Description
advertisement

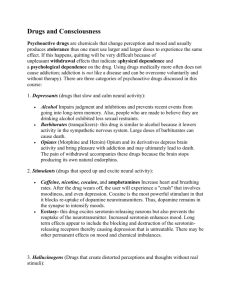
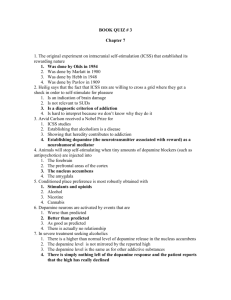
Drug abuse By Mohie aldien elsayed (MD) Learning Objectives • To be able to: • Identify the anatomical areas of the brain involved in the reward pathway • Outline the neurotransmitter systems which activate the reward pathway • Identify the anatomical areas and receptors involved in activation from psychoactive drugs • Identify the anatomical areas and receptors involved in the withdrawal from psychoactive drugs • Understand concepts relating to the development of addiction Corpus Callosum Connects Hemispheres Creativity and Problem Solving Frontal Cortex Planning, Strategizing, Logic, Judgment Cerebellum Coordinates muscles/ movement and thinking processes Thalamus Nucleus accumbens Extended Amygdala Emotional responses: fear and anger Ventral tegmental area Locus coeruleus Hippocampus Forms Memories Coordinates thinking processes Dopamine Pathways: Reward, Pleasure, Euphoria, Motor Function, Decision making Prefrontal cortex Hippocampus Nucleus accumbens Ventral tegmental area Raphe Serotonin Pathways: Mood, Memory, Sleep, Cognition Reward Pathway • There is a axonal network in the brain labeled the ‘reward pathway’ • This reward pathway is activated by: - Food, water and sex, activities (such as sky diving, paragliding etc) and exercise -This reward pathway is also activated by drugs and alcohol Dopamine (Ventral tegmental Serotonin area, nucleus accumbens) •Receptors: •Receptors: D1, D2 •Function: pleasure, euphoria, mood, motor function Cannabinoids •Receptors: CB1, CB2 •Function: Pain, appetite, memory 5HT3 •Function: mood, impulsivity, anxiety, sleep, cognition Opioid peptides (Endorphins, Enkephalins) Nucleus accumbens, amygdala, ventral tegmental area) GABA (Amygdala, bed nucleus of stria terminalis) •Receptors: Kappa, Mu, Delta •Function: pain Glutamate (Nucleus accumbens) In all rewards, dopamine is the final activation chemical Drug Action & Reward Pathway Alcohol •Binds/Inhibit GABAA: Dopaminergic activity is eventually increased in the VTA by inhibiting GABAergic interneurons •Also binds to NMDA, endorphins, activates secondary messages and has direct serotonergic effects Heroin (Opioid) Binds to opioid receptors that inhibit GABAergic neurons that project to dopaminergic neurons in the VTA Methadone and levo-alphaacetylmethadol (LAAM). Naltrexone Naltrexone Cocaine Nicotine Blocks the function of DAT (by binding the DAT and slowing nto icotine replacement producttransport) (such as Activates cholinergic neurons that project to dopaminergic neurons of the VTA patches or gum) or an oral medication (such as bupropion) Intoxication & Withdrawal: Neurotransmitter Involvement Intoxication Dopamine: euphoria Serotonin: elevated mood Opioid Peptides: analgesia, relaxation GABA: decreased anxiety, less panic, relaxation Withdrawal Dopamine: dysphoria Serotonin: dysphoria Opioid Peptides: increased pain GABA: anxiety, panic attacks NPY: stress Dynorphin: dysphoria CRF: stress Norepinephrine: stress Glutamate: hyperexcitability GABA GABA + Alcohol GABA + Alcohol Acute Intoxication Chronic Intoxication Stress: Heart rate Blood pressure Blood glucose Response to stressors Adapted from Koob & Moal, 2006, reprinted with permission No Alcohol The Development of Addiction • The use of the drug of abuse is increased to maintain euphoria or to avoid dysphoria or withdrawal • The number of receptors gradually increases to counter for the continual presence of the drug of abuse • The amount of neurotransmitter gradually decreases through depletion and feedback inhibition • The reinforcing properties of the drug are thus gradually decreased (tolerance) • The need for drug to maintain this new homeostasis is therefore increased (dependence begins) *The resulting behaviours activate the reward pathway and a relationship is developed and becomes dominant. *Behavioural repertoire is narrowed and eventually other important behaviors are ignored (e.g. familial, financial) •The reward and cognitive (decision making systems) are compromised resulting in an imbalance in impusive behaviours (e.g. violence, crime) PFC Amygdala NAc The Development of Addiction: Long Term Changes There is evidence of prolonged drug abuse resulting in both structural and functional brain changes Decreases in CREB transcription factor in NAc (and extended amygdala) Decreases in metabolism in Orbito Frontal Cortex (OFC) Decreases in dopamine D2 receptor binding (see figure below) Volkow et al. Synapse 14 (2), 1993, pp. 169-177. © 1993 Synapse. Reprinted with permission of John Wiley & Sons, Inc. The Development of Addiction: Long Term Changes Dopamine transporter (DAT) binding following heavy methamphetamine (METH) use Control METH user Volkow et al. Am. J. Psychiatry 158(3), pp. 377-382, 2001 Reprinted with permission from the American Journal of Psychiatry (Copyright 2001). American Psychiatric Association. The Development of Addiction: Genetics Inheritability has been found to range from 40-60% Some variability between: gender and substances Specifically: 4-fold increased risk in 1st degree relatives 4-fold increased risk also in adopted away children The Development of Addiction: Genetics Polymorphism is an altered base pair sequence (altered mRNA = altered protein = altered function) Polymorphisms may - alter synthesis of dopamine - alter neurotransmitter release which may diminish function of prefrontal cortex and exaggerate amygdala Functional consequences relating to addiction include altered: initial response to intoxication, tolerance development, withdrawal effects, psychiatric comorbidity Goals of Drug Treatment: Keeping an Eye on the Target Functionality in Family, Work, and Community Drug Abuse Treatment Core Components and Comprehensive Services Medical Financial Housing & Transportation Core Treatment Intake Assessment Child Care Treatment Plans Group/Individual Counseling Abstinence Based Pharmacotherapy Mental Health Urine Monitoring Case Management Continuing Care Self-Help (AA/NA) Family AIDS / HIV Risks Vocational Legal Etheridge, Hubbard, Anderson, Craddock, & Flynn, 1997 (PAB) Educational When to Consider Pharmacotherapy Assess Pt For: • Severity of Concomitant Medical Illness: Patient’s ability to tolerate medication? • Pregnancy: opioid therapy should be offered to pregnant opioid/heroin addicts; medications that can be associated with adverse physical effects should be avoided (e.g.: disulfiram (Antabuse) • Phase of Recovery: Medications for medical withdrawal or medication to assist with maintenance of abstinence following withdrawal Phases of Substance Use that are Targets for Pharmacotherapy • intoxication/overdose • withdrawal/detoxification • abstinence initiation/use reduction • relapse prevention • sequelae (psychosis, agitation, etc.) Substances for which Pharmacotherapy is Available • Opioids • Alcohol • Benzodiazepines Substances for which Pharmacotherapy is Not Available • Cocaine • Methamphetamine • Hallucinogens • Cannabis • Tobacco (nicotine dependence) • Solvents/Inhalants PHARMACOTHERAPIES Opioid Addiction › Methadone › Buprenorphine › Naltrexone Tobacco Addiction Alcohol Addiction › Naltrexone › Acamprosate (Campral®) › Disulfiram (Antabuse®) › Topiramate (Topamax®) › Nicotine Replacement Therapy (NRT) Electronic Cigarettes, gum, patches Bupropion (Zyban®) › › Varenicline (Chantix®) Lori L. Phelps California Association for Alcohol/Drug Educators, 2013 Similarities & Differences Alcohol Intended Intoxica W/d – detox effect tion 4-12n hrs. p last drink Course hand tremor, AlcoholCNS Depressant/ relaxation, loss of inhibition sweating Slurred speech; Relapse Prevention loss of *Disulfiram coordinati *Naltrexone (oral and injectable)on; mu blocker *Acamprosate ataxia; (↓glutamate decreased release ) coordinati *to help sleep Consider low dose on, trazodone (e.g. attention/ 25 mg) or qHS concensedating anti Depressant tration, (especially if pt has co-morbid depression, memory e.g.:mirtazepine). judgment Sedatives /Hypnotics Anxiolytics Induced effect Benzodiazapi nes& Barbituates Use: to produce Drowsiness, anxiety IntoxBenzo’s rarely fatal when taken alone; sx’s = Lethergy, Confusion; Barb’s –fatal in OD-coma,resp – cardiac arrest W/d – detox Ativan-10 hrs W/d sx’s-6-8 hrs p last dose Valium –w/d up to 1 wk W/d= v/s Need to taper off drug Stimulants amphetamines/cocaine Intended effect Excite – CNS Limited clinical use – high abuse potential Cocaine-highly addictive IntoxHigh-euphoric feeling;hyperactivity/vigilance Talkativeness, grandiosity,hallucin ations, anxiety Repetitive behaviors, anger , fighting W/d – detox Occurs-few hrsdays C/b marked dysphoria; fatigue; vivid & unpleasant dreams; hyper or insomnia; psychomotor act. Opioids: morphine, heroin, meperidine, codeine, hydromorphone, Induced effect Intox – develops Popular for quickly c/b apathy, abuse – lethergy,listless desensitize user to both ness,judgment physio/psych , psycho-motor pain-induce retardation or agiation, euphoria, constricted well-being pupils,slurred speech Severe o d coma, Resp. arrest/death W/d detox: Drug intake ceases or markedly; c/b Anxiety /restless., aching back ,legs, craving for opioids Heroin –w/d 6-24 hr; peak 2-3 days; Ends=5-7 days •Long acting mu agonist (Methadone ;Buprenorphine ) •Naltrexone Hallucinogens Intended effect Distort users perception of reality Intoxification/OD Intox= (Psychologic) anxiety,depression, Paranoid delusions, hallucinations (Physio) B/P,T,P dilated pupils,sweating, blurred vision,tremors, decreased coordination Withdrawal/Detox No withdrawal symptoms known -may crave drug Produce flashbacks May continue up to 5 years after use. Drug Action: Direct e.g. Cocaine •The mechanism of action for cocaine is via reuptake inhibition of dopamine •Dopamine release is promoted via the protein responsible for the reuptake of dopamine (dopamine transporter; DAT) Cocaine binds DAT = extracellular dopamine Thank you