HIV and AIDS

Good Morning!
Counseling, Bereavement and the Emotional Impact on those living with and affected by HIV and AIDS
Overview
Part I Counseling and Disease Continuum
Part II Some Insights on Bereavement
Assistance for people living with
HIV/AIDS and
Part III Emotional Impact on the Infected and the Affected;
Caring for the Dying/Grieving
Part IV Theology: HIV and AIDS
3
Counselling Issues Across the
HIV Disease Continuum
World Health Organization Module 4 Sub Module 1
– PPT25
Session
Objectives
Counselling
Issues
Across the
HIV Disease
Continuum
Identify common psychosocial issues of clients living with HIV
Identify the link between VCT and treatment and care
Describe the continuum of care
Identify the interrelationship between disclosure, stigma and discrimination
World Health Organization Module 4 Sub Module 1
– PPT25
Psychosocial
Issues
Counselling
Issues
Across the
HIV Disease
Continuum
Consideration of psychosocial issues is fundamental to HIV / AIDS counselling & care
Counsellors need to view the client in a holistic manner within the context of their social environment
A range of issues can be experienced by clients
Different clients experience different issues
– no two people are the same
Issues can change across time & with disease progression
World Health Organization Module 4 Sub Module 1
– PPT25
Common Key
Issues
Counselling
Issues
Across the
HIV Disease
Continuum
Confidentiality
Difficulty accepting diagnosis
Disclosure
Discrimination and stigma
Emotional reactions – shock, denial, depression, anger, fear, guilt, depression, anxiety, suicidal thoughts
World Health Organization Module 4 Sub Module 1
– PPT25
Common Key
Issues
Counselling
Issues
Across the
HIV Disease
Continuum
Disease progression
Changes in physical appearance
Illness/deterioration in health
Loss of control
Death and dying
Loss and grief
World Health Organization Module 4 Sub Module 1
– PPT25
Common Key
Issues
Counselling
Issues
Across the
HIV Disease
Continuum
Relationships – partner, family, friends, child(ren)
Financial difficulties
Welfare – income/employment/housing
Sexual difficulties
Employment difficulties/loss of job
Treatment issues – access, adherence, sideeffects
World Health Organization Module 4 Sub Module 1
– PPT25
Interventions for
Psychosocial
Issues
Counselling
Issues
Across the
HIV Disease
Continuum
Psychosocial care encompasses a range of interventions that address the social & psychological issues & needs of PLWHA & their significant others
Interventions can assist clients to:
- Develop a support network
- Experience autonomy
- Gain a sense of control
Counsellors play an integral role in facilitating interventions & care across the
HIV disease continuum
World Health Organization Module 4 Sub Module 1
– PPT25
Possible
Interventions
Counselling – individual, couple, family, pastoral, group, community
Support groups & peer support networks
Emotional & spiritual support
Economic support/welfare interventions
Counselling
Issues
Across the
HIV Disease
Continuum
World Health Organization Module 4 Sub Module 1
– PPT25
Possible
Interventions
Counselling
Issues
Across the
HIV Disease
Continuum
Medical interventions/symptom management
Pharmaceutical management
Regular health checks
Nutritional care
Palliative care
World Health Organization Module 4 Sub Module 1
– PPT25
Possible
Interventions
Counselling
Issues
Across the
HIV Disease
Continuum
Home-based care
STI care
Family planning services
Community activities
Assistance to orphans & other vulnerable children
World Health Organization Module 4 Sub Module 1
– PPT25
Counselling
Issues
Across the
HIV Disease
Continuum
VCT is an entry point for HIV prevention, treatment & care
World Health Organization Module 4 Sub Module 1
– PPT25
The HIV / AIDS
Continuum of Care
Counselling
Issues
Across the
HIV Disease
Continuum
VCT is the entry point
Proposes a range of interventions
Incorporates a range of different people, resources and services
Includes hospital care, community and home care over the course of the illness
Provides comprehensive and holistic care for PLWHA and their significant others
World Health Organization Module 4 Sub Module 1
– PPT25
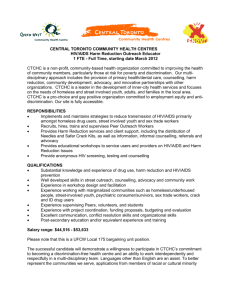
Prevention
Care
Continuum
Service
Continuum
Voluntary
Counselling
Testing
Secondary
Health
Care
District
Hospitals
HIV Clinics
Social/legal
Support
Hospice
Counselling
Issues
Across the
HIV Disease
Continuum
The entry point
Specialists and
Specialised
Care facilities
Tertiary Health
Care
Primary Health
Care
Health posts
Dispensaries
Traditional
Orphan care
Community Care
NGOs
Churches
Youth Groups
Volunteers
PLWHA
Peer support
Palliative emotional and spiritual support self care
Home care
World Health Organization Module 4 Sub Module 1
– PPT25
AN ACTIVITY
17
The person
I love most
18
My greatest value as a person
19
My greatest dream in life
20
Some Insights On Bereavement
Assistance on PLWHA
21
Questions on our mind…
22
How do you actually feel about dying?
23
Are you afraid of dying?
Or are you afraid of the unkown ?
24
Do you think seriously about your tomorrow, or even today?
25
What do you think you ought to do in preparation for your death?
forward to it?
26
Are you willing to entrust your body, mind and spirit to your
God?
27
Take a deep breath…
28
Definition of Bereavement
29
Bereavement
• The objective state of having lost someone or something precious; the objective situation of individuals who have experienced a loss.
• Refers to the particular grief that accompanies and is evoked by the death of a loved one.
Grief
• Refers to the psychological process of adjustment to any substantive loss or change
• Grieving is about the natural response of people to all types of life crises—death, divorce, unemployment or retrenchment, loss of health, limbs or physical disappearance, loss of purpose and self-esteem; loss of anyone or anything we value.
31
Mourning
• Represents the culturally defined acts that are usually performed after a death
• Sorrow or regret expressed through customs and conventions
Bereavement Assistance
Bereavement Assistance
HIV-AIDS Bereavement in contrast to Cancer Bereavement
Levels of Grief
Traumatic stress
Grief-related depression symptoms
Anxiety, depression, somatic symptoms
Social Dysfunction
Lower level of social support
More likely to hide the cause of death
Greater level of rejection
Refuge from “support groups” than family
34
Purpose of Bereavement Assistance
• Infected
Acceptance of one’s situation / Integrate in the daily undertakings
Management of Infection
Eliminate adverse psychological burdens
Make plans on how to live with the virus
Enhancing Quality of life
35
Purpose of Bereavement Assistance
• Affected
Recognition and acceptance of the reality of loss
Management of painful memories
Eliminate adverse psychological burdens
Coping with situational lifestyle changes resulting from loss
Adapting to the loss, and reconfiguring their own life
36
Phases of Reaction to HIV/AIDS
A General Sense of Loss
physical ability
cognitive ability (thinki ng)
home, work
social status and suppo rt
sense of the future
faith, hope, and a sense of God’s care
Caitlin Ryan, Recommendations for a Support and Management
Plan for People with AIDS and HIV Infection in the Republic of Korea (February 1990)
38
Reactions to HIV/AIDS
Initial Response
Shock
Range of Emotions: confusion, despondency
Difficulty in comprehending diagnosis
Beginning to mobilize resources
Caitlin Ryan, Recommendations for a Support and Management Plan for People with AIDS and HIV Infection in the Republic of Korea (February 1990)
39
Reactions to HIV/AIDS
Adaptation Stage
Range of emotions: fear, sadness, guilt, anger, depression, etc.
Possible displacement of anger by acting out (placing others at risk for infection)
Beginning to cope with health status
Dealing with stigma and need to manage information about HIV status
Increased dependency
Caitlin Ryan, Recommendations for a Support and Management Plan for People with AIDS and HIV Infection in the
Republic of Korea (February 1990)
40
Reactions to HIV/AIDS
Integration Stage
Learning to live with chronic illness
Feeling a broad range of emotions which may not be understood by family and friends
Grieving cumulative losses
Coping with increasing health crises
Continuing risk reduction and management of stress
Exploring spiritual concerns
Re-negotiating relationships
Caitlin Ryan, Recommendations for a Support and Management Plan for People with AIDS and HIV Infection in the Republic
of Korea (February 1990)
41
Reactions to HIV/AIDS
Stage of Advanced HIV-disease
• Need to cope with continued and worsening health crises
• Loss of body control, disfigurement, possible dementia
• Facing death and dying
Caitlin Ryan, Recommendations for a Support and Management Plan for People with AIDS and HIV Infection in the Republic
of Korea (February 1990)
42
Understanding the Stages of
Bereavement
43
Bereavement Stages
STAGE 1: Acclimation and Adjustment
Adjusting to changes brought by the loss
Functioning appropriately in daily life
Keeping emotions and behaviours check
Accepting support
Phil Rich Ed. D., MSW, The Healing Journey Through Grief (January 1999)
44
Stages of Bereavement
STAGE 2: Emotional Immersion and Deconstruction
Contending with reality
Development of insight
Reconstructing personal values and beliefs
Acceptance and letting go
Phil Rich Ed. D., MSW, The Healing Journey Through Grief (January 1999)
45
Stages of Bereavement
STAGE 3: Reclamation and Reconciliation
Development of social relations
Decisions about changes in lifestyle
Renewal of self-awareness
Acceptance of responsibility
Phil Rich Ed. D., MSW, The Healing Journey Through Grief (January 1999)
46
HIV/AIDS and Suicide
Persons living with HIV/AIDS may experience thoughts about suicide, especially when they are first informed about HIV infection or when first admitted to hospital for AIDS-defining illness.
Possible signs of that suicide is being considered:
• Previous attempts,
• Verbal or written threats
• Gathering of potentially dangerous items,
• Giving away valuables
• Extreme sadness,
• Withdrawal from family & friends, sudden mood elevation
Source: Communities of Care Team Manual (Third Edition), AIDS Pastoral Care Network, Chicago,
Illinois
47
HIV/AIDS and Suicide
Ways to offer help …
Take talk of suicide very seriously - get help fast!
Listen … Loved ones may be afraid to talk with person about these things.
Don’t be afraid to ask questions - keep talking until person calms down - that gives you time to get help
Encourage the person to get professional help.
Source: Communities of Care Team Manual (Third Edition), AIDS Pastoral Care Network, Chicago,
Illinois
48
Caring for the Dying
49
What are your reactions to the following statements: agree or disagree?
50
Examine your own Attitude / Paradigms
People with AIDS are to be blamed for bringing this disease on themselves.
51
Examine your own Attitude / Paradigms
• The AIDS epidemic could be stopped if laws against prostitution and homosexual behavior were made stronger and if
“foreigners” were sent home.
52
Examine your own Attitude / Paradigms
• People with HIV and AIDS should have the same rights as other persons.
53
Examine your own Attitude / Paradigms
Men who have sex with men indulge in abnormal sexual behavior.
Examine your own Attitude / Paradigms
All health care workers should be tested for HIV antibodies and removed from practice if found to be positive.
Identifying the Needs of the Dying and Caring for the Dying
56
“a companion unto death”
Dying is a psycho-social, biological and spiritual process. The person going through this process is also considering in some way or another, the meaning of one’s having been in the world, being in the world, and now leaving the world . In this process the person goes through a series of intense feelings and reactions, and as caregivers we should be capable of observing and dealing with them comfortably.
57
Companion
Expression of Feelings
A companion sits and LISTENS, and encourages expression of these feelings, accepting them as they are.
We may have to work as mediators for the family in guiding them as well.
58
Companion
Overcoming Loneliness
SITTING with them, and encouraging family members to sit with the dying person. Remember, it’s terrible to “die alone”.
59
Companion
Give meaning to their past lives
Helping the person to review their life, especially helping them to recognize that they have not lived their lives in vain, however small their “successes” might be.
Focus on meaning and purpose of their life.
60
Companion
Finding Meaning in the Present Moment
Participate with the dying in their struggle to find meaning in the present process of dying.
61
Companion
Need to let go of life
Loosening of personal ties, pulling back, withdrawing, less intensity, etc. Companions/ Caregivers must assist the dying and the family in this delicate process of letting go.
62
Companion
The need to deny death
The counsellor must be aware of the dying person’s need to deny the finality of sickness from time to time. Even after they have accepted the reality, it’s important to let them use denial because the thought if death and family is just too much to accept. Never force the reality check on them.
63
Other religious/existential needs
• The need for meaning and purpose
• The need to give love
• The need to receive love
• The need for hope and creativity
• The need to relate with God
64
Fears of Dying
PROCESS OF DYING
MEANINGLESSNESS LOSS OF CONTROL
DEATH
LOSS OF LOVED
ONES
UNKNOWN
ISOLATION OTHER’S REACTION
65
Faith in the after life
66
The Catholic Church on HIV and
AIDS Prevention
67
Basic Guiding Principles
•
Human Dignity
[The value and dignity of human person]
•
Solidarity
[The rights and responsibilities of society]
•
Grace
[The love and compassion of God)
68
The approach of the Church is guided by a precise and all-rounded view of a human being ‘created in the image of God and endowed with a God-given dignity and inalienable human rights.’
69
HUMAN DIGNITY
In the Gospels, Jesus not only physically cured leprosy patients, the paralytic and the woman with haemorrhage, but he also restored in them human dignity and their rightful place in the community.
70
HUMAN DIGNITY
Every human being is created in
God’s image, redeemed by Jesus, and called to everlasting life.
71
HUMAN DIGNITY
All of us are called to live in ways that embody and express this dignity.
There is then a serious call for personal responsibility and to personal behaviour change .
72
SOLIDARITY
The Church’s teachings speak extensively about the rights and the responsibility of the society.
73
SOLIDARITY
"A comprehensive AIDS education then has to place
AIDS within a moral context; impart accurate medical information and challenge misinformation; motivate individuals to accept the responsibility for personal choices and actions; confront discrimination and foster the kind of compassion which Jesus showed to others; model justice and compassion through policies and procedures."
(New Mexico Bishops, 1990)
74
"While preaching a Gospel of compassion and conversion, Jesus also proclaimed to those most in need the Good News of forgiveness. The father in the parable of the prodigal son did not wait for his son to come to him. Rather, he took the initiative and ran out to his son with generosity, forgiveness, and compassion."
75
GRACE
"The love of God is so great that it goes beyond the limits of human language, beyond the grasp of artistic expression, beyond human understanding . . . . [God] loves us all with an unconditional and everlasting love"
(Pope John Paul II)
76
GRACE
Jesus has revealed a God who loves each of us unconditionally, a God who forgives our sinful actions. God is not vengeful. God respects human freedom, calling us to love and responsibility, but not interfering even with destructive choices.
77
Pope John Paul II cautioned young people about the myth of “safe sex”
“Do not let yourselves be led astray by those who ridicule your chastity or your power to control yourselves. The strength of your future married love depends on the strength of your present effort to learn about true love. Chastity is the only safe and virtuous means to put an end to the tragic plague of
AIDS. ”
Documentation Catholique, No. 2068, 21 March 1993, p. 262.
78
Church’s teaching in the external forum and formation of conscience in internal forum
“We too preach the gospel, but we try above all to form consciences” [1]
Discernment of right or wrong in human acts, including those related to prevention of HIV:
• must take place with the benefit of Church’s teaching on right values related to individual behavior as well as to the common good
• with support and counseling to hear the “voice of God” echoing in one’s conscience.
[1] Bishop Theodore Adrien Saar, President of Bishops’ Conference of Senegal at International Conference on AIDS in Religion, 1996.
79
Challenges for Pastoral Leaders
The challenges for pastoral leaders are many:
• They often are called upon to accept the affected person’s expression of anger against the Church, the clergy, or God, and then to help the person discern God’s loving care and mercy in all human situations even those which involve illness and loss.
• They are expected to offer pastoral care which goes beyond traditional and familiar formulae for prayer.
• In order to provide compassionate, non-judgmental pastoral care-giving, they need to deal with their own unresolved emotional issues regarding sexuality and around serious illness, death and dying.
Source: Mimi Blum and Robert Vitillo, Training Manual and Resource Guide for HIV/AIDS Trainers/Service Providers, Catholic
Charities USA/University of Texas, Houston (1997): 155.
80
Challenge to the Church by
Persons Living with and Affected by HIV
• Be a true reflection of Christ – for if Christ walked the earth today he would respond to the needs of people living with
HIV and AIDS.
• Be the light of the world, drawing people with HIV to you, not making them to feel guilty and ashamed. We should be drawn to the church.
• Preach and live the gospel.
• We would like the church to be at the frontline in educating people about HIV and AIDS
• Talk about sex and sexuality in church, for God created sex.
Teach about the right context of sex.
• Set an example by going for the test; WALK OUR WALK and know how we really feel.
• Support our initiative as people living with HIV.
81
Source: At Research Feedback meeting, “Churches and HIV/AIDS”, Pietermaritzburg Agency for Christian Awareness, 23 November 2004.
Challenge to the Church by
Persons Living with and Affected by HIV
• Involve us, acknowledge our presence in the church. For we are here in the church, we are Christians – children of God, the Blessed, not cursed.
• Stop preaching about AIDS as a curse.
• The gospel you preach should meet our spiritual needs.
• Create an environment where we can disclose our status.
• Practice confidentiality.
• Love us and create Hope for us.
• Give unconditional LOVE
Source: At Research Feedback meeting, “Churches and HIV/AIDS”, Pietermaritzburg Agency for Christian
Awareness, 23 November 2004.
82
Pope John Paul II urged all to be involved in response to the
HIV pandemic
“ AIDS threatens not just some nations or societies but the whole of humanity . It knows no frontiers of geography, race, age, or social condition… The threat is so great that indifference on the part of public authorities, condemnatory or discriminatory practices toward those affected by the virus or self-interested rivalries in the search for a medical answer, should be considered forms of collaboration in this terrible evil which has come from humanity.”
Pope John Paul II, visit to Tanzania, September 1990
83