DNP Capstone Project Summary
advertisement

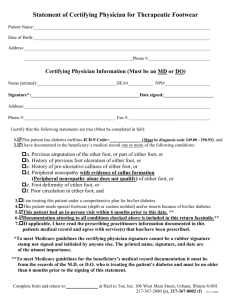
Development of Assessment Tool to Assist with Prevention and Identification of Charcot Foot in Type 2 Diabetics Louise Wade MSN, RN DNP Student Walden University Learning Objectives At the end of the presentation, learners will be able to: Identify and discuss the problem, which is the need for a Charcot foot assessment tool Discuss the relevance of accurate diagnosing of Charcot foot to nursing practice Discuss the IOWA model of evidence-based practice in the identification and treatment of Charcot foot Discuss the American Diabetes Association (ADA) guidelines for treatment of Charcot foot Impact of Type 2 DM According to the World Health Organization [WHO] (2013), 347 million people worldwide have type 2 diabetes and in 2004, an estimated 3.4 million people died from consequences of high fasting blood sugar. Diabetic neuropathy is the most common complication of type 2 diabetes mellitus and affects up to 50% of all diabetic patients and may lead to Charcot foot, which involves the soft tissue and bones of the foot and ankle and leads to permanent deformities. Diagnosing Charcot Foot Diagnosis can sometimes be difficult due to the potential of mimicking other conditions like cellulitis or deep venous thrombosis, and because diagnosis of a Charcot fracture cannot be made definitively until bone changes occur. The problem addressed in the proposed project is inconsistency of healthcare providers in the recognition and referral of patients with potential Charcot foot DNP Project Goals and Objectives GOAL: Improve consistency of healthcare providers in the recognition and treatment of patients with or at risk of Charcot foot. Objectives: 1. Develop an assessment tool and integrate policy and practice guidelines set forth by the American Diabetes Association 2. Educate health care providers in identifying, assessment, treatment, and referral of patients with Charcot foot. Implications for Social Changes Accurate assessment of the diabetic foot is a complex process requiring skill, experience, and knowledge of not only the disease but also signs and symptoms of potential complications. The loss of sensation due to peripheral nerve damage makes it difficult for providers to diagnose issues as well as unseen internal problematic issues such as destruction of bone tissue and cartilage as a result of uncontrolled hyperglycemia. Diagnosing Charcot Foot According to Zgonis (2010), there is a limited amount of scientific literature in regard to treatment protocols and guidelines for management of Charcot foot and ankle deformities and may be in part due to the presence of each individual case of Charcot of the foot and ankle. While many patients present with obvious deformities, there are a higher number of those who have, little, or vague complaints, which adds to the difficulty of accurate diagnosing for the practitioner. Limitations Limitations of this project pertain to the willingness of all stakeholders to participate in the change. Stakeholders are much more likely to support the evaluation and act on the results and recommendations if they are involved in the evaluation process” (George, Daniel, Frankish, Herbert & Bowie, n.d.). The identified stakeholders for this project include health practitioners who are completing the diabetic foot assessment. Relevance to Nursing Practice According to Rogers et al (2011), “the Charcot foot in diabetes poses many clinical challenges in its diagnosis and management. Since undiagnosed Charcot can lead to serious complications including infection, deformity, amputations, disability, loss of employment, financial and mental strains, and life-long devastating effects, it is crucial for practitioners to be knowledgeable and skilled in assessment and treatment methods. Review of Literature According to O’Rourke (2010), from 1999-2008 of patients who underwent either a below or above the knee amputation, 60% suffered from diabetic neuropathy and had some type of trauma, nonhealing wound or other complication such as Charcot foot. Mumoli & Camaiti (2012) discussed a case of Charcot in which a 59 yearold male presented with complaints of a plantar ulcer for two months but after examination, his healthcare provider discovered that his foot was also deformed; however, the patient had such severe neuropathy that he felt no pain at all. According to Jackson (2011), many diabetic patients with existing neuropathy may present with other distracting issues such as foot ulcerations, swollen extremities, or have no complaints of pain or discomfort at all. Evidence-based Practice Model IOWA Model of Evidence Based Practice The Iowa model begins with a trigger or identified problem, which may also be a knowledge-based problem and involves the development of a team of stakeholders and a practice change is developed, implemented, and evaluated (Malone & Bucknall, 2013, 139). Prevalence and Incidence According to the American Diabetes Association, 60–70% of people with diabetes develop peripheral nerve damage that can lead to Charcot foot and about 0.5% of these patients develop the condition. In most cases, onset occurs after the age of 50 and after the patient has had diabetes for 15 to 20 years (Peng & Swierzerswki, 2011). Treatment GOAL: Stabilize the joints American Diabetes Association Recommendations The ADA recommendations are based on expert opinion and are available for access in Diabetes Care (Rogers et al, 2011). Summary Charcot is a major health issue affecting an infinite number of patients each year, many of whom have never heard of it and are unaware of its overwhelming and destructive potential. Prevention and early detection are the keys to avoiding such effects. DNP Project Process Steps 1. Assemble interdisciplinary project team stakeholders 2. Review of best practices of diabetic foot assessment as presented in evidence-based literature. 3. Integration of ADA policies and practice guidelines for assessment, treatment, and referral of the diabetic patient with, or at risk for developing, Charcot foot in conjunction with project team. 4. Development of assessment tool of the diabetic foot in conjunction with the project team 5. Obtain permission to conduct the project from institutional review boards 6. Development and implementation of plan in collaboration with project team 7. Development of evaluation plan in collaboration with project team CHARCOT FOOT ASSESSMENT AND SCREENING TOOL Patient _________________________________ DOB________________Age________________ Insulin____________________ Diabetes Type ________Duration____________ Oral______________________ PCP____________________________________ Management Diet Control________________ Height___________Weight_________________ BP___________Latest HgAIC________________ SKIN Turgor________________________________________Color___________________________________Temperature________ ___________________________Nails___________________________________Calluses________________________________ _______Other___________________________________ SENSORY RIGHT FOOT Sensation : Present_______Absent__________ Numbness/Tingling Yes____No______ Burning Yes____No______ Sharp Pain Yes____No______ LEFT FOOT Sensation: Present________Absent_________ Numbness/Tingling Yes____No_____ Burning Yes____No_____ Sharp Pain Yes____No_____ VASCULAR RIGHT FOOT Pedal pulse: Present_______Absent_________ Edema: None____1+____2+____3+____4+____ LEFT FOOT Pedal Pulse: Present_______Absent_________ Edema: None____1+____2+____3+____4+____ WOUNDS RIGHT FOOT Ulcer Yes____No________ Description (approximate size in mm)________ _______________________________________ DEFORMITIES RIGHT FOOT Bunion Yes_____No_________ Corns Yes_____No_________ Arch intact Yes_____No_________ Other ___________________ LEFT FOOT Ulcer Yes_____No_________ Description(approximate size in mm)_________ _______________________________________ LEFT FOOT Bunion Corns Arch intact Other Yes_____No_______ Yes_____No_______ Yes_____No_______ _________________ RISK LEVEL Low Risk_______ No sensory loss, ulcerations, or deformities Treatment: Annual Assessment Moderate Risk________ Altered sensory, minimal structural deformity, or beginning onset of ulcerations Treatment: Refer to Podiatry High Risk________ Impaired sensory, + numbness/tingling, healed or active ulcerations, amputation, deformities Treatment: Refer to Podiatry REFERRAL Name of Podiatrist______________________________Date Contacted____________________ Person making referral__________________________Appointment Date__________________ Special instructions or treatment given by podiatrist_________________________________________________________________________________________________ Signature of Provider________________________________Date_______________________________ Implementation * Assessment tool presented to members of area nurse practitioner group at annual NP symposium. * Education for NPs and clinic staff * Assessment tool integrated into electronic medical record (EMR) as reminder for practitioners to complete and initiate treatment as indicated. Evaluation 1. 2. Evaluation is tentatively scheduled after a 3-6 month assessment trial period to include key stakeholders of the project The evaluation plan for this project will involve both a verbal and written formal process in the form of an electronic anonymous survey Project Summary Prevention of Charcot foot is an important aspect of assessment in the diabetic population and more importantly, in patients suffering from peripheral neuropathy. The ability to rapidly and accurately identify risk factors, signs and symptoms, and appropriately treat this serious complication of diabetes is a significant measure in preventing life-threatening injuries References George, A., Daniel, M., Frankish, C. J., Herbert, C. P., & Bowie, W. R. (n.d.). Introduction to Program Evaluation for Public Health Programs. Retrieved from http://www.cdc.gov/getsmart/program-planner/Step1.pdf Jackson, K. (2011, March 1). Charcot Neuroarthropathy. Retrieved from http://nursing.advanceweb.com/Regional-Content/Articles/CharcotNeuroarthropathy.aspx Malone, R., & Bucknall, T. (2013). Models and frameworks for implementing evidence-based practice: Linking evidence to action. (1st ed., pp. 137-146). Malden, MA: Wiley-Blackwell Publishing. Retrieved from http://books.google.com/books?hl=en&lr=&id=iFFBt_PULWcC&oi=fnd&pg=PR3&dq =Iowa model of evidence based practice in nursing&ots=nDvfGINa7w&sig=C3SdnXCqyW8vm9iCsUF2e5xgu0 Mumoli, N., & Camaiti, A. (2012). Charcot Foot. Canadian Journal of Medicine, 184(12). Doi:10.1503/cmaj.111972 References Continued O’Rourke, I. (2010). Model of care for the high risk foot. ANZ Journal of Surgery, 72(4), 286. Retrieved from http://www.healthnetworks.health.wa.gov.au/modelsofcare/docs/High_Risk_Foot_Mod el_of_Care.pdf Peng, H., Swierzewski, S., & (2011, May 23). Charcot foot overview. Retrieved from http://www.healthcommunities.com/charcot-foot/charcot-foot-overview.shtml Rogers, L., Frykberg, R., Armstrong, D., Boulton, A., Edmonds, M., Ha Van, G., & Hartemann, A. (2011). The Charcot foot in diabetes. Diabetes Care, 34(9), 2123-2129. Doi: 10.2337/dc11-0844 World health organization: Diabetes fact sheet. (2013, October). Retrieved from http://www.who.int/mediacentre/factsheets/fs312/en/ Zgonis, T. (2010). How To Manage The Charcot Midfoot Deformity. Podiatry Today, 23(7), 68-75. Retrieved from http://www.podiatrytoday.com/how-manage-charcot-midfoot-deformity