Family Assessment: Utilizing the Calgary Family Assessment Model
advertisement

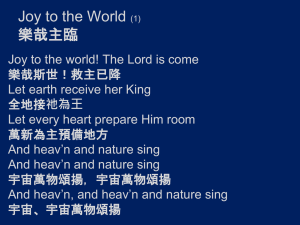
Running Head: FAMILY ASSESSMENT 1 Family Assessment: Utilizing the Calgary Family Assessment Model Stephanie Cheers University of North Carolina Wilmington FAMILY ASSESSMENT 2 Family Assessment: Utilizing the Calgary Family Assessment Model Introduction For the purpose of this assignment a family was interviewed. Upon completion of the family assessment, their weaknesses and strengths were identified. Based on my assessment findings a care plan was developed, and strength based interventions were implemented. The family discussed in this paper is a cohabiting family, which means the couple described lives together but is not married. Included is a mother Joy age 21, a father Thomas age 24 and two children Tyler and Carter whose ages are 3 and 10 months. The children can be described as multi-racial since Joy is Caucasian and Thomas is African American. Thomas and Joy are originally from New York and met in high school six years ago and began to date. Shortly after Thomas graduated high school in 2008 he moved to Wilmington, so he could pursue a career working for his Uncle Jason in the flooring industry. After a few months and struggling to make a long distance relationship work, Joy dropped out of high school at the age of 15 and moved to Wilmington to be with Thomas. Thomas and Joy had a on again, off again rocky relationship and it wasn’t till she got pregnant at the age of 16 that things turned serious. Their first son Tyler was born in 2010, when Joy and Thomas were still just kids their selves at the ages of 16 and 19. Joy took on the role of a stay at home mother and put her dreams of going back and graduating high school on hold. Thomas has continued to work for his uncle in the flooring business, and stays very busy working six long days a week. Thomas provides the sole income for the family. Tyler appears to be a happy and healthy 3 year old, however Joy admits that he has not seen a physician in over two years because they do not have insurance. Tyler attends preschool FAMILY ASSESSMENT 3 three days a week, where he is learning to write his name and speak Spanish. Joy says he is very advanced for a 3 year old. In 2012, Thomas and Joy had a very big surprise – they were pregnant again. 10 month old Carter was born in June of 2013. Carter is healthy and has hit all his developmental milestones thus far. However, while discussing Carter’s health, Joy shared with me she forgot to take him to his nine month old wellness checkup and has been procrastinating to reschedule. Access was gained to this family through my husband whom is also in the flooring business. He is a co-worker of Thomas’s, and had spoken about us donating some of my son’s (who is a few months older then Carter) clothes and toys to the family. He said that Thomas admitted they were struggling to pay the bills, and actually asked my husband for a cash advance so that he could pay for his son’s preschool. After meeting Joy, I knew that she and her family would be great for this assessment project because I could tell there were multiple problems within this family and their dynamics. Joy and Thomas agreed to be interviewed, and shared a lot of personal information with me. This family personally has meaning to me because I hate to see anybody struggling, but especially someone with kids. I have a young child and I know how hard it can be, and how expensive things can get. Academically, I grew and enhanced not only my interview skills but my family assessment skills. I also learned a lot about my own community and the resources that are offered, as well as expanding my knowledge on Obamacare and Medicaid. Family Assessment The Calgary Family Assessment Model (CFAM) helps nurses to organize data, and served as a template for completing this family assessment. CFAM consist of three major categories – structural, developmental, and functional (Wright & Leahey, 2000, p. 67). FAMILY ASSESSMENT 4 Structural Assessment When completing a family assessment, the nurse needs to examine its structure which includes who is in the family, what is the connection among family members, and what is the family’s context (Wright & Leahey, 2000, p. 69). The three aspects of the family structure that can be most readily examined are internal structure, external structure, and context (Wright & Leahey, 2000, p. 69). Internal Structure The family composition of this cohabiting family consists of a mother and father in a monogamous un married relationship with two children and one dog. The mother, Joy is the caregiver, whereas the father Thomas is the financial supporter and ultimate decision maker. There appears to be very rigid boundaries, Joy is the only one who cooks and cleans the house; however this does help to facilitate functioning and may be beneficial towards the family. The two children, Tyler and Carter are both boys, age 3 and 10 months. Tyler has been very accepting of his new brother, and they enjoy spending time together and playing. Several subsystems have been identified and include parent-child, male, female, sibling, caregiver, supporter and girlfriend-boyfriend. The dog Buddha is a large pit mix that mostly stays inside, he does not require much extra attention but he does eat a lot of food which can be expensive. The family cares deeply for Buddha and considers him to be part of their family. External Structure The external family assessment falls into two subcategories, the extended family and larger systems. First, the extended family, which includes generations within the family, is reviewed. Next, larger systems such as social agencies and personnel with whom the family has meaningful contact are identified (Wright & Leahey, 2000, p. 79). FAMILY ASSESSMENT 5 Extended family. The maternal extended family includes three generations. All of Joy’s extended family lives in New York. Joy’s mother, Allison is 40 years old and is overweight. Allison also has a medical history of Bipolar disorder and is a recovering drug addict. Joy has one sister, Susan who is two years older than her who is in good health. Joy is estranged from her father William; he was physically abusive to Allison. Alice is Joy’s grandmother, she is 64. Alice is obese and has high blood pressure, as well as high cholesterol. Joy’s grandfather Robert had high blood pressure but died of lung cancer when he was 63 years old. He smoked cigarettes up until the day he died. Joy states that she is not very close with her family; they are not a good support system and she rarely speaks to them. The paternal extended family offers more support but is still distant. It consists of four generations. Thomas is very close with his brother Luke, age 23 and Cousin Jason, age 37. Both Luke and Jason live in Wilmington. Luke and Thomas work together installing flooring for their cousin Jason. Although Luke suffered from Hepatitis A three years ago he now considers himself healthy. Both Luke and Jason are in good physical condition with no noted health problems. Luke and Jason are the only relatives of Thomas’s that live nearby, the rest are in New York. Thomas is also fairly close with his mother Paula, 50. This is who they look to when they need advice, especially when it comes to the children. Paula does have diabetes, and takes insulin three times a day. Thomas’s father Kenneth, who is 49, is an alcoholic and left Paula and the children when Thomas was just 5 years old. Thomas states he barely remembers his father, but the memories he does have are not good ones. Aside for Luke, Thomas has another sibling Tonya who is 27. Like Thomas, Tonya also has two children out of wedlock. She has a little girl who is 7 named Sarah, and a son named Jacob who is 5. Tonya is no longer in a relationship with the children’s father James, and he is not involved in their lives. Both of Thomas’s maternal FAMILY ASSESSMENT 6 grandparents are deceased. His grandfather David died of a massive heart attack at the age of 70. His grandmother Betty had Alzheimer’s and died a natural death when she was 72. Although, Thomas’s relationship with his extended family is distant, they still provide guidance and support for Thomas and his family. Thomas’s cousin Jason often provides the family with financial assistance. The genogram below provides a visual model of the family and the relationships to each other on a multigenerational spectrum. Genogram Symbols Male 1932 1936 1944 1950 David Betty Robert Alice Female Death 64 1960 1955 54 59 Laura Kirby Family Relationships 7 1965 1964 49 50 Kenneth 1968 Paula 1974 46 40 William Allison 11 1 Obesity 1977 1983 1987 1991 1990 37 31 27 23 24 Jason James Tonya Luke 1993 Thomas 20 23 Joy Susan 1 Alcohol or drug abuse 1 Hepatitis Unw ed Unw ed 1991 1 Cancer, Hypertension / High Blood Pressure 2007 2009 2010 2013 7 5 3 10m Sarah Jacob Tyler Carter Primary Family 1 Diabetes 1 Obesity, Depression 1 Heart Disease, Hypertension / High Blood Pressure, Obesity 1 Alzheimer's Disease 1 Heart Disease 1 Alcoholism Larger systems. Thomas has developed several of his relationships though work. His job serves not only the purpose of providing financial income, but also allows him to socialize. Thomas doesn’t have a lot of free time but when he does he spends it drinking with his friends or FAMILY ASSESSMENT 7 playing video games with his brother. Joy states that with being a stay at home mother she doesn’t have many opportunities to meet people or friends. She has one neighbor, that she is close with, Roseanne. Roseanne is quite a bit older then Joy, she is 40 and serves more of a motherly role then a peer acquaintance. Joy does enjoy taking her son’s to the park down the street. They also seem to enjoy getting out and playing. Joy’s youngest son does receive Medicaid and is able to attend the clinic for his check-ups. However, Joy does not like the doctor there and is looking to switch Physicians. She said that nobody is accepting new patients. Tyler, the three year old attends preschool three days a week which he very much enjoys. He loves going to school to learn and spend time with his friends. The Ecomap bellows depicts the family members contact with lager systems, such as institutions and friendships Spend time with brother Work as flooring installer Drink with friends Spend time with Neighbor Joy 21 Thomas 24 Tyler Carter 3 10m Play/Learn at school Recreation at Park Doctor visits at clinic FAMILY ASSESSMENT 8 Context Assessment The context of a family is explained “as the whole situation or background relevant to some event or personality” (Wright & Leahey, 2000, p. 80). The contextual assessment included five subcategories which are ethnicity, race, social class, religion and environment. Joy is of Caucasian American decent, whereas Thomas is of African American decent. Joy believes that she has some German heritage down the line. Joy states she is Christian and grew up Methodist. Thomas attended Baptist church when he was a young boy, but now has developed agonist beliefs. Although Joy is Christian, she does not claim to be religious. They do not attend church, and neither of the boys has been baptized. They do however celebrate Christian holidays such as Easter and Christmas. I would describe the family as upper-lower class in regards to social class. Thomas graduated high school, but did not pursue college. Joy dropped out of high school at the age of 15, however she dreams of going back to finish high school and then pursuing a career as a nurse. Thomas is a considered a “blue collar worker”, he performs manual labor installing flooring. He works extremely hard, typically six 8-12 hours days a week. Because he works so hard he has a decent income, but still struggles to pay the bills and lives pay check to pay check. Joy mentioned during the interview that she tried to renew Tyler’s Medicare but “Thomas made too much money.” The family lives in nice neighborhood in the suburbs of Wilmington (Ogden). It is a 3 bedroom, 2 bathroom “cookie cutter” house. They rent the home, and have lived there for approximately 1 year. They have a large fenced in backyard for the kids and dog to play in. Joy states “she loves the neighborhood; it is very quiet and safe.” She says this is the nicest house she has ever lived in. Prior to moving into their current house, they rented a trailer “in the middle of FAMILY ASSESSMENT 9 nowhere” and living conditions were poor. Overall the living conditions and their environment are nice, but again Thomas does struggle to meet the monthly rental payment of $1,000. Developmental Assessment Families are complex systems that deal with many different levels of progression at once; there are biological, psychological, sociological, and cultural progressions (Wright & Leahey, 2000, p. 100). The CFAM developmental category discusses family life cycle stages, the emotional process of transition and second – order changes (Wright & Leahey, 2000, p. 102).The CFAM uses Carter and McGoldricks model of the six stages of the family life cycle, these stages are: 1. Leaving home: single young adult 2. The joining of families through marriage: The young couple 3. Families with young children 4. Families with adolescents 5. Launching children and moving on Stage of Development Joy and Thomas entered stages 1, 2, and 3 of the life cycles when they were very young. Joy was 15 and Thomas was 18 when they entered stage one, Leaving Home. Thomas graduated high school, however Joy dropped out when she was 15 to move to North Carolina with Thomas. During this stage Thomas had to learn to take financial responsibility for not only himself, but for Joy too. Joy has never been successful at keeping a job. She has held two jobs, once at a fast food restaurant and the other cleaning houses, both only lasted a few weeks. Throughout the stage of Leaving Home Thomas was able to establish self-independence; however Joy heavily relied on Thomas for everything. FAMILY ASSESSMENT 10 Stage two is the Joining of Families through Marriage, the new couple. Although Joy and Thomas are not married, they have still identified themselves as a unit. During stage two they made a commitment to each other and developed close emotional ties and intimacy. Relationships with extended family members were rearranged during this stage. The couple is currently in stage three, Families with Young Children. They entered this stage three years ago, when Joy was only 17 and Thomas was 20. They were kids, taking care of kids. Both pregnancies caught Joy and Thomas by surprise. Joy has now assumed the caretaker role and Thomas juggles the financial cost of raising a child. During this life cycle stage, Joy and Thomas have accomplished the task of adjusting their relationship and accepting the responsibilities that come with childrearing. Joy and Thomas have been able to maintain an intimate bond with each other, but it appears that Joy may be over bonded with the boys and Thomas may be under bonded. Thomas does not participate in meeting the emotional and physical needs of the children, yes he supports them financially but according to Joy “he has never even changed a diaper.” Joy states that she can’t even leave the kids home alone with Thomas for her to go on a walk or run an errand to the grocery store. Throughout the Families with Young Children stage, an emotional process that Joy and Thomas have had to tackle is accepting new members into their system. Functional Assessment The functional assessment portion of the CFAM describes the family’s current interactions with each other and how they behave in relation to one another. There are two basic aspects of functions: instrumental and expressive (Wright & Leahey, 2000, p. 129). Instrumental Functioning FAMILY ASSESSMENT 11 Crucial interactions among the family make up the instrumental aspect of family functioning, which refers to the routine activities of daily living, such as eating, sleeping, preparing meals, house work, caring for children and so fourth (Wright & Leahey, 2000, p. 129). The family tends to be on a pretty routine schedule, except for Thomas whose work hours are always changing. Since he does manual labor, he never knows when he will be home. He leaves work when the job is done. For Joy and the boys, it’s a little different. The entire family wakes up on an average day between 7 and 8. Tyler is usually the first to rise and wakes the rest of the family. Thomas goes to work, while Joy is left to tend to the kids all day. Tyler goes to preschool on Monday, Wednesday and Friday and this is when Joy finds time to do chores around the house such as laundry and cleaning. On days when Tyler is home from school, he and Carter play together. Joy likes to let the boys play outdoors and they frequent the park down the street. They do not have organized family dinners. Thomas usually eats fast food on the way home from work. Joy admits to not really knowing how to cook, so the boys eat “whatever she can find” including hotdogs, pizza and frozen dinners. Joy often skips meals as she is trying to lose weight. Joy gives the boys a bath together typically between 6 and 7pm. After the bath, around 7 she reads a book to Carter and hums to him while he falls asleep. Then she goes to Tyler’s room (who watches TV as Joy puts Carter to bed), and reads a goodnight story to him. Joy is usually exhausted and in bed by 10 or 11. Thomas goes to bed at the same time; often they will lie in bed watching TV together until they fall asleep. Expressive Functioning CFAM assesses expressive functioning with nine categories of communication: emotional, verbal, nonverbal, circular, problem solving, roles, influence and power, beliefs, and FAMILY ASSESSMENT 12 alliances and collations (Wright & Leahey, 2000, p. 129). Patterns of interaction are the main focus of the functional assessment category. Emotional communication. Thomas and Joy admit to being very open with their feelings. If one is sad or mad about something, most likely the other can tell it. The children let their feelings flow by screaming, crying, pouting and rejoicing. Verbal communication. Direct verbal communication is usually understood between Joy and Thomas. However, they said that they do have a hard time communicating with the children. Carter, being only 10 months old obviously doesn’t understand much verbal communication. However, Joy says that he says “mama” and “dada”, and she thinks he understands the word “no”, although he doesn’t always listen when she says it. Tyler’s verbal communication skills are developing very quickly for a three year old; however he still does sometimes have a hard time expressing himself and understanding what others are saying. Nonverbal communication. A lot of nonverbal communication goes on throughout this family, especially with the children. Joy can tell when the children are getting tired by their use of non-verbal communication, Carter rubs his eyes and Tyler yawns. According to Thomas, Joy has a bad habit of rolling her eyes when she doesn’t get her way. Joy says that Thomas grimaces and crosses his arms when he is upset or angry about something. Throughout the interview it was noted that Thomas was fidgeting quite a bit, this could be an expression of nervousness or boredom. However, both Joy and Thomas maintained good eye contact with me throughout the process of the interview. I did notice that Joy likes to speak with her hands. When I asked Thomas a question that he was unsure of he would look at Joy, and this was her signal to go ahead and answer the question. FAMILY ASSESSMENT 13 Circular communication. A reciprocal communication that can be identified in this family is between Joy and Thomas. Joy states she has continuously asked Thomas to help her more around the house and with the kids. This angers Thomas because he works too much so he ultimately avoids the issue. This form of circular communication often leaves Joy frustrated. Problem solving. The family relies heavily on their extended family. Not only do they look to them for advice in regards to the children, but Thomas often turns to his cousin Jason for financial assistance. Roles. Roles throughout the family are well defined. Thomas is the sole source of income, and therefore is the primary financial decision maker. Although, the parent role is assumed by both Joy and Thomas, Joy has occupied the caretaker role. Carter and Tyler both are in the dependent child role. Carter is the “angel” and Tyler is the “class clown”. Joy is the “softie” and normally gives in to the children. Although Joy technically is not a wife, many would classify her as a house wife since her main duties are taking care of the house and children. Influence and power. Decision making for the household is shared by both Thomas and Joy; however Thomas always gets the final say. He monitors what Joy does, and only gives her a limited amount of money to spend. He says that she is irresponsible. Beliefs. Although they do not attend church regularly Joy tries to enforce Christian beliefs upon the children. She also tries to teach them good morals, such as treat others how you would like to be treated. Thomas has agnostic beliefs. Joy believes that because she is not sick, she is healthy. Joy tends to believe and be supportive of Western medicine, whereas Thomas prefers more of an integrative approach when it comes to his health care. Joy has a “this is how they have always done it approach” to raising her children. During the interview, it was noticed FAMILY ASSESSMENT 14 that Joy was feeding her 10 month old son Carter whole milk. I shared with Joy that according to research babies under the age of one should have either breast milk or formula, milk simply doesn’t have all the nutrients they need (Gavin, 2014). She replied that “Thomas’s mother gave him milk before a year, and he turned out fine…I trust his mom.” Alliances and Coalitions. While everyone gets along, it appears that the primary family is not extremely close with their extended family. In fact, Joy never speaks with her family. The siblings Tyler and Carter, although there is a three year age difference, are extremely close. Thomas has formed an alliance with both Joy and his brother Luke. Assessment Summary The family can be described as a non-traditional, multi-racial cohabiting family. The mother Joy, and the father Thomas, are not married. Joy is white and Thomas is black. They have two children together, Tyler and Carter who are 3 and 10 months. Thomas is the provider of income, and is forced to work hard and long hours to make ends meet. They still struggle to pay the bills and have to borrow money frequently from Thomas’s cousin Jason. They do live in a nice house, in a safe neighborhood but the house was bare. The furniture is rented. They do not have many valuables in the home. Joy also works hard. She takes care of their two sons, and maintains the house. Joy only has a tenth grade education, but would like to go back and get her high school diploma or GED one day. The primary family has a tight and loving relationship, but is distant with most of their extended family. Joy has not spoken with her mother in over a year, but she does have a friend and neighbor next door that represents a motherly figure. Joy admits to thoughts of depressions. She said that she hates being overweight, she use to be a size four, but she gained 60 pounds with her second pregnancy and she hasn’t been able to shed it. She is lonely. She has no social contacts except for the neighbor. She spends all day, every day caring FAMILY ASSESSMENT 15 for her children. Tyler, the three year old is happy and healthy. At least appears healthy, he hasn’t actually seen a physician in over two years due to lack of insurance. Carter also appears to be healthy, but throughout the time I spent with the family I do have my concerns. He appears to be slightly underweight, is not receiving the recommended nutrition and has not had his 9 month well child checkup and immunizations. Thomas is in good physical condition and stays fit through his laboring lob. However, he does smoke cigarettes; he even smokes in the home. Joy hates the fact that he smokes, not only for his health but for the children’s too. Joy’s grandfather died of lung cancer from smoking, so Thomas smoking is something she struggles with. Joy and Thomas have different beliefs when it comes to both religion and health. Although, the family has many identifiable issues they are still functioning fairly well, and are happy with their lives. Thomas and Joy are happy with their accomplishments and how far they have come together. Family Strengths The family has a very close and loving relationship. They communicate openly, and understand each other. The roles within the family are well established and equally important. The children get along well and are equally valued. Both Thomas and Tyler have social interactions with their peers, Thomas via work and Tyler though school. They have faced and overcome many obstacles, especially considering they have two children at such a young age. They are open to change, and willing to make lifestyle adjustments for the benefit of their family. Family Weaknesses and Diagnoses There is a lack of family bonding, not only with the extended family but also between Thomas and the children. Thomas stays so busy with work he does not have much time for family affairs. There are some health concerns including Joy’s depression and obesity, Thomas’s smoking, Carter’s nutrition and missed wellness checkup and lack of medical insurance for Joy, FAMILY ASSESSMENT 16 Thomas and Tyler. Joy lacks social contacts and friends, except for one who fills more of the motherly role. They struggle to pay the bills and barely make ends meet. Thomas and Joy had to grow up quickly and accept the parental roles at such young ages. Although, there is commitment between Joy and Thomas there is no marriage. Joy is not well educated, and has not been able to keep a job more than a few weeks at a time. Due to the issues I have identified and stated above, I was able to identify both family and individual nursing diagnoses. Altered Health Maintenance and Interrupted Family Processes are nursing diagnoses that I have identified that apply to the family in general. I chose Altered Health Maintenance because the only family member that carries insurance and has seen a physician in the last several years is Carter; and even Carter is overdue on his 9 month wellness exam. Interrupted Family Processes applies to this family for many reasons including their lack of family support and issues with Thomas’s lack of parenting. I have assigned two nursing diagnoses for Thomas. The first is Parental Role Conflict due to him not participating in his children’s lives as a fatherly figure because he works so much. The second is Knowledge Deficit related to smoking; Thomas smokes which is bad for him but he also does it around the children. I have assigned several nursing diagnoses to Joy including Disturbed Body Image, Joy has issues with being overweight, and she is disgusted by her body since giving birth to her second son. The next diagnosis for Joy is Impaired Social Interaction, she has only one social contact and spends all her time with her children, she admits to being lonely. Lastly, Joy is at risk for Care Giver Role Stain because she doesn’t get any help from Thomas in caring for the children. She is the sole caregiver 24 hours a day and 7 days a week, this is exhausting for her. Carter is at risk for Imbalanced Nutrition, Less than Body Requirements due to the fact that Joy is going against FAMILY ASSESSMENT 17 pediatrician recommendations and not feeding him formula or breast milk for the first year. She has introduced milk early, which doesn’t contain all the proper nutrients he needs to thrive. Family Issues One identifiable factor that I think may be contributing to several of the issues that this family experiences is their young age; they were not mentally, financially or emotionally mature enough to become parents at the ages of 17 and 20. According to Stanhope and Lancaster (2014), “teenagers who become pregnant often get caught in a cycle of poverty and school failure” (p. 415). Joy fell pregnant as a teenager at the young age of 16; she had already dropped out of school at that point but had hopes of one day returning. Joy dreams of getting her high school diploma or GED and then pursuing a nursing career, however she has not been able to go back to school due to her having children at such a young age. She does not have the support she needs to be able to attend school at this time. She also like Stanhope and Lancaster suggested, is very close to falling into a vicious cycle of poverty. Thomas completely supports her; due to her lack of education she has been unable to hold a job. If she did not have Thomas supporting her, there is a high suspension she could have ended up on the streets homeless. Joy has led a hard life. She lacked family support and many of her childhood experiences may actually have increased her likelihood of becoming pregnant as a teen. Young woman who have been deprived as a child and raised in single parent families are at risk for becoming pregnant early; many teens think that a baby will bring them joy and they can provide the love and attention their families have not provided (Stanhope & Lancaster, 2014, p. 417). Joy also may be at risk for depression. According to Stanhope & Lancaster, high levels of stress contribute to adult’s mental health status, “sources of stress include multiple-role responsibilities, job insecurity, lack of or diminishing resources and unstable relationships” FAMILY ASSESSMENT 18 (Stanhope & Lancaster, 2014, p. 423). Joy has all of the identified stress factors. She assumes multiple- role responsibilities of mother, girlfriend and home maker. She has been unable to hold a job, which has been stressful for her. She has a lack of resources not only financially but through the family and community as well; she has nobody except for the neighbor to turn to in a time of need. Lastly, she has unstable relationships with her extended family. She is estranged from her father and has not spoken with her mother in over a year. Being a mother of two young children is extremely stressful for Joy, and she doesn’t get much help. Taking care of children can be both emotionally and physically draining. Joy needs an escape outlet; she needs friends and peers to socialize with. She needs some help around the house….some alone time. Support from friends and family help mothers deal better with stress; “mothers who have the help of people they trust feel more self-esteem, confidence as a parent, and struggle less to access information that helps them problem-solve for their bundle of joy” (Guzman, 2013). According to Steakley (2011) children who are African American and live in a low income household are at the highest risk for exposure to second hand smoke. Although Tyler and Carter are multi-racial, there father Thomas is African American and smokes around them. The findings from one survey in California identified that the rate of exposure to second hand smoke for children who are African American is triple that of other races, and the lower a household income is the higher the chances of someone in the household smoking (Steakley, 2011). In one report Pfizer reviewed and analyzed national databases and arrived at facts about workers in the United States who smoke. The report findings suggest the prevalence of smoking is higher in men then woman; non-college educated then college graduates and blue collar workers then FAMILY ASSESSMENT 19 those who hold office jobs (Pfizer, 2007). All of these risk factors apply to Thomas; he is a noncollege educated, male who holds a blue collar job as a flooring installer. Maintaining child health relies on good nutrition and dietary habits, low income families are at increased risk for poor nutrition (Stanhope & Lancaster, 2014, p. 355). It is very important for both Tyler and Carter to eat healthy, due to their age difference their dietary needs and recommendations are different. The American Academy of Pediatrics (AAP) recommends that whole cow milk not be introduced for the first year of life; instead the child should drink breast milk or formula and may begin to introduce solid baby food at 6 months of age (American Academy of Pediatrics, 1992). I advised Joy against giving Carter Cow’s milk in the replacement of formula or breast milk. The American Academy of Pediatrics (1992) released the following statement: Infants fed cow’s milk have low intakes of iron, linoleic acid, and vitamin E, and excessive intakes of sodium, potassium, and protein, illustrating the poor nutritional compatibility of solid foods and cow’s milk. These nutrient intakes are not optimal and may result in altered nutritional status, with the most dramatic effect on iron status. Infants fed iron-fortified formula or breast milk for the first 12 months of life generally maintain normal iron status (p. 1107). Tyler also doesn’t eat a very healthy diet, he often eats junk food or frozen dinners. The AAP (2014) says to choose foods that aren’t “overly sugary, fatty, or salty”. Joy admitted to not really knowing how to cook. But meals don’t have to be elaborate; in fact some don’t even require cooking. A quick meal could be a turkey sandwich, a side of green beans or apple sauce and a glass of milk. According to the AAP (2014), obesity is a growing childhood epidemic in America, and for this reason Joy needs to be aware and monitor her children’s dietary habits. FAMILY ASSESSMENT 20 Not only are the children’s dietary habits unhealthy both Joy and Thomas’s are as well. Thomas’s diet consists of mostly fast food, whereas Joy skips a lot of meals. Neither of these options is considered healthy. Joy needs to understand there are healthy ways to lose weight and skipping meals is not one of them. In fact dietician Dawn Blatner, warns against skipping meals and instead eating vegetables, drinking water, keeping a food journal and getting tempting food out of the home (Zelman, 2014). Instead of eating fast food while working, Thomas can bring a healthy lunch alternative like a sandwich, apple and pretzels which would also be more cost effective then buying fast food routinely. One of the biggest and most surprising issues I found within this family was their lack of medical insurance. Carter is covered under Medicaid until he turns one. However the rest of the family is without health coverage. Neither Joy or Thomas have ever had insurance, however Joy was covered under Medicaid while she was pregnant. Thomas’s work doesn’t offer employee insurance, and he can’t afford private insurance. Tyler did have Medicaid, but when they tried to renew they were told Thomas made too much. This was very surprising to me. Here I am looking at a family that is struggling to pay their bills, with only one source of income for a family of four - and they don’t qualify for assistance? Apparently, this happens more then I realized. According to Stanhope and Lancaster (2014), “an increasing number of middle-income families have major wage earners…but often do not have enough income to purchase health care but earn too much money to qualify for public assistance programs” (p. 333). Under Obama’s Health Care Reform many Americans may now qualify for subsidized insurance under their states health insurance marketplace (Swartz, 2014). Joy and Thomas unfortunately do not know much about health care coverage, let alone the affordable care act, and missed the deadline to apply. Open enrollment for 2015 coverage will open in November 2014 (Swartz, 2014). While FAMILY ASSESSMENT 21 researching Medicaid requirements, I learned about the North Carolina Health Choice (NCHC). NCHC is a comprehensive healthcare plan specifically designed to cover children whose family makes too much to qualify for Medicaid, but not enough to afford private insurance (North Carolina Department of Health and Human Services, 2013). Like me, neither Joy nor Thomas was aware of NCHC, but it would be something they would like to pursue. Another issue I identified was that Carter, who is 10 ½ months old, has not had his 9 month old checkup. The wellness checkup is crucial because it not only identifies that the child is meeting developmental milestones, growing and gaining weight appropriately but the child also receives vaccines. Routine immunizations for children are important in disease prevention; a challenge can be to make sure the child gets the vaccine at the appropriate time (Stanhope & Lancaster, 2014, p. 355). The Center for Disease Control and Prevention (CDC), recommends a child be given their 3rd dose of the Hepatitis B vaccine and an inactivated poliovirus at their 9 month well child checkup (National Center for Immunization and Respiratory Diseases, 2014). While discussing the importance of the well child visits and immunizations with Joy she admits to forgetting about the appointment and then procrastinates to reschedule. I can’t help but to wonder if Joy’s young age is leading to her not taking her son’s wellness checkup seriously. Family Comparison Both Joy and Thomas came from low income homes. Ethnicity, religion, socioeconomic status, race and environment all play a role in how a family will transition in its own life cycle (Wright & Leahey, 2000, p. 125). This family so far has followed right along with Fulmer’s life cycle stage of the low-income family. As Fulmer suggest Joy did have her first pregnancy and attempt to go to high school between the ages of 12-17, then between the ages of 18-21 she had her second pregnancy and received no further education (Wright & Leahey, 2000, p. 126). If she FAMILY ASSESSMENT 22 maintains on this path according to Fulmer's family life cycle stages she will have her third child and get married between the age of 22-25, but then separate from her husband by the age of 30 (Wright & Leahey, 2000, p. 126). Statistics from the 2012 US Census were reviewed for comparisons of this family and their characteristics, amongst other families. The census identified that partners of different races were less likely to be married then those of the same race (Vespa, Lewis, & and Krieder, 2013, p. 17). This statistic does apply to Joy and Thomas, because Joy is Caucasian and Thomas is African American and they are unwed. The report found that children whose parents are married typically have a higher socioeconomic status, but 1 in 2 children who either live with their mother only, two unmarried parents or no parents at all live below the poverty level (Vespa, Lewis, & and Krieder, 2013, p. 23). Carter and Thomas do have two unmarried parents, but fortunately they do not fall below the poverty level. Almost 90% of children live with either married parents or their mother (Vespa, Lewis, & and Krieder, 2013, p. 23). Thomas and Carter fall into the category of living with either unmarried parents, father only or no parents which make up 12% of America’s children. Cohabiting parents like Joy and Thomas were found to be young; “about 23 percent of cohabiting women and 13 percent of cohabiting men who had children under the age of 18 were between 15 and 24 years old; the corresponding figures for male and female spouses were 2 percent and 4 percent, respectively” (Vespa, Lewis, & and Krieder, 2013, p. 19). This statistics applies to Thomas and Joy because they are cohabiting and are 24 and 21 years old. And lastly married parents were found to be better educated. 40% of married woman with children under 18 have a bachelor’s degree, compared to only 12% of cohabiting woman with FAMILY ASSESSMENT 23 children (Vespa, Lewis, & and Krieder, 2013, p. 19). Joy is cohabiting mother of children under the age of 18 and she does not have a high school diploma, let alone a bachelor’s degree. To sum it up although this family does relate to many of the census statistics for unmarried parents, they have overcome some of the obstacles other unmarried families living in America have such as living in poverty. Family Care Plan 1. Altered Health Maintenance as evidenced by not maintaining health insurance, not seeing a physician in years, missing Carter’s 9 month wellness checkup and immunizations, poor dietary habits and smoking. Goals: Family describes positive health maintenance behaviors such as keeping scheduled appointments, participating in smoking cessation programs, and making diet and exercise changes Family identifies available resources. Family uses available resources. Interventions: Assess family’s knowledge of health maintenance behaviors. Joy and Thomas may know that certain unhealthy behaviors can result in poor health outcomes but continue the behavior despite this knowledge. I need to ensure that the family has all of the information needed to make good lifestyle choices. Assess health history over past 5 years. This may give some perspective on whether poor health habits are recent or chronic in nature. FAMILY ASSESSMENT 24 Assess to what degree environmental, social, interfamilial disruptions or changes have correlated with poor health behaviors. These changes may be precipitating factors Determine to what degree their cultural beliefs and personality contribute to altered health habits. Health teaching may need to be modified to be consistent with cultural or religious beliefs. Assess whether economic problems present a barrier to maintaining health behaviors. They may be too proud to ask for assistance or be unaware that Obama care and Child Health Insurance could be helpful to them. Follow-up on clinic visits with telephone or home visits. To develop an ongoing relationship with patient and to provide ongoing support. Compliment family on positive accomplishments. To reinforce behaviors. Provide Smoking Education and Cessation Information and support. Smoking has been linked to cancers and many other medical conditions Educate the family on the importance of a balanced diet. Bad dietary habits can lead to bad health Educate on the importance of immunizations. Immunizations have been proven successful against many diseases. Provide the family with the proper recourses on how to get Marketplace Insurance. This may be a more affordable insurance program for the family. 2. Caregiver Role Stain as evidence by multiple competing roles, social isolation of Joy, unavailability of community resources, time and freedom restricted due to caregiving. Goals: FAMILY ASSESSMENT 25 Joy reports that formal and informal support systems are adequate and helpful Joy uses strengths and resources to withstand stress of caregiving. Joy demonstrates competence and confidence in performing the caregiver role by meeting care recipient's physical and psychosocial needs. Joy expresses satisfaction with caregiver role. Interventions: Establish relationship with Joy and children. To facilitate assessment and intervention. Assess caregiver-care recipient relationship. Dysfunctional relationships can result in ineffective, fragmented care or even lead to neglect or abuse. Assess family communication pattern. Open communication in the family creates a positive environment whereas concealing feelings creates problems for caregiver and care recipient. Assess family resources and support systems. Family and social support is related positively to coping effectiveness. Assess Joy’s appraisal of caregiving situation, level of understanding, and willingness to assume caregiver role. Individual responses to potentially stressful situations are mediated by an appraisal of the personal meaning of the situation. Encourage Joy to identify available family and friends who can assist with caregiving. Successful caregiving should not be the sole responsibility of one person. Encourage involvement of Thomas to relieve pressure on primary caregiver. Caring for a child can be a mutually rewarding and satisfying family experience. FAMILY ASSESSMENT 26 Encourage Joy to set aside time for her. This could be as simple as a relaxing bath, a time to read a book, or going out with friends. Teach caregiver stress-reducing techniques. Encourage Joy to join and participate in a Mommy group. Groups that come together for mutual support can be quite beneficial in providing education and anticipatory guidance. Acknowledge to Joy the role she is carrying out and its value. Caregivers have identified how important it is to feel appreciated for their efforts 3. Risk for Altered Nutrition, less then body requirements as evidence of Carter assuming whole cow milk as more source of nutrients Goals: Joy will verbalize and demonstrate selection of foods or formula that will achieve proper nutrition for Carter. Carter will weigh within 10% of his ideal body weight at his next appointment Interventions: Determine etiologic factors for reduced nutritional intake. Proper assessment guides intervention. For example, maybe the family cannot afford formula. Monitor or explore attitudes toward eating and food. Many psychological, psychosocial, and cultural factors determine the type, amount, and appropriateness of food consumed. Consult dietitian for further assessment and recommendations regarding food preferences and nutritional support. Dietitians have a greater understanding of the nutritional value of foods and may be helpful. FAMILY ASSESSMENT 27 Educate Joy about the lack of nutritional components that Carter needs that are not in Cow’s milk. Babies should not have cow’s milk till 1 year of age Provide referral to community nutritional resources such as WIC. WIC can assist with formula and baby food, Carter automatically qualifies since he receives Medicaid. 4. Disturbed Body Image related to the situational change of during/post pregnancy as evidence by verbalization of obesity Goals: Joy will demonstrate enhanced body image and self-esteem as evidenced by ability to look at, talk about, and care for actual or perceived altered body part image. Interventions: Assess perception of change in structure of body (also proposed change). The extent of the response is more related to the value or importance Joy places on her body than the actual value or importance. Assess impact of body image disturbance in relation to patient's developmental stage. Young adults may be particularly affected by changes in the structure or function of their bodies at a time when developmental changes are normally rapid, and at a time when developing social and intimate relationships are particularly important. Assess perceived impact of change on activities of daily living (ADLs), social behavior, personal relationships, and occupational activities. How does this affect Joy? FAMILY ASSESSMENT 28 Refer Joy to support groups comprised of individuals who are also overweight. Lay persons in similar situations offer a different type of support, which is perceived as helpful. Help Joy identify healthy ways she can lose weight. Identifying healthy weight loss options, help to discourage bad habits such as crash dieting Reassure Joy that she is beautiful. Words of encouragement are always good to hear 5. Social Isolation as evidence by lack of friendships and resources Goals: Identify stable support system and supportive individual Utilize community resources Interventions: Determine Joy’s response to condition, feelings about self, concerns or fears about response of others, sense of ability to control situation, and sense of hope. How Joy accepts and deals with the situation will help decide the plan of care and interventions. Assess coping mechanisms and previous methods of dealing with life problems. This may reveal successful techniques that can be used in current situation. Identify availability and stability of support systems including Thomas, immediate and extended family, and community. This information is crucial to help client plan future care. Encourage contact with significant other, family, and friends. Many people fear telling their significant other, family, and friends for fear of rejection, and some FAMILY ASSESSMENT 29 people withdraw because of tumultuous feelings. Contact promotes sense of support, concern, involvement, and understanding. Help Joy differentiate between isolation and loneliness or aloneness, which may be by choice. Provides an opportunity for Joy to realize the control she has to make decisions about the choice to take care of self about these issues. Identify community resources, such as mother groups. Provides opportunities for resolving problems that may contribute to sense of loneliness and isolation. 6. Knowledge deficit related to health risk of smoking as evidence by Thomas currently smoking ½-1 pack a day. Goals: Thomas demonstrates motivation to learn. Thomas identifies perceived learning needs. Thomas verbalizes understanding of desired content, and/or performs smoking cessation. Interventions: Assess Thomas’s motivation and willingness to learn. Adults must see a need or purpose for learning. Some patients are ready to learn; others cope better by denying or delaying the need for instruction. Learning also requires energy, which Thomas may not be ready to use. Question Thomas regarding previous experience and health teaching. Adults bring many life experiences to each learning session. Adults learn best when teaching builds on previous knowledge or experience. FAMILY ASSESSMENT 30 Identify any existing misconceptions regarding material to be taught. This provides an important starting point in education. Determine cultural influences on health teaching. Providing a climate of acceptance allows patients to be themselves and to hold their own beliefs as appropriate. Determine Thomas’s learning style, especially if he has learned and retained new information in the past. Some persons may prefer written over visual materials, or they may prefer group versus individual instruction. Matching the learner's preferred style with the educational method will facilitate success in mastery of knowledge. When presenting material, move from familiar, simple, and concrete information to less familiar, complex, or more abstract concepts. This provides Thomas with the opportunity to understand new material in relation to familiar material. Review the associated health risk of smoking. Thomas may not be aware of the health risk associated with smoking, and exposing children to second hand smoke. Discuss ways to help quit smoking (patch, gum, e-cig, cold turkey). This helps to identify alternatives to smoking. Refer Thomas to support groups as needed. He may benefit from talking with others who are also trying to quit smoking. Principals of Intervention The Calgary Family Intervention Model (CFIM) is complementary to the Calgary Family Assessment Model. The CFIM examines interventions for family function across three domains: cognitive, affective, and behavioral. Interventions should be designed to promote, improve or FAMILY ASSESSMENT 31 sustain family functioning. Interventions implemented should match the problem, flow with the nurse’s hypotheses and match the family’s strengths (Wright & Leahey, 2000, p. 311). One of the family’s strengths that I identified was their openness mindedness, and their willingness to make lifestyle changes for the better good of their family. The willingness to accept change was crucial during the implementation of the interventions. Not only did I want the interventions I implemented to help the family, but I also wanted to focus on empowerment which allowed the family to assume an active role in their health care. Principals of empowerment include the ability to identify and obtain needed resources and the development of decision-making and problem solving skills (Wright & Leahey, 2000, p. 342). The goal of the empowering approach is to create a partnership and shared responsibility; “interventions that promote desired family behaviors increase family competency, decrease the need for outside help, and result in families seeing themselves as being actively responsible for bringing about desired changes” (Wright & Leahey, 2000, p. 342). To promote empowerment I helped the family to identify several resources including online websites that foster smoking cessation, child nutrition, healthcare access and community support for mothers. Evaluation and Conclusion The nursing interventions I implemented were focused on health promotion and maintenance. The family has demonstrated the desire to learn and make life style changes that will benefit their family. One of my goals throughout this process was to help Thomas identify the reasons smoking was harmful and to identify ways to help him quit once he has made the commitment to change. According to Stanhope and Lancaster (2014), Americans who use interventions to quit smoking such as nicotine replacement, behavioral modifications or medication are most likely to FAMILY ASSESSMENT 32 be successful (p. 448). I referred Thomas to the Center of Disease Control and Prevention’s website, where we reviewed the associated health risk of smoking, the benefits of quitting and several methods to help him quit. Thomas has stated that he would like to try and quit smoking again; he decided he was going to purchase an electronic cigarette with the intentions to be completely nicotine free within the year. I also wanted to promote optimal nutrition; no member of the family had good eating habits. Stanhope and Lancaster (2014), recognize that “low income families are at an increased risk for poor nutrition” and nurses can guide families to improve their nutrition by providing information on good nutrition (p.355). They also recommend the American Academy of Pediatrics website as a useful source of information which offers information about childhood nutrition (Wright & Leahey, 2000, p. 355). After reviewing this website with Joy, she shared my concern about Carter not getting the proper nutrition from milk. I informed her that since he receives Medicaid he automatically will qualify for Woman, Infant and Children (WIC) assistance where he can get vouchers for formula. Joy committed to calling the WIC office and setting up an initial appointment so she can apply. To encourage healthy nutrition and obesity prevention I suggested they modify their family eating habits to include low-fat food choices, whole grains, fruits and vegetables as Stanhope and Lancaster have recommended (2014, p. 349). Joy appreciated me reviewing the food pyramid with her, and states that she is going to not only try and eat better but she is going to try and establish family dining to include healthy alternatives. Health promotion was addressed by encouraging Joy to schedule and keep Carters wellness appointments, promoting child immunizations and exploring healthcare insurance resources. Stanhope and Lancaster (2014) state “it is important to repeatedly urge parents to FAMILY ASSESSMENT 33 obtain immunizations for their children”. Together Thomas, Joy and I reviewed the CDC’s website and learned why and what immunizations Carter should have at his 9 month checkup. Joy plans on calling and rescheduling Carters appointment as soon as possible, she assured me she will not let him lapse on his wellness checkup/immunizations again. Because Stanhope and Lancaster (2014) suggest “nurses play an important role in teaching families about the resources available to them and giving them clear instructions about how and where to apply for needed services” (p. 334), I wanted to review health care insurance options with the family. Together we reviewed Healthcare.gov which contains a wealth of information on the Affordable Care Act, Medicaid, marketplace insurance, and Children’s Health Insurance Programs (CHIP); there we were able to identify the types of healthcare coverage programs the family could qualify for and how to apply. After reviewing the information and the different options with the family, they decided they are going to try and get Tyler enrolled in the North Carolina Health Choice for Children plan which offers comprehensive health coverage to children who don’t qualify for Medicaid, but whose parents can’t afford private insurance (North Carolina Department of Health and Human Services, 2013). Joy acknowledges that she must go to the Department of Social Services to apply and she plans on doing this, she is very enthusiastic at the possibility that Tyler can again have healthcare coverage. Joy and Thomas think marketplace insurance may be best for them but realize they missed the deadline to apply this year. They have been set up with the resources and intend to apply in November for 2015 coverage. Lastly, I wanted to help Joy find ways to be able to make time and enjoy herself. Lacking the support system she needs, she is the sole caregiver for Tyler and Carter. Furthermore she has no real social outlets except for her neighbor whom is a motherly figure. According to Holley FAMILY ASSESSMENT 34 (2007), “social isolation is a serious problem in our society…the lack of needed and wanted social contacts is a serious source of discomfort that can lead to further health problems”. Nurses are in a unique position to intervene, practical interventions include referring the patient to a support group, helping to rebuild the family network, enhancing the patients spirituality, and helping the patient use internet based supports (Holley, 2007). To help assist Joy, I spoke with Thomas to see if he would be receptive to helping her more with the children. He said he would, but because he works so much the time would be limited. Next, I explored with Joy ways that she can gain social contacts. Wilmington has several mommy and me groups, where mothers (and their kids) get together for play dates. Together we identified several of these groups online including Mom’s Club of Wilmington and Circle of Mom’s. We also identified an online mommy support forum, Wilmingtonmommies.com which offers friendships, support and fun for moms. Joy is very excited about the opportunity to meet other moms in the area while also letting her children play. Overall, I think that this family is functioning fairly well considering all the obstacles they have had to face in life. Like all families, they have their issues but they also have great strengths. The weaknesses that I was able to identify during the completion of this interview and assessment were for the most part addressed. I feel that the family was very open and receptive to the idea of change. The interventions that I implemented were well received, and I feel I have been a great benefit to this family. Hopefully if they follow through with their plans, and utilize the tools and resources I have left them with, they will continue to focus on health promotion and prevention in their lives. They have the passion and the vision, now it’s up to them to take charge of their lives. FAMILY ASSESSMENT 35 References American Academy of Pediatrics. (1992, June). The Use of Whole Cow's Milk in Infancy. Pediatrics, 89(6), 1105-1109. Retrieved from http://pediatrics.aappublications.org/content/89/6/1105.short American Academy of Pediatrics. (2014). Healthy Children. Retrieved from American Academy of Pediatrics: http://www.healthychildren.org/english/agesstages/toddler/nutrition/Pages/default.aspx Gavin, M. (2014, February). When Can Babies Begin Drinking Cow's Milk. Retrieved from Kids Health: http://kidshealth.org/parent/pregnancy_newborn/feeding/cow_milk.html Guzman, M. (2013). New Moms Need Social Support. Moral Landscapes. Retrieved from http://www.psychologytoday.com/blog/moral-landscapes/201301/new-moms-needsocial-support Holley, U. (2007). Social isolation: a practical guide for nurses assisting clients with chronic illness. Rehabilitation Nursing, 32(2), 51-56. doi:http://www.ncbi.nlm.nih.gov/pubmed/17432633 National Center for Immunization and Respiratory Diseases. (2014, January 31). Recommended Immunization Schedule. Retrieved from Center for Disease Control and Prevention: http://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent-shell.html North Carolina Department of Health and Human Services. (2013, May 16). What is Health Choice for Children. Retrieved from NC Division of Medical Assistance: http://www.ncdhhs.gov/dma/healthchoice/index.htm Pfizer. (2007). Smoking in the United States Workforce. Retrieved from Pfizer Facts: http://www.pfizer.com/files/products/Smoking_in_the_US_Workforce.pdf FAMILY ASSESSMENT Stanhope, M., & Lancaster, J. (2014). Foundations of Nursing in the Community (4th ed.). St. Louis: Elsevier. Steakley, L. (2011, October 28). Report shows African-American, low income children in California at highest risk for secondhand smoke. Retrieved from Stanford Medicine: https://scopeblog.stanford.edu/2011/10/28/report-shows-african-american-low-incomechildren-at-highest-risk-of-secondhand-smoke/ Swartz, K. (2014, April 1). Health Care Reform: Health insurance & the affordable care act. Retrieved from WebMD: http://www.webmd.com/health-insurance/nc/north-carolinahealth-insurance-marketplace?page=2&state=NC Vespa, J., Lewis, J., & and Krieder, R. (2013). America's Families and Living Arrangements:2012. US Departmen of Commerce. Retrieved from http://www.census.gov/prod/2013pubs/p20-570.pdf Wright, L. M., & Leahey, M. (2000). Nurses and Families: A guide to family assessment and interventions. Philadelphia: F.A Davis Company. Zelman, K. (2014). Lose Weight Fast: How to do it safely. Retrieved from WebMD: http://www.webmd.com/diet/features/lose-weight-fast-how-to-do-it-safely 36 FAMILY ASSESSMENT 37 Family Journal Sunday April 6, 2014 I met with the family on a Sunday afternoon, in their home. I wanted to meet them in their home to observe their environment and living conditions first hand. This was the first time meeting with the family, so I began the interview by introducing myself and my role as a Registered Nurse pursuing my BSN. I explained the purpose of my interview was to gather information and perform a family focused assessment. I informed them I was going to try and identify strengths and weaknesses they may have and help them work through them. I then proceeded to talk to Joy and Thomas about how and when they met. I spoke with them a little bit about their childhood and how they were raised. We discussed there ethnicity, and any cultural issue they may want addressed. I also spoke with them about their religious beliefs. I asked Thomas and Joy to tell me about their family, including their ages and any medical or psychologically history they may have. I drew a genomap from the information they provided. I spoke with them about their education and employment status. We then began a discussion about their children Carter and Tyler, who were present for the interview. However, Tyler was running in and out of the room to watch TV in the next room. I identified their ages, and how having children at such a young age has affected them. I was able to quickly identify some issues simply by observing the family. For instance, Thomas smoked a cigarette during the interview (in his home, with his children in the room) and Joy gave Carter a bottle of cow’s milk. Joy expressed frustration with Thomas for smoking in the home and around the children. I questioned Joy as to why she was giving Carter cow’s milk at 10 months of age, she stated she had just stopped nursing and that’s what Thomas’s mom told her to give Carter. With this FAMILY ASSESSMENT 38 interview I mainly just wanted to gather general information and characteristics about the family. I plan to dig deeper into some of the issues next time we meet. I wanted to go ahead and address the two main issues I recognized this meeting with the family and they were Thomas’s smoking and Carter drinking cow’s milk. I asked Thomas if he would be interested in quitting smoking; he stated he has tried in the past and never could. I asked him if he would be willing to try again and if he knew the health risk of smoking. He said “lung cancer”. I taught Thomas that there are many other risk factors that come along with smoking besides lung cancer; including multiple types of cancer, heart attacks, strokes, and respiratory diseases. I then reviewed smoking cessation methods with Thomas. I discussed many options for quitting including nicotine patch/gum, Chantix, electronic cigarettes, hypnosis and acupuncture. I did not have any patient handouts readily available but together we reviewed the website for the Center for Disease Control and Prevention. We were able to identify associated risk of smoking and helpful ways to quit. I also told him about the support phone line 1-800Quit-Now. I wanted to educate Joy about the importance of Carter getting the proper nutrition. Myself recently having a baby I have done a lot of research on the recommend nutrition and have spoken with the pediatrician. I knew that the American Academy of Pediatrics recommends that children not consume cow’s milk until after the age of 1, until then they should be getting most of the nutrition from either breast milk or formula. I told Joy that cow’s milk simply doesn’t have all the nutrients that Carter needs. Together we reviewed the American Academy of Pediatrics parent resource website. Joy was surprised but was receptive. The family expressed initial concerns with their privacy. They knew I would be using the information I gathered to help me with a project at school and wanted to make sure that their FAMILY ASSESSMENT 39 personal information would not be shared. I informed the family that to protect their privacy, I would be changing all names that were included in my reports. This reassured the family and allowed them to feel more comfortable in sharing this private information with me. I learned a lot in general about the family during the interview. I also learned that not everybody is aware of the health risk associated with smoking. I thought this was common sense, but now that I think more about it….all the anti-smoking campaigns usually concentrate on lung cancer; many people probably are not aware of the other dozens of associated risk factors such as heart attack and strokes. I also learned that mothers don’t always get the proper information. Joy was never informed that her infant should not have cow’s milk at such a young age. I had only learned by being proactive and researching what I should be feeding my baby, and then asking the pediatrician for clarification. Most importantly, I learned that I should never assume anything. This was the first family interview I have ever done in my nursing career and I can use what I have learned from this experience towards my nursing career. Now that I have my first real interview under my belt, I feel I will be more confident with my interview questions and approach in the future. This process has helped me to feel more comfortable speaking with a family about delicate situations and intervening. Saturday April 10th, 2014 This visit I again met with the family in their home. Now that the family was feeling more comfortable with me, I wanted to utilize this visit to talk more about personal issues such as their health and any issues they might be experiencing. While exploring how the family perceived their own health, I discovered that the family (except Carter) is without insurance. FAMILY ASSESSMENT 40 While addressing health issues, Joy expressed concern about being overweight, and not losing the “baby weight”. During this visit I also spoke with the family about what they like to do for leisure, this is when I discovered that Joy really didn’t have any social contacts besides one neighbor. She stated she was always caring for the children; this led into a conversation about the extended family and their involvement. I learned that Joy was not close with her family at all, and most of Thomas’s family was also considered distant. The most important topic for me to addresses with the family was there lack of insurance. They said that they tried to get Medicaid a couple of years ago, but were declined because “Thomas made too much”. I informed them of Obama’s new health care reform. They said they had heard a little but really didn’t understand or know much about it. I informed them that under the new laws, they must carry health insurance or they will have to pay a penalty. I educated them about the North Carolina Marketplace, and how it offers lower cost healthcare plans to people without insurance based on household size and income. I also spoke with them about North Carolina’s Health Choice for Children program (HCCP), which enables children whose family do not qualify for Medicare but can’t afford private insurance to obtain health coverage. Together we reviewed two websites which I feel will be huge resources to this family in obtaining medical coverage. The first website was The North Carolina Department of Health and Human Services – here we looked at the HCCP and more about who is eligible and how to apply. We discovered they can apply in person at the County Department of Social Services. Next, we looked at Healthcare.gov which is a wealth of information on the affordable care act and the different options to obtain insurance. It reviews the marketplace plan and how to apply. We unfortunately discovered they missed this year’s deadline to apply, but they can apply for the year 2015 beginning in November. FAMILY ASSESSMENT 41 I also felt it was important for me to address some issues I had noticed about Joy, her lack of friendships/social interaction and issues with her weight were a concern for me. I talked to Joy about great mother groups Wilmington has. There are several such as Circle of Mom’s, Moms of Preschoolers and Mommy and Me. These types of group normally meet once or twice a month and it allows the mother some time to socialize with other mothers, the children normally play. I also turned Joy on to the website Wilmingtonmommies.com; this is a great online community for moms. She had also expressed concern about being overweight and mentioned she often “skips meals”. I educated Joy that skipping meals is very unhealthy and there are actually dieticians who recommend against it when trying to lose weight; I instructed her instead to try a healthy alternative such as fruits, vegetables and foods low in fat. Together we reviewed the food pyramid and came up with a sample healthy meal the whole family could enjoy. The interview was effective and I was able to gain a lot of information about the family, and help them with some issues. However, they did express a concern over the healthcare penalty I mentioned to them. They said that this was the first they had heard of it, and they didn’t want to have to pay a fine. I informed them they may not have to pay a penalty, that there are certain exemptions they can file for. We then reviewed these exemptions on the internet and determined they may be exempt because Thomas was denied Medicaid and NC didn’t expand coverage, and Joy does not have an income. Finding out this information helped them to feel reassured. They were excited about the possibility of them gaining insurance through the marketplace. Throughout this interview experience I was able to learn a lot myself about the Affordable Health Care act, and how many American’s who cannot afford insurance can gain access to coverage. I had heard about the penalties for those who did not have insurance, but I FAMILY ASSESSMENT 42 didn’t know there were exemptions. While reviewing the websites with Thomas and Joy, I discovered there are actually a lot of exemptions and many Americans probably do not have to pay the penalty. I can use this information in my career and in the future. I come in contact on a daily basis with patients who do not have insurance. Now that I know more about the Affordable Care Act and all it has to offer, I will feel more confident and comfortable in discussing this with my patients. I hope to help more people gain access to health coverage.