(GIB) and Subsequent Endoscopic Therapy after Implantation of Left
advertisement
 and Subsequent Endoscopic Therapy after Implantation of Left")
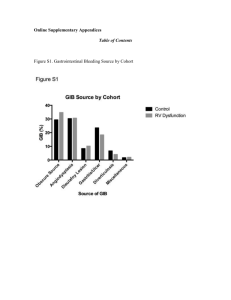
Characteristics of Gastrointestinal Bleeding (GIB) and Subsequent Endoscopic Therapy after Implantation of Left Ventricular Assist Device (LVAD) for End Stage Heart Failure Sandeep Mahajan, David T. Majure, Amir Taefi, Julio Salcedo, Maria E. Rodrigo, Mark Hofmeyer, George Ruiz, Ezequiel J. Molina, Steven W. Boyce, Samer S. Najjar, Farooq H. Sheikh Digestive Disease Week May 16th, 2015 LVAD Therapy Improves Survival in Advanced Heart Failure (AHF) Patients Rose et al., N Engl J Med. 2001;345:1435-43. Continuous Flow LVADs HeartMate II HeartWare GI Bleeding and LVAD Therapy ~15-30% of LVAD recipients develop GIB1-3 Multiple mechanisms of bleeding have been postulated including: 1. 2. 3. Acquired Von Willebrand Syndrome Chronic low pulse pressure (resulting in AVM formation) Need for chronic anticoagulation 1. Boyle et al. J Am Coll Cardiol 2014;63:880-8. 2. Goldstein et al. J Am Coll Cardiol HF 2015;3:303-13. 3. Uriel et al. J Am Coll Cardiol 2010;56:1207-1213. Purpose To characterize GIB events in LVAD recipients implanted with one of two FDA approved LVADs at our institution Thoratec HeartMate II, HMII HeartWare HVAD Methods Single center retrospective review of patients implanted with a LVAD (MedStar Washington Hospital Center) Study period – 1/1/2011 – 10/27/2014 GIB defined as melena, hematochezia, hematemesis, or anemia requiring endoscopy Methods (cont’d) We characterized GIB events by: 1. 2. 3. 4. Presenting signs or symptoms Location and type of lesion Type of endoscopy performed Type of endoscopic therapy provided Results Study Characteristics Number of patients - (no.) 170 Total follow up – (patient years) 153 Incidence of GIB – (no.) % 35 (21) Number of GIB events – (no.) 73 Incidence GIB rate - (events per patient year) 0.22 Overall GIB event rate – (events per patient year) 0.39 Median time to first GIB event (months) HMII HVAD 8.2 ± 3.5 3.5 ± 0.98 (p = 0.07) Results (cont’d) Frequency of GI Hemorrhages HMII HVAD 100 Frequency of GI Hemorrhages 80 40 60 74.24 20 Percent of Patients 82.69 16.67 4.545 2 3 7.692 1.515 4.808 .9615 1.923 1.923 4 5 0 3.03 0 1 4 5 6 0 1 2 3 Number of GI Hemorrhages Graphs by type of LVAD 9% of HMII and 10% of HVAD patients experienced more than one GIB 6 Results (cont’d) Baseline Demographics of the GIB Study Patients (N = 35) Age (years) 59 ± 11 Sex – no. (%) Male Female 26 (75) 9 (25) Race – no. (%) African American Caucasian Other 25 (71) 9 (26) 1 (3) BMI - median 27 ± 5 Ischemic Cardiomyopathy – no. (%) 14 (40) Diabetes – no. (%) 13 (37) CKD > Stage 2 – no. (%) 13 (37) Smoker (ever) – no. (%) 22 (65) History of GIB prior to LVAD implantation 1 of 35 Results (cont’d) Anticoagulation and presenting INR of all GIB events (N = 73) On Warfarin Total On ASA No Yes No 10 17 27 Yes 4 42 (58%) 46 (63%) Total 14 59 (81%) 73 Mean INR on admission - 2.56 ± 2.07 Mean INR at the time of GIB did not differ between the 2 LVAD groups Results (cont’d) Presenting symptoms of all GIB events– No. (%) Melena 34 (46) Anemia 31 (42) Hematemesis 4 (6) Hematochezia 4 (6) Results (cont’d) A culprit lesion was identified in only 47 of 73 GIB events (67%) Type of GIB identified - No. (%) Angioectasias/AVM 40 (85) Ulcer 3 (6) Gastritis/Duodenitis 3 (6) Polyp 1 (2) Hemorrhoidal 0 (0) Diverticular 0 (0) Characteristic Image of AVM Results (cont’d) Esophagus = 0 Stomach - Fundus = 4 - Body = 16 (34%) - Antrum/Pylorus = 6 Small Intestine - Duodenum = 4 - Jejunum = 9 (19%) - Ileum = 0 - Cecum = 3 Colon - Colon = 5 - Rectum = 0 Results (cont’d) Types of procedures of all GIB events Time to Endoscopy – mean (days) 2.56 ± 2.85 EGD – no. (%) 66 (90) Colonoscopy – no. (%) 33 (45) Enteroscopy – no. (%) 36 (49) Video Capsule Endoscopy – no. (%) 5 (7) Results (cont’d) Type of intervention with culprit lesions (N = 47) Argon Plasma Coagulation – no. (%) 38 (81) Cautery – no. (%) 4 (9) Clipping – no. (%) 1 (2) Polyp resected – no. (%) 2 (4) None – no. (%) 2 (4) Limitations Single center Retrospective review Use of antiplatelet therapy differs between the 2 LVAD devices at our center Conclusions are dependent on the accuracy and completeness of the recorded events Conclusion GIB is a common complication of LVAD therapy which frequently necessitates upper endoscopy Angioectasias/AVM are the most common lesions found Gastric body is the most common site of GIB in our cohort Bleeding source could not be identified in up to 33% of cases Future Directions Future studies should evaluate optimal strategies for identifying the source of bleeding – standardized protocols Success of primary endoscopic therapy New investigational LVADs (introduction of pulsatility) Thank You Dr. Farooq Sheikh Dr. David T. Majure Dr. Samer Najjar Dr. Julio Salcedo Dr. Amir Taefi