social performance. B - If another Axis I disorder is present, the focus of the anxiety and worry in A is unrelated to it, e.g., the anxiety or worry is not about having a panic attack (as in panic disorder), being embarrassed in public (as in social phobia), being contaminated (as in OCD), or gaining weight (as in anorexia nervosa). C - The disturbance does not occur only during the course of a mood disorder or a psychotic disorder. D - At least 6 of the following 18 symptoms are often present when anxious (do not include symptoms present only during panic attacks): Motor tension - (1) trembling, twitching, or feeling shaky; (2) muscle tension, aches, or soreness; (3) restlessness; (4) easy fatigability. Autonomic hyperactivity - (5) shortness of breath or smothering sensations; (6) palpitations or accelerated heart rate (tachycardia); (7) sweating, or cold clammy hands; (8) dry mouth; (9) dizziness or lightheadedness; (10) nausea, diarrhea, or other abdominal distress; (11) flushes (hot flashes) or chills; (12) frequent urination; (13) trouble swallowing or “lump in throat”. Vigilance and scanning - (14) feeling keyed up or on edge;(15) exaggerated startle response; (16) difficulty concentrating or “mind going blank” because of anxiety; (17) trouble falling or staying asleep; (18) irritability. E - It cannot be established that an organic factor initiated and maintained the disturbance, e.g., hyperthyroidism, caffeine intoxication. DSM-III-R Motor tension (1) trembling, twitching, or feeling shaky (2) muscle tension, aches, or soreness (3) restlessness (4) easy fatigability Autonomic hyperactivity DSM-IV (1) restlessness or feeling keyed up or on edge (2) being easily fatigued (3) difficulty concentrating or mind going blank (4) irritability (5) muscle tension (5) shortness of breath or smothering sensations (6) sleep disturbance (difficulty falling or (6) palpitations or accelerated heart rate (tachycardia) staying asleep, or restless unsatisfying sleep) (7) sweating, or cold clammy hands (8) dry mouth (9) dizziness or lightheadedness (10) nausea, diarrhea, or other abdominal distress (11) flushes (hot flashes) or chills (12) frequent urination (13) trouble swallowing or “lump in throat” Vigilance and scanning (14) feeling keyed up or on edge (15) exaggerated startle response (16) difficulty concentrating or “mind going blank” because of anxiety (17) trouble falling or staying asleep (18) irritability Aim 2 • Review the DSM-5 taxonomy for GAD • DSM-5 GAD Model What is Generalized Anxiety Disorder? DSM-5 Taxonomy of GAD A. Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance). B. The individual finds it difficult to control the worry. C. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms having been present for more days than not for the past 6 months): Note: only one item is required for children. 1. Restlessness or feeling keyed up or on edge 2. Being easily fatigued 3. Difficulty concentrating or mind going blank 4. Irritability 5. Muscle tension. 6. Sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep) DSM-5 Taxonomy of GAD D. The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. E. The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism). F. The disturbance is not better explained by another mental disorder (e.g. anxiety or worry about having panic attacks in panic disorder, negative evaluation in social anxiety disorder [social phobia], contamination or other obsessions in OCD, separation from attachment figures in SAD, reminder of traumatic events in PTSD, gaining weight in anorexia nervosa, physical complains in somatic symptom disorder, perceived appearance flaws in body dysmorphic disorder, having a serious illness in illness anxiety disorder, or the content of delusional beliefs in schizophrenia or delusional disorder). GAD in the DSM-5 Children with GAD tend to worry excessively about their competence or the quality of their performance. During the course of the disorder, the focus of worry may shift from one concern to another. Associated Features Supporting Dx Muscle tension – trembling, twitching, feeling shaky, and muscle aches or soreness. Somatic symptoms – sweating, nausea, diarrhea Exaggerated startle response Symptoms of autonomic hyperarousal – (e.g. accelerated heart rate, shortness of breath, dizziness) are less prominent than in panic disorder. Other conditions associated with stress (e.g. irritable bowel syndrome, headaches) frequently accompany GAD. GAD Prevalence 12-month prevalence is 0.9% among adolescents and 2.9% among adults in the general community of U.S. In other countries, the 12-month prevalence is 0.4% - 3.6%. Lifetime morbid risk is 9.0% Prevalence of diagnosis peaks in middle age and declines across the later years in life. European-descent individuals tend to experience GAD more frequently than non-European descent (i.e., Asian, African, Native American and Pacific Islander). Persons from developed countries are more likely to report that they have experience GAD than those from nondeveloped countries. Onset and Course of GAD Many people with GAD report that they have felt anxious and nervous all of their lives. The median age at onset is 30 y/o. Age at onset is spread over a broad range. Symptoms of worry and anxiety may occur early in life, but are then manifested as an anxious temperament. Symptoms tend to be chronic and wax and wane across lifespan, fluctuating from syndromal to subsyndromal forms of disorder. Rates of full remission are very low. Gender Differences and Comorbidity More frequently diagnosed in females (55-60%) than males. In epidemiological studies 2/3 are females. Female and males appear to have the same symptoms, but present different patterns of comorbidity. Females - Comorbidity confined to anxiety disorders and unipolar depression. Males - Comorbidity more likely to extend to substance abuse disorders. Comorbidity – People with GAD are likely to have met, or currently meet, criteria for other anxiety and unipolar depression disorder. Comorbidity with substance abuse, conduct, psychotic, neurodevelopmental, and neurocognitive disorders LESS common. GAD Risk and Prognosis Factors Temperamental – Behavioral inhibition, negative affectivity (neurotism), and harm avoidance have been associated with GAD. Environmental – No environmental factors have been identified as specific to GAD or necessary or sufficient for making the diagnosis. Genetic and physiological – 1/3 of the risk of experiencing generalized anxiety disorder is genetic, and these genetic factors overlap with the risk of neurotism and are shared with other anxiety and mood disorders, particularly MDD. Culture Considerable cultural variation in the expression of GAD. In some cultures somatic symptoms predominate, but in other cultures cognitive symptoms predominate. Cultural expressions are more evident in the initial presentation; over time more symptoms tend to be reported. Important to consider the social and cultural context when evaluating whether worries about certain situations are excessive. Differential Diagnosis Other Disorders GAD Social Anxiety Disorder Often have anticipatory anxiety focused on upcoming social situations in which they must perform or be evaluated by others People with GAD worry whether or not they are being evaluated. Obsessive-Compulsive Disorder The obsessions are inappropriate ideas that take the form of intrusive and unwanted thoughts, urges, or images. Focus of worry is about forthcoming problems and it is the excessiveness of the worry about future events that is abnormal. DSM-5 Model Aim 3 • Literature Review of Pediatric GAD Prevalence Anxiety is the most common mental disorder in children and adolescents (Anderson et al. 1987). Prevalence rates range from 6% to 20% (Costello et al. 2004). Generalized Anxiety Disorder In community samples, prevalence rates range from 0.1% (Merikangas et al., 2010) to 3.3% (Kessler et al., 2005). In clinical samples, prevalence rates range from 3% (Chorpita et al., 2005) to 15% (Ebesutani et al., 2010). Comorbidity Isolated cases of “pure” anxiety disorders (no co-occurring dx) are relatively rare (Comer & Olfson, 2010). About 70–80% with a lifetime anxiety disorder and 60–90% with an anxiety disorder in the past year meet criteria for at least one additional disorder (Kessler et al. 2006, Lampe et al. 2003, Jacobi et al. 2004, Torres et al. 2008). Individuals with SP, GAD, and SAD are at 15, 9, and 6 times increased odds, respectively, for having a co-occurring anxiety disorder (Grant et al. 2005, Stinson et al. 2007, Ruscio et al. 2008). Cont… Comorbidity Those diagnosed with 12-month GAD, SAD, and SP are at 19, 5, and 3 times increased odds, respectively, for having a co-occurring mood disorder (Merikangas et al. 2002, Grant et al. 2005, Stinson et al. 2007). GAD or SP are at greatest risk for co-occurring bipolar disorder. In cases of co-occurring anxiety and mood disorders, onset of anxiety disorders typically occurs prior to mood disorders (Brady & Kendall,1992) Rate and comorbidity GAD - Lifetime Prevalence GAD Comorbidity Walkup, J. T. et al (2008) - Child-Adolescent Multimodal Treatment Study: GAD was the most common disorder; however, GAD, SAD, and SoP were highly comorbid. GAD Comorbidity Separation Anxiety Disorder Social Phobia Generalized Anxiety Disorder Walkup, J. T. et al (2008) Onset Among all Anxiety Disorders, GAD has the latest mean and median age at onset (early 30s) (Grant et al. 2005, Kessler et al. 2005, Lieb et al. 2005). However, substantial numbers of children and adolescents do meet full criteria (Albano & Hack 2004 , Comer et al. 2004 , Robin et al. 2005 , Alyahri & Goodman 2008). In community samples, 0.1% for children 8-11 y/o and 1.1% for adolescents 12-15 y/o (Merikangas et al. 2010); 8.6% for 8 y/o and 17.1% for 17 y/o (Kashani and Orvaschel, 1990). The onset of GAD may be gradual or sudden and, unsurprisingly, symptoms are often exacerbated by stress (Rapoport & Ismond, 1996) Early GAD onset is associated with greater excessiveness and uncontrollability of worry, as well as a more chronic course with more severe life impairment (Ruscio et al. 2005 ). Gender Gender differences in the prevalence of GAD in children and adolescents are inconsistent. Merikangas et al. (2010) reported no gender differences in a sample of 8–15-year-olds, using the DSM-IV In another study, girls (of all ages) were found to have higher rates than boys (15 % of girls and 9 % of boys (Kashani et al., 1990). Clinical samples have reported no gender differences in GAD in children 9–13 years of age (Last et al., 1992). With respect to symptoms of GAD and/or worry, females report more GAD symptoms than males. Course GAD, phobias, panic disorder, and depressive disorders predicted each other over time, and early-onset GAD was a stronger predictor of later anxiety rather than depressive disorders. Predictors of GAD onset over time - Parental GAD and depression, childhood behavioral inhibition, childhood separation events, and parental overprotection. GAD was associated with the personality trait “reward dependence” (based on self-reported personality) and dysfunctional family functioning. Community sample; N= 3,021; 14–24 years at time 1) for 10 years. Bessdo et al., 2010 Race/Ethnicity Lower lifetime rates of anxiety disorders among immigrants than among US-born natives of the same national origins (Vega et al. 1998 , Grant et al. 2004). Early age at immigration and longer duration residing in the USA are both associated with increased risk for mental disorders among immigrants relative to natives (Breslau et al. 2007). A epidemiological survey conducted in South Africa revealed that rates of GAD were significantly higher in men than women (Bhagwanjee et al. 1998). Suicidality Any single anxiety disorder (phobia, GAD, panic disorder) increased the odds of suicidal ideation by 7.96 times [95% confidence interval (CI) 5.69–11.13] and increased the rate of suicide attempts by 5·85 times (95% CI 3.66–9.32). Rates of suicidal behavior increased with the number of anxiety disorders. Estimates of the population attributable risk suggested that anxiety disorders accounted for 7–10% of the suicidality in the cohort. Christchurch Health and Development Study (CHDS). 25-year longitudinal study; over 1000 participants. Subjects aged 16–18, 18–21 and 21–25 years. Boden et al., 2007 Temperament and Genes Genetic correlations between GAD and neuroticism were high 0.80 (95% confidence interval=0.52–1.00), with no significant difference between men and women (1.00 and 0.58, respectively) (Hettema et al, 2004). Bivariate Twin Model for Neuroticism and Generalized Anxiety Disorder aThe phenotypic correlation is decomposed into the additive genetic correlation (rg) between additive genetic factors (AN and AG), the common environmental correlation (rc) between common familial environmental factors (CN and CG), and the individual-specific environmental correlation (re) between individual-specific environmental factors (EN and EG) for neuroticism and generalized anxiety disorder, respectively. Temperamental Trait and GAD Distribution of harm avoidant scores and presence/absence of current DSM-IV GAD in children and adolescents. Genes and Anxious Brains (Monkeys) Genes and Anxious Temperament (AT) Neurological Pathways Contradictory research findings - Youth with GAD exhibited greater amygdala volumes (De Bellis, et al., 2000), whereas reduced amygdala volume was identified in adolescents with GAD, SAD, or SoPh (Milham et al., 2005). Patients with GAD fail to engage regulatory regions in response to heightened displays of amygdala activity resulting from emotional stimuli (Etkin et al., 2010). Compared to healthy controls, adolescents with GAD displayed a relatively weaker negative task-dependent functional connectivity (TDFC) between the lateral prefrontal cortices and the amygdala during an emotional attention orienting task (Thomas et al., 2001). This is consistent with the notion that individuals with anxiety are less able to regulate neural responses to emotion, even prior to adulthood. Schematic Framework Pine, et al 2008 Areas of the Brain Affected by GAD The noradrenaline pathways in GAD Noradrenaline Pathways Serotenergic Pathways GABAergic pathways The Septohippocampal Circuit Fear and Anxiety in the Brain Networks that Support Negative Reactivity and Regulation Etkin, A. & Wager, T. D. (2010) Genes A meta-analysis of family and twin studies of anxiety disorder estimated GAD heritability to be 32% (Hettema et al. 2001). Genes Associated with GAD Gene Name and Abbreviation Serotonergic System Serotonin transporter (SLC6A4 ) Location 17q11.1–q12 Modulation of monoamine metabolism Monoamine oxidase A (MAOA ) Xp11.4-p11.23 Dopaminergic system Dopamine transporter (DAT1 ) Regulator of G-protein signaling Regulator of G-protein signaling 2 (RGS2 ) Studies Supporting the Association Ohara et al. 1999 You et al. 2005 Samochowiec et al . 2004 Tadic et al. 2003 p15.3 Rowe et al. 1998 q31 Koenen et al. 2009 Cognitive Symptoms Worry and the disturbance of mental processes (e.g., thinking, planning, abstract reasoning, problem solving, and recall) encompass the cognitive features of anxiety (Kendall et al., 2004). With GAD, there is an overall attitude of apprehension. Children and adolescents with GAD are often described as self-conscious, perfectionistic “worriers” (Beidel, Turner, 2005; Eisen & Kearney, 1995). Cognitive Factors Youth with GAD display problematic cognitive processes (Ginsburg & Affrunti, 2013). Youth with GAD are: more likely to overestimate the negative consequences of their actions, expect negative consequences to occur with greater frequency, overestimate the likelihood of threatening situations, interpret ambiguity as threatening, and have impaired problem-solving skills Albano et al., 1996; Bögels et al., 2003; Léger et al., 2003 Attentional Bias Youth with GAD are more likely to interpret ambiguous information as threatening and have an attentional bias toward threatening stimuli. Waters et al. (2008) examined the attentional bias for angry and happy faces in 7-12 y/o with GAD (N= 23) and nonanxious controls ( N= 25). Found that GAD severity was associated with greater attentional bias toward angry faces. Mean attention bias scores (+SE) for angry and happy faces as a function of group (CON = control; LCA = low clinical anxiety; HCA = high clinical anxiety). Attention Orienting A process that involves focusing one’s attention on salient stimuli. Recent RCTs have demonstrated that training anxious children to modify their attentional threat biases can facilitate disengagement of attention to threat, which in turn can reduce anxiety symptoms (Bar-Haim et al.,2011; Eldar et al., 2012). These findings suggest that attention biases might emerge over time through reinforcement or as a means to reconcile ambiguous situations (Field et al., 2010). Dot-probe paradigm Threat Learning Youth with GAD tend to have difficulties learning to discriminate threat cues from safety cues, term Threat Learning. Threat learning involves correctly determining what cues and in which situations indicate potential danger or safety (Pine et al., 2009; Britton et al., 2011). Youth with GAD underestimate their ability to cope with threatening events (Weems & Wattas, 2005). Physiological Symptoms The physiological element of anxiety revolves around the biological effects anxiety has on the body. Physical symptoms generally reflect elevated sympathetic autonomic nervous system activity and include increased heart rate and blood pressure, increased muscle tension, muscle tremor, alterations in salivation and perspiration, bodily temperature changes, and modifications of stomach gastric and acidic actions (Beidel & Turner, 2005). These symptoms are caused by the release of cortisol and epinephrine in the brain when a threat is detected (Wood & McLeod, 2008). Physiological Symptoms Tracey et al. (1997) found that youth with GAD endorsed experiencing several physical symptoms, including restlessness (74% of the sample), irritability (68%), difficulties concentrating (61%), sleep disturbance (58%) headaches (36%), muscle tension (29%), and stomachaches (29%). Behavioral Symptoms In GAD, the anxiety and avoidance behavior generalizes to non-threatening cues; as a result, numerous objects and events that were previously harmless become cues that evoke anxiety. In essence, individuals with GAD are in a constant state of vigilance (Rapoport & Ismond, 1996). Due to the self-conscious, perfectionistic nature of youth with GAD, they ask for and require repeated reassurance from others (Beidel & Turner, 2005; Eisen & Kearney, 1995). Children and adolescents with GAD usually demonstrate a rather debilitating restriction of age-appropriate social functioning and activities (Eisen & Kearney, 1995). Parenting and Parent-Child Factors Longitudinal studies suggests a reciprocal relationship: parental behaviors affect child anxiety and child anxiety symptoms affect parental behaviors (Wijsbroek et al., 2011; Murray et al., 2008) Peer Relationship Children with GAD may be more selective and may avoid friendships with `adventurers' or `risk-takers‘ who are not similarly concerned with rules and/or about possible injury. Social activities may be restricted due to concerns about safety and performance. Children with GAD and Healthy Control group had similar relationships with peers, with the exception of an overall reduced number of friends. Scharfstein, et al. 2011 Aim 4 • Theoretical Models Kertz Woodruff-Borden (2010) Etiological Model of Pediatric GAD Beck’s Model & Metacognitive Model Pathological anxiety derives from the misperception of danger, resulting from distortions in the way information is perceived. Based on cognitive therapy as applied to appraisal of threat (Beck, Distinguishes between two types of worries – type 1 (worries about everyday events and physical sensations) and type 2 (worries about – both positive and negative appraisals of worrisome activity) (Wells, 1995). & Emery,1985). GAD sufferers view the world as a dangerous place, and in order to avoid possible danger or to plan ways to deal with the occurrence of danger, they feel that it is imperative to constantly scan the environment for cues of threat. Beliefs are centered on two main themes: (1) beliefs about the uncontrollability of worry, and (2) beliefs about the dangerous consequences of worrying for mental, physical, and/or social functioning. Barlow’s Emotion Theory (2002) GAD is the major feature of all Anxiety disorders. Synergy between genetic vulnerability (genetic contribution) and psychological vulnerability (diminished sense of control) Early experiences (uncontrollable or unpredicted events) plus overprotective/intrusive/punitive parenting styles lead to low perception of control, increased neurobiological activity and varied somatic outputs. Barlow’s Model Translational Development Neuroscience Figure depicts the time course of atypical versus typical development. The red arrow at an early childhood indicates a perturbation followed by an immediate or later onset trajectory involving dynamic changes in molecular systems, information processes running on hierarchically distributed neural networks, and resulting sychopathology, which when sufficiently altered (brown circle) comes to clinical attention. March, 2011 What is like to live with GAD Across the anxiety disorders, GAD may be the most profound and have the most deleterious effect on functioning and healthrelated quality of life (Grant et al. 2005). Significantly increased risk of impaired social and role functioning, mental health, and overall physical and mental well-being (Mendlowicz & Stein 2000; Stein & Heimberg 2004). Associated with poor marriage stability, as afflicted individuals are almost twice as likely to have their first marriage end in divorce (Kessler et al. 1998). Occupational impairment is also common (Merikangas et al. 2007). Cost to Society and Individuals with BP When untreated - reduced quality of life, including decrements in social functioning, role functioning, educational attainment, financial independence, and mental health (Mendlowicz & Stein 2000). Associated with decrements in educational achievement. Predictor of failure to complete high school, failure to enter college among high-school completers, and failure to complete college among college entrants (Kessler et al. 1995). Aim 5 • Present a new theoretical model for pediatric bipolar disorder Generalized Anxiety Disorder Model Nicasio, A. (2013) References Albano, A. M., & Hack, S. (2004). Children and adolescents. In R. G. Heimberg, C. L. Turk, & D.S. Mennin (Eds.). Generalized Anxiety Disorder: Advances in Research and Practice. New York, NY: Guilford. Albano, A. M., Chorpita, B. F., Barlow, D. H. (2006). Childhood anxiety disorders. In: Mash, E. J., Barkley, R. A., Mash, E. J., Barkley, R. A., (Eds). Child psychopathology. New York: Guilford, p. 196–241. Albano, A. M., Chorpita, B. F., Barlow, D. H. (1996). Childhood anxiety disorders. In: Mash, E. J., Barkley, R. A., Mash, E. J., Barkley, R. A, editors. Child psychopathology. New York: Guilford; p. 196–241. Alyahri, A. , & Goodman, R. (2008). The prevalence of DSM-IV psychiatric disorders among 7–10 year old Yemini schoolchildren. Social Psychiatry and Psychiatric Epidemiology, 43, 224–2. American Psychiatric Association (1952). Diagnostic and Statistical Manual of Mental Disorders(DSM-I). Washington, DC : APA. American Psychiatric Association (1968). Diagnostic and Statistical Manual of Mental Disorders, 2nd ed. (DSM-II). Washington, DC: APA. American Psychiatric Association (1980). Diagnostic and Statistical Manual of Mental Disorders, 3rd ed. (DSM-III). Washington, DC: APA. American Psychiatric Association (1987). Diagnostic and Statistical Manual of Mental Disorders, 3rd ed., revised (DSM-III-R). Washington, DC : APA American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV). Washington, DC: APA. American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders, 4th ed., text revision (DSM-IV-TR). Washington, DC: APA. American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th ed., text revision (DSM-5). Washington, DC: APA. Anderson, J. C., Williams, S., McGee, R., & Silva, P. (1987). DSM-III disorders in preadolescent children: Prevalence in a large sample from the general population. Archives of General Psychiatry, 44, 69-76. Barlow, D. H. (2002). Anxiety and its disorders. The nature and treatment of anxiety and panic (2nd Ed.) New York: Guilford Press. Bar-Haim, Y., Morag, I., Glickman, S. (2011). Training anxious children to disengage attention from threat: a randomized controlled trial. J Child Psychol Psychiatry. 52(8), 861–9. Epub 2011/01/22. 57. Bhagwanjee, A., Parekh, A., Paruk, Z. et al (1998). Prevalence of minor psychiatric disorders in an adult African rural community in South Africa. Psychological Medicine, 28, 1137-1147. Beck, A.T., & Emery, G. (1985). Anxiety disorders and phobias: A cognitive perspective. New York: Basic Books. Beesdo, K., Pine, D. S., Lieb, R., Wittchen, H. (2010). Incidence and risk patterns of anxiety and depressive disorders and categorization of generalized anxiety disorder. Arch Gen Psychiatry, 67(1), 47–57. Beesdo, K., Pine, D.S., Lieb, R. & Wittchen, H.U. (2010). Incidence and Risk of Patterns of Anxiety and Depressive Disorders and Categorization of Generalized Anxiety Disorder. Archives of General Psychiatry, 67, 47–57. Beidel, D. C. & Turner, S. M. (2005). Childhood Anxiety Disorders: A Guide to Research and Treatment. Routledge, Taylor & Francis Group, New York. Berrios, G. E. (1996). The history of mental symptoms: Descriptive psychopathology since the nineteenth century. Cambridge University Press. Cambridge England and New York, NY, USA. References Boden, J., Fergusson, D. M., & Horwood, L. J. (2007). Anxiety disorders and suicidal behaviours in adolescence and young adulthood: findings from a longitudinal study. Psychological Medicine, 37(3), 431-440. Bögels, S. M., Snieder, N., Kindt, M., (2003). Specificity of dysfunctional thinking in children with symptoms of social anxiety, separation anxiety and generalised anxiety. Behav Change, 20(3):160–9. Brady, E. U. , & Kendall P. C. (1992). Comorbidity of anxiety and depression in children and adolescents. Psychological Bulletin, 111, 244 –25. Breslau, J., Aguilar-Gaxiola, S., Borges, G., et al. (2007). Risk for psychiatric disorder among immigrants and their US-born descendants: Evidence from the National Comorbidity Survey Replication. Journal of Nervous and Mental Disease, 195, 189–195. Britton, J. C., Lissek, S., Grillon, C., Norcross, M. A., Pine, D.S. (2011). Development of anxiety: the role of threat appraisal and fear learning. Depress Anxiety. 28(1), 5–17. Chorpita, B. F., Moffitt, C. E., Gray, J. (2005). Psychometric properties of the revised child anxiety and depression scale in a clinical sample. Behav Res Ther. 43(3), 309–22. Comer, J. S. , & Kendall, P. C. (2004). A symptom-level examination of parent–child agreement in the diagnosis of anxious youths. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 878 –88. Costello, E. J., Mustillo, S., Erkanli, A., Keeler, G., & Angold, A. (2003 ). Prevalence and development of psychiatric disorders in childhood and adolescence. Archives of General Psychiatry, 60, 837 –844. CNSforum Image Bank: Anxiety – GAD- generalised anxiety disorder. Retrieved on 10/20/2013 from http://www.cnsforum.com/imagebank/section/neurochemical_pathways_GAD/default.aspx CNSforum. The septohippocampal circuit. In L’Encephale 1983; IX, 161B-166B. Retrieved on 10/23/2013 from http://www.cnsforum.com/imagebank/item/septotohippo_circ/default.aspx CNSforum. The areas of the brain affected in generalised anxiety disorder (advanced). In J Clin Psychiatry 2001, 62(11), 22-27. Retrieved on 10/20/2013 from http://www.cnsforum.com/imagebank/item/Neuro_biol_GAD_2/default.aspx CNSforum. Anxiolytics and sedative-hypnotics. In: Essential Psychopharmacology. Neuroscientific basis and practical applications. Stahl S. Cambridge, UK: Cambridge University Press, 1996 167–215. Retrieved on 10/20/2013: http://www.cnsforum.com/imagebank/item/Neuro_path_N_GAD/default.aspx De Bellis, M. D., Casey, B. J., Dahl, R. E., Birmaher, B., Williamson, D. E., Thomas, K. M., et al. (2000). A pilot study of amygdala volumes in pediatric generalized anxiety disorder. Biol Psychiatry, 48(1), 51–7. Epub 2000/07/29.33. Ebesutani, C., Bernstein, A., Nakamura, B. J., Chorpita, B. F., Weisz, J. R. (2010). A psychometric analysis of the revised child anxiety and depression scale-parent version in a clinical sample. J Abnorm Child Psychol. 38(2), 249–60. Eisen, A. R. & Engler, L. B. (2007). Helping Your Socially Vulnerable Child: What to do when your child is Shy, Socially Anxious, Withdrawn or Bullied. New Harbinger Publications. Eisen, A. R. & Kearney, C. A. (1995). Practicioner’s guide to treating fear and anxiety in children and adolescents: A cognitive-behavioral approach. Northvale, NJ: Aronson. References Eldar, S., Apter, A., Lotan D., Perez-Edgar, K., Naim , R. Fox, N. A., Pine, D. S., Bar-Haim, Y. (2012). Attention bias modification treatment for pediatric anxiety disorders: a randomized controlled trial. Am J Psychiatry, 169, 213–220. Etkin, A., Prater, K. E., Hoeft, F., Menon, V., Schatzberg, A. F. (2010). Failure of anterior cingulate activation and connectivity with the amygdala during implicit regulation of emotional processing in generalized anxiety disorder. Am J Psychiatry, 167(5), 545-54. Etkin, A., & and Wager, T. D. (2010). “Brain systems underlying anxiety disorders: a view from neuroimaging", Anxiety Disorders. 1st ed. Cambridge: 2010. 192-203. Cambridge Books Online. Web. 10 October 2013. http://dx.doi.org/10.1017/CBO9780511777578.019 Field, A. P., Lester, K. J. (2010). Is there room for ‘development’ in developmental models of information processing biases to threat in children and adolescents? Clin Child Fam Psychol Rev., 13(4), 315–32. Grant, B. F. , Hasin, D. S., Stinson, F. S., et al. (2005). Prevalence, correlates, co-morbidity, and comparative disability of DSM-IV generalized anxiety disorder in the USA: results from the National Epidemiologic Survey on Alcohol and Related Conditions . Psychological Medicine, 35, 1747 –1759. Grant, B. F., Stinson, F. S., Hasin, D. S., et al. (2004). Immigration and lifetime prevalence of DSM-IV psychiatric disorders among Mexican Americans and nonHispanic whites in the United States: results from the National Epidemiologic Survey of Alcohol and Related Conditions. Archives of General Psychiatry, 61, 1226 –1233. Ginsburg, G. S. & Affrunti, N. W. (2013). Generalized Anxiety Disorder in Children and Adolescents. R.A. Vasa and A. K. Roy (Eds), Pedriatric Anxiety Disorders: A clinical guide, Current Clinical Psychiatry, 71-90, Springer Science+Business Media, New York. Haggard, P., Furman, A., Levy, S. T., et al. (2008). Psychoanalytic theories. In Tasman, A., Kay, J., Lieberman, J., First, M., & Maj, M., eds., Psychiatry, 3rd edn. Chichester : Wiley , pp. 464–485. Hans-Ulrich, W. & Jürgen, H. (2001). Generalized Anxiety Disorder: Nature and Course. J Clin Psychiatry, 62(11), 15–19. Hettema, J. M., Prescott, C. A. & Kendler, K. S. (2004) Genetic and environmental sources of covariation between generalized anxiety disorder and neuroticism. American Journal of Psychiatry, 161, 1581-1587. Jacobi F., Wittchen, H. U., Holting, C., et al. (2004). Prevalence, comorbidity and correlates of mental disorders in the general population: results from the German Health Interview and Examination Survey (GHS). Psychological Medicine, 34, 597 –61. Kashani, J. H., & Orvaschel, H. (1990). A community study of anxiety in children and adolescents. Am J Psychiatry, 147(3), 313–8. Kendall, P.C., Safford, S., Flannery-Schroeder, E., & Webb, A. (2004). Child anxiety treatment: Outcomes in adolescence and impact on substance use and depression at 4 year follow-up. Journal of Consulting and Clinical Psychology, 72, 276–287. Kessler, R. C., Chiu, W. T., J i n , R . , et al. (2006). The epidemiology of panic attacks, panic disorder, and agoraphobia in the National Comorbidity Survey Replication. Archives of General Psychiatry, 63, 415 –42. Kessler, R. C., Berglund, P., Demler, O., et al. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 593 –60. Kessler, R. C., Walters, E. E., Forthofer, M. S. (1998). The social consequences of psychiatric disorders, III: Probability of marital stability. Arch Gen Psychiatry, 155, 1092–1096. References Kertz, S. J., Woodruff-Borden, J. (2011). The developmental psychopathology of worry. Clin Child Fam Psychol Rev, 14(2), 147–97. Lampe, L., Slade, T., Issakidis, C., & Andrews, G. (2003). Social phobia in the Australian National Survey of Mental Health and Well-Being. Psychological Medicine, 33, 637-646. Last, C. G., Perrin, S., Hersen, M., Kazdin, A. E. (1992). DSM-III-R anxiety disorders in children: sociodemographic and clinical characteristics. J Am Acad Child Adolesc Psychiatry, 31(6), 1070–6. Lau, J. Y., Lissek, S., Nelson, E. E., Lee, Y., Roberson-Nay, R., Poeth, K., et al. (2008). Fear conditioning in adolescents with anxiety disorders: results from a novel experimental paradigm. J Am Acad Child Adolesc Psychiatry, 47(1), 94–102. Léger, E., Ladouceur, R., Dugas, M. J., Freeston, M. H. (2003). Cognitive-behavioral treatment of generalized anxiety disorder among adolescents: a case series. J Am Acad Child Adolesc Psychiatry, 42(3), 327–30. Lieb, R., Becker, E., & Altamura, C. (2005). The epidemiology of generalized anxiety disorder in Europe. European Neuropsychopharmacology, 15, 445–452. March, J. S. (2011). Looking to the future of research in pediatric anxiety disorders. Depression and anxiety, 28, 88–98. Mendlowicz, M. V. & Stein, M. B. (2000). Quality of life in individuals with anxiety disorders. Am J Psychiatry, 157(5), 669-82. Merikangas, K. R., He, L. P., Burstein, M., Swanson, S.A., Avenevoli, S. Cui, L., . . . Swendsen, J. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry, 49(10), 980-9. Merikangas, K. R., Avenevoli, S., Acharyya, S., Zhang, H., & Angst, J. (2002). The spectrum of social phobia in the Zurich Cohort Study of Young Adults. Biological Psychiatry, 51, 81 –91. Merikangas, K. R., Ames, M., Cui, L., Stang, P. E., Ustun, T. B., Von Korff, M., Kessler, R. C. (2007). The impact of comorbidity of mental and physical conditions on role disability in the US adult household population. Arch Gen Psychiatry, 64(10), 1180-8. Milham, M. P., Nugent, A. C., Drevets, W. C., Dickstein, D. P., Leibenluft, E., Ernst, M., et al. (2005). Selective reduction in amygdala volume in pediatric anxiety disorders: a voxel-based morphometry investigation. Biol Psychiatry, 57(9), 961–6. Murray, L., de Rosnay, M., Pearson, J., Bergeron, C., Schofield, E., Royal-Lawson, M., et al. (2008). Intergenerational transmission of social anxiety: the role of social referencing processes in infancy. Child Dev. 79(4),1049–64. Oler, J. A., Fox, A. S., Shelton, S. E., Rogers, J. Dyer, T. D., Davidson, R. J., …Kalin, N. H. (2010). Amygdalar and hippocampal substrates of anxious temperament differ in their heritability. Nature, 466(7308), 864-8. Pine, D. S. (2009). Integrating research on development and fear learning: a vision for clinical neuroscience? Depress Anxiety, 26(9), 775–9. Pine, D. S., Guyer, A. E., Leibenluft, E. (2008). Functional magnetic resonance imaging and pediatric anxiety. J Am Acad Child Adolesc Psychiatry, 47(11), 121721. Pine, D. S., Helfinstein, S. M., Bar-Haim, Y., Nelson, E., Zfox, N. A. (2009). Challenges in developing novel treatments for childhood disorders: lessons from research on anxiety. Neuropsychopharmacology, 34(1), 213-28. Rapoport, J., & ismond, D. R. (1996). DSM-IV training guide for diagnosis of childhood disorders. Brunner/Mazel (New York). References Rettew, D. C., Doyle, A. C., Kwan, M., Stanger, C. Hudziak, J. J. (2006). Exploring the boundary between temperament and generalized anxiety disorder: a receiver operating characteristic analysis. Journal of Anxiety Disorder, 20(7). Ruscio, A. M., Lane, M., Roy-Byrne, P., et al. (2005). Should excessive worry be required for a diagnosis of generalized anxiety disorder? Results from the U.S. National Comorbidity Survey Replication. Psychological Medicine, 35, 1761 –1772. Ruscio, A. M., Brown, T. A., Chiu, W. T., et al. (2008). Social fears and social phobia in the USA: results from the National Comorbidity Survey Replication. Psychological Medicine, 38, 15 –28. Scharfstein, L., Alfano, C., beidel, D., Wong, N. (2011). Children with generalized anxiety disorder do not have peer problems, just fewer friends. Child Psychiatry Hum Dev., 42(6), 712-23. Stein, M. B. & Heimberg, R. G. (2004). Well-being and life satisfaction in generalized anxiety disorder: comparison to major depressive disorder in a community sample. J Afffect Disord, 79(1-3), 161-6. Stinson , F. S. , Dawson , D. A. , Chou , S. P. , et al. (2007). The epidemiology of DSM-IV specific phobia in the USA: results from the National Epidemiologic Survey on Alcohol and Related Disorders. Psychological Medicine, 37, 1047 –105 Torres, A. R., Prince, M. J., Bebbington, P. E., et al. (2006). Obsessive–compulsive disorder: prevalence, comorbidity, impact, and help-seeking in the British National Psychiatric Morbidity Survey of 2000. American Journal of Psychiatry, 163, 1978–198. Thomas, K. M., Drevets, W. C, Whalen, P. J., Eccard, C. H., Dahl, R. E., Ryan, N. D., Casey, B. J. (2001). Amygdala response to facial expressions in children and adults. Biological Psychiatry, 49, 309–316. Tracey, S. A., Chorpita, B. F., Douban, J., & Barlow, D. H. (1997). Empirical evaluation of DSM-IV generalized anxiety disorder criteria in children and adolescents. Journal of Clinical Child Psychology, 26, 404–414. Vega, W. A., Kolody, B., Aguilar-Gaxiola, S., et al. (1998). Lifetime prevalence of DSM-III-R psychiatric disorders among urban and rural Mexican Americans in California. Archives of General Psychiatry, 55, 771–7. Walkup, J. T., Albano, A. M., Piacentini, J., Birmaher, B., Compton, S. N., Sherrill, J. T., Kendall, P. C. (2008). Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. New England Journal of Medicine, 359, 2753–2766. Waters, A. M., Henry, J., Neumann, D. L. (2009). Aversive Pavlovian conditioning in childhood anxiety disorders: impaired response inhibition and resistance to extinction. J Abnorm Psychol, 118(2), 311–21. Waters, A. M., Mogg, K., Bradley, B. P., Pine, D. S. (2008). Attentional bias for emotional faces in children with generalized anxiety disorder. J Am Acad Child Adolesc Psychiatry, 47(4), 435–42. Weems, C. F. & Watts, S. E. (2005). Cognitive models of childhood anxiety. In: Velotis CM, editor. Anxiety Disorder Research. Nova Science Publishers, Inc.; Hauppauge, NY, pp. 205–232 Wells, A. (1995). Meta-cognition and worry: A cognitive modelof generalised anxiety disorder. Behavioural and Cognitive Psy-chotherapy, 23, 301-320. Wijsbroek, S. A., Hale, III, W. W., Raaijmakers, Q. A., Meeus, W. H. (2011). The direction of effects between perceived parental behavioral control and psychological control and adolescents’ self-reported GAD and SAD symptoms. Eur Child Adolesc Psychiatry, 20(7), 361–71. Wood, J. J., & McLeod, B. D. (2008). Child anxiety disorders: A family-based treatment manual for practitioners. New York: Norton.