over the counter drugs
advertisement

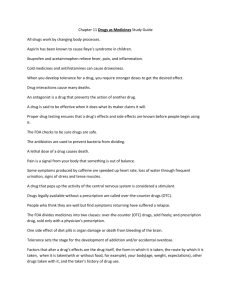
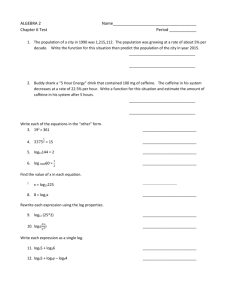
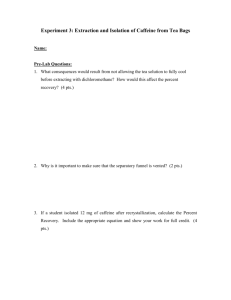
OTC DRUGS • ANALGESICS • ANTI-HISTAMINES • HERBALS OVER THE COUNTER DRUGS SELF MEDICATION IS AN INTEGRAL PART OF HEALTH CARE TODAY. PEOPLE LIKE TO MEDICATE THEMSELVES. HOWEVER, SELF MEDICATION IS BEING PRACTICED TODAY WITH THE DEGREE OF SOPHISTICATION THAT BELONGS TO THE DARK AGES. BY DEFINITION, OVER THE COUNTER DRUGS (OTC DRUGS), ARE THOSE THAT ANYONE CAN BUY WITHOUT A PRESCRIPTION. THEY ARE SELF PRESCRIBED, AND SELF ADMINISTERED FOR THE RELIEF OF SYMPTOMS OF A SELF DIAGNOSED ILLNESS. ONE ESTIMATE IS THAT EVERY 3 OUT OF 4 INDIVIDUALS HAVE THE SYMPTOMS OF AN ILLNESS EACH MONTH, BUT ONLY 1 OF THESE 3 SEEK PROFESSIONAL HELP. THAT MEANS THAT OTC COMPOUNDS ARE FREQUENTLY BEING TURNED TO FOR RELIEF. • OTC PACKAGES MUST CARRY AT LEAST THE COMMON OR GENERIC NAMES AND QUANTITIES OF THEIR ACTIVE INGREDIENTS, AS WELL AS THE AMOUNT OF ALCOHOL, IF ANY, THEY CONTAIN. • THE LABELS MUST ALSO INCLUDE INSTRUCTIONS FOR USING THE DRUG, INCLUDING SIMPLE DIRECT WARNINGS AND LIMITATIONS ON THEIR USE, SUCH AS "DISCONTINUE USE IF PAIN PERSISTS AND CONSULT A PHYSICIAN." • THE DIFFERENCE BETWEEN AN OTC DRUG AND PRESCRIPTION DRUG: • (FROM FDA) "A DRUG SHALL BE PERMITTED FOR OTC SALE AND USE BY THE LAITY UNLESS, BECAUSE OF ITS TOXICITY OR OTHER POTENTIAL FOR HARMFUL EFFECT OR BECAUSE OF THE METHOD NECESSARY TO ITS USE, IT MAY BE SAFELY SOLD AND USED ONLY UNDER A PRACTITIONERS PRESCRIPTION." • USUALLY THIS TRANSLATES TO MEAN THAT THE ONLY DIFFERENCE BETWEEN AN OTC AND A PRESCRIPTION PRODUCT IS THE GREATER AMOUNT OF AN ACTIVE INGREDIENT IN THE PRESCRIPTION DOSE. • IN 1962, FOOD, DRUG, AND COSMETIC ACT STATED THAT ALL DRUGS MUST BE EVALUATED FOR EFFECTIVENESS AS WELL AS BEING SAFE. • THE PROBLEM WITH ENFORCING THIS ACT IS THAT NO ONE KNOWS HOW MANY OTC PRODUCTS ARE ON THE MARKET. • THE FDA ALSO DOES NOT REQUIRE THE MANUFACTURER TELL ANYONE, INCLUDING THE CUSTOMER OR THE FDA, WHEN THERE IS A CHANGE IN THE INGREDIENTS OR IN THE AMOUNT OF AN INGREDIENT IN A PRODUCT. THE FDA ALSO DECIDED ON ANOTHER REGISTRATION CALLED: GENERALLY RECOGNIZED AS HONESTLY LABELLED: WHICH STATED THAT LABELLING SHALL BE CLEAR AND TRUTHFUL IN ALL RESPECTS, AND MAY NOT BE FALSE OR MISLEADING IN ANY PARTICULAR. • THE LABEL MUST STATE THE INTENDED USES AND RESULTS OF THE PRODUCT, AND ADEQUATE DIRECTIONS FOR PROPER USE AND WARNINGS AGAINST UNSAFE USE, SIDE EFFECTS, AND ADVERSE REACTIONS. How are we protected? The FDA and its history In 1929 the US. Post office forced pharmacist Harold Watkins to stop promoting his lucrative weight loss formula. Harold was jobless after the stock market crash and throughout the depression. He was eventually hired by the S.E.. Massengill company Bristol, Tennessee. In July 1937 Harold was asked to find a solvent for the new anti-biotic sulfanilamide. The drug was very effective against gonorrhea, meningitis and strep throat. However the tablets were too big and difficult to swallow, especially for children. Harold was instructed, as the company's chief chemist, to make it into a liquid. Harold chose the solvent diethylene glycol, a sweet syrupy liquid. Sometimes used as anti-freeze Harold held a degree in pharmaceutical chemistry but was not aware that this solvent could be a deadly poison at certain doses. Harold added to the solution saccharin, caramel, amaranth, raspberry extract. Harold tasted the concoction himself and with no further tests sent it to the manufacturing laboratories. By September 1937 the lab had shipped 240 gallons of "elixir sulfanilamide." By October of the same year almost 12 gallons had been prescribed. In that year, 107 children died after taking the elixir. Samuel E. Massengill insisted his company was blameless, but fired Watkins anyway. The government could only charge Massengill and his company with improper labeling since the nation's food and drug law was so feeble at that time. Within months the food drug and cosmetic act had cleared both houses and in June 1938 president Franklin D. Roosevelt signed it into law. This act is still enforced today and requires drug makers to prove all new products safe and effective. On January 10, 1939 Samuel E. Massengill was elected president of the Bristol chamber of commerce. Watkins, morose at this time, retreated to his home and read of the election of Massengill. A brief notice appeared in the Bristol Herald Courier a week later. "Harold Cole Watkins, 58, retired chemist, was found dead Tuesday morning in the kitchen of his home, a discharged 38 caliber automatic pistol lying near his body. He had been shot once through the heart." DRUG ADVERTISING TENDS TO PRESENT A PAIN, PILL, PLEASURE MODEL WHICH FUNCTIONS TO VALIDATE AND ENFORCE VALUES, ATTITUDES, AND BEHAVIOR THAT ENCOURAGE THE MISUSE AND ABUSE OF SUCH DRUGS. WHERE IS PAIN? Kong, J. et al. J. Neurosci. 2006;26:381-388 Copyright ©2006 Society for Neuroscience • CLASSIFICATION OF PAIN GOES INTO TWO TYPES DEPENDING ON PLACE OF ORIGIN. • VISCERAL PAIN, SUCH AS INTESTINAL CRAMPS, ARISES FROM NONSKELETAL PORTIONS OF THE BODY. • NARCOTICS ARE EFFECTIVE IN REDUCING PAIN OF THIS TYPE. • SOMATIC PAIN, ARISING FROM MUSCLE OR BONE, INTENSIFIED BY SPRAINS, HEADACHES, AND ARTHRITIS, IS REDUCED BY THE SALICYLATES (ASPIRIN). • ONE CAN ALSO CATEGORIZE PAIN RELATED TO TYPES OF NEURONS THAT CARRY THE SIGNAL. • BRIGHT, SHARP PAIN IS MEDIATED BY LARGE FAST NEURONS THAT SEEMS TO ACTIVATE THE INDIVIDUAL, UNTIL ACHING PAIN WHICH DEPRESSES THE PERSON AND CAUSES ANXIETY IS MEDIATED BY SMALL, SLOW UNMYLENATED NEURONS. • EXAMPLES TO DIFFERENTIATE THESE TWO: HIT YOUR THUMB WITH A HAMMER. THE INITIAL SENSATION IS BRIGHT PAIN, WHEREAS THE THROBBING EXPERIENCE THAT SOON FOLLOWS IS DULL PAIN. • THIRD CLASS OF PAIN EXPERIENCE IS LABELLED BURNING PAIN. NEURONS INTERMEDIATE IN SIZE AND SPEED PRODUCE THIS PAIN. Pain • THE EXPERIENCE OF PAIN IS INCREASED WITH FATIGUE, ANXIETY, FEAR, BOREDOM, AND ANTICIPATION OF MORE PAIN. • INTROVERTS ARE GENERALLY FOUND TO HAVE LOWER PAIN THRESHHOLDS THAN EXTROVERTS. • REDHEADS ARE MORE SENSITIVE TO PAIN THAN BLONDES, WHO ARE MORE SENSITIVE THAN BRUNETTES. • Melanocortin-1 receptor Aspirin SALICYLATES ARE THE MOST WIDELY USED CLASS OF INTERNAL ANALGESICS. THE NAME IS DERIVED FROM THE LATIN SALIX, MEANING WILLOW (FILIPENDULA ULMARIA). 2400 YEARS AGO, THE GREEKS USED EXTRACTS OF WILLOW AND POPLAR BARK OR CORIANDER (CORIANDRUM SATIVUM) IN THE TREATMENT OF PAIN, GOUT, AND OTHER ILLNESSES. ARISTOTLE COMMENTED ON SOME OF THE CLINICAL EFFECTS OF SIMILAR PREPARATIONS. THESE REMEDIES FELL INTO DISREPUTE WHEN ST. AUGUSTINE DECLARED THAT ALL DISEASES OF CHRISTIANS WERE THE WORK OF DEAMONS, AND THUS THE PUNISHMENT OF GOD. • THE AMERICAN INDIANS USED A TEA BREWED FROM WILLOW BARK TO REDUCE FEVER. • THE SALICYLATES WERE NOT REDISCOVERED IN EUROPE UNTIL ABOUT 1763, WHEN AN ENGLISHMAN, REV. EDWARD STONE, PREPARED AN EXTRACT OF WILLOW BARK AND GAVE THE SAME DOSE TO 50 PATIENTS WITH VARYING ILLNESSES AND FOUND THE RESULTS TO BE “UNIFORMLY EXCELLENT.” • IN THE 19TH CENTURY, ACTIVE INGREDIENTS IN THESE PREPARATIONS WAS ISOLATED AND IDENTIFIED AS SALICYLIC ACID. Aspirin • IN 1838, SALICYLIC ACID WAS SYNTHESIZED, AND IN 1859 IT WAS MADE IN BULK PRODUCTIONS. AT THAT TIME, IT WAS PRIMARILY USED FOR THE TREATMENT OF ARTHRITIS. • IN 1890, AT BAYER LABORATORIES IN GERMANY, A CHEMIST, DR. HOFFMANN TREATED HIS FATHER FOR RHUMATORY ARTHRITIS. • HOWEVER, THE DRUG PRODUCED GREAT GASTRIC DISCOMFORT. • HOFFMANN IN 1898 SYNTHESIZED ACETYLSALICYLIC ACID. THIS AGENT PRODUCED RELIEF FROM PAIN WITHOUT STOMACH UPSET. • THIS AGENT HAD BEEN ACTUALLY SYNTHESIZED SOME 45 YEARS EARLIER, BUT WAS NEVER TESTED CLINICALLY. • THE COMPOUND WAS TESTED, PATENTED, AND RELEASED FOR SALE AUGUST 10, 1897 UNDER THE NAME ASPIRIN. • IN 1915, THE BAYER ASPIRIN APPEARED FOR THE FIRST TIME, AND ASPIRIN BECAME A NONPRESCRIPTION ITEM. • TODAY THERE ARE OVER 300 ASPIRIN CONTAINING PRODUCTS ON THE AMERICAN MARKET. THERAPEUTIC USE ASPIRIN HAS 3 MAIN EFFECTS: 1. ANALGESIC: BLOCKS SOMATIC PAIN IN THE MILD TO MODERATE RANGE. 2. ANTIPYRETIC: REDUCES BODY TEMPERATURE WHEN ELEVATED BY FEVER. 3. ANTI-INFLAMMATORY: REDUCES INFLAMATION IN AN INJURED AREA. THIS ACTION IS THE BASIS FOR ITS USE IN ARTHRITIS. Mechanism of Action of Aspirin ASPIRIN MODIFIES THE CAUSE OF PAIN. WHEN CELL MEMBRANES ARE DAMAGED OR INJURED, PROSTOGLANDINS ARE LOCAL HORMONES THAT ARE RELEASED. THESE AGENTS ACT ON THE ENDINGS OF NEURONS THAT MEDIATE PAIN IN THE INJURED AREAS. PROSTOGLANDINS SENSITIZE THE NEURONS TO MECHANICAL STIMULATION AND TO STIMULATION BY HISTAMINE Mechanism of Action of Aspirin ASPIRIN BLOCKS THE SYNTHESIS OF PROSTAGLANDINS. PROSTOGLANDINS ARE STORED BUT ARE RAPIDLY SYNTHESIZED AND RELEASED FROM CELLS WHEN INJURY OCCURS. THEY SENSITIZE NEURONS TO PAIN AND TO OTHER LOCAL HORMONES. • THEREFORE NERVE IMPULSES ARE NOT INITIATED IN THE PAIN PATHWAYS BY BRADYKYNINS OR HISTAMINE. • ASPIRIN DOES NOT BLOCK PAIN PRODUCED BY INJECTIONS OF PROSTAGLANDINS. • ASPIRIN'S ANALGESIC EFFECTS ARE ONLY ON TISSUES WHERE PROSTAGLANDIN FORMATION OCCURS • ASPIRIN'S REDUCES BODY TEMPERATURE (FEVER) BY BLOCKING SYNTHESIS OF PROSTOGLANDINS IN THE ANTERIOR HYPOTHALAMUS. • THE THERAPEUTIC DOSE IS USUALLY CONSIDERED TO BE BETWEEN 600 TO 1,000 MG; 300 MG. IS USUALLY MORE EFFECTIVE THAN A PLACEBO OF 600 MG., CLEARLY EVEN MORE EFFECTIVE. • ABOVE 600 MG, THE ANALGESIC ACTION OF ASPIRIN DOES NOT SEEM TO INCREASE, ALTHOUGH THIS QUESTION HAS NOT BEEN RESOLVED. • OLDER PATIENTS NEED LESS ASPIRIN TO OBTAIN THE SAME BLOCK OF PAIN. DISTRIBUTION ASPIRIN CAN BE ABSORBED FROM THE STOMACH, BUT IS MUCH FASTER FROM THE INTESTINE. THEREFORE, ANYTHING THAT DELAYS THE MOVEMENT OF ASPIRIN FROM THE STOMACH WOULD EFFECT ABSORPTION TIME. MEALS TEND TO DELAY EMPTYING OF THE STOMACH, AND THEREFORE MAY DELAY THE ONSET OF ACTION. A WATER SOLUTION OF ASPIRIN IS MORE RAPIDLY ABSORBED THAN THE TABLET FORM, THUS GIVING HIGHER AND EARLIER EFFECTIVE BLOOD LEVELS OF THE DRUG. BUT RAPID ABSORPTION DOES NOT CORRELATE WITH RAPID ANALGESIA. METABOLISM ASPIRIN, WHICH IS ACETYLSALICYLIC ACID, IS CONVERTED EITHER IN THE GASTROINTESTINAL TRACK OR IN THE BLOODSTREAM TO ITS ACTIVE FORM, SALICYCLIC ACID. TAKEN ORALLY, ASPIRIN IS MORE POTENT AN ANALGESIC THAN SALCYLIC ACID, SINCE ASPIRIN IRRITATES THE STOMACH LESS AND IS ABSORBED MORE RAPIDLY. METABOLISM • IT IS INTERESTING TO COMPARE TWO COMPOUNDS INTRODUCED BY BAYER LABORATORIES IN GERMANY AT THIS TIME. • BOTH ARE RAPIDLY TRANSFORMED TO THEIR ORIGINAL FORM AFTER ABSORPTION. HEROIN, WHICH IS DIACETYLMORPHINE, AND ASPIRIN, WHICH IS ACETYLSALICYLIC ACID, ARE CONVERTED EITHER IN THE GASTROINTESTINAL TRACK OR IN THE BLOODSTREAM TO THEIR ACTIVE FORMS. • TAKEN ORALLY, ASPIRIN IS MORE POTENT AN ANALGESIC THAN SALCYLIC ACID, SINCE ASPIRIN IRRITATES THE STOMACH LESS AND IS ABSORBED MORE RAPIDLY. Acetylsalicylate - Aspirin LATENCY OF ONSET INGESTION OF 650 MG TABLET OF ASPIRIN, HEADACHE AND POSTPARTUM PAIN WERE NOT REDUCED SIGNIFICANTLY FROM PLACEBO UNTIL 45 MIN HAD ELAPSED. MAXIMUM RELIEF WAS OBTAINED AFTER 60 MIN. AFTER 4 HRS., PAIN LEVELS WERE EQUIVALENT IN DRUG AND PLACEBO GROUPS, I.E., ANALGESIA WAS GONE. AT 45 MIN TO 4 HR THE LEVELS OF SALICYLATE IN THE BLOOD WAS THE SAME. IT WAS DETERMINED, THEREFORE, THAT THE BLOOD LEVEL OF 30 UG/ML IS THE THRESHHOLD FOR ANALGESIA. MAXIMUM RELIEF IS OBTAINED AT 40 UG/ML. EFFECTIVENESS ASPIRIN DOES NOT BLOCK ALL TYPES OF PAIN. IT IS ESPECIALLY EFFECTIVE AGAINST HEADACHE AND MUSCULO-SKELETAL ACHES AND PAINS, LESS EFFECTIVE FOR TOOTHACHE AND SORE THROAT, AND MOST USELESS IN VISCERAL PAIN AS WELL AS IN TRAUMATIC OR ACUTE PAIN. ANTIPYRETIC ACTIONS ASPIRIN DOES NOT LOWER THE TEMPERATURE OF A NORMAL INDIVIDUAL. ONLY WORKS IN PERSON WITH FEVER, I.E. LAW OF INITIAL VALUE. ASPIRINS WORK ON THE TEMPERATURE REGULATING AREA OF THE HYPOTHALAMUS TO INCREASE HEAT LOSS THROUGH PERIPHERAL MECHANISMS. THIS IS ATTAINED PRIMARILY BY INCREASED VASODILATION OF PERIPHERAL BLOOD VESSELS AND INCREASED PERSPIRATION. HEAT PRODUCTION IS NOT CHANGED, BUT HEAT LOSS IS FACILITATED. Thermo-regulation of body temperature Involves autonomic nervous, endocrine, and skeletomotor systems Body temperature detectors Peripheral: skin, spinal cord, viscera Central: anterior hypothalamus Body temperature effectors Heat retention or generation: posterior hypothalamus Heat dissipation: anterior hypothalamus • Heat dissipating mechanisms – Dilation of blood vessels in the skin – Inhibition of shivering • Heat conserving mechanisms – Vasoconstriction of blood vessels in the skin – Shivering – Increased secretion of thyroxin Response to Cold Response to Heat Aspirin enhances the loss of heat from the body ADVERSE SIDE EFFECTS ASPIRIN INCREASES BLEEDING TIME BY INHIBITING BLOOD PLATELET AGGREGATION. 2 OR 3 ASPIRINS CAN DOUBLE BLEEDING TIME. THIS EFFECT MAY LAST 4 TO 7 DAYS. THE RELATIONSHIP BETWEEN ASPIRIN USE AND A DECREASE IN HEART ATTACKS WAS ORIGINALLY OBSERVED IN A GROUP OF RHUMATORY ARTHRITIS PATIENTS. THESE PATIENTS HAD ABOUT 1/5 AS MANY HEART ATTACKS AS WOULD BE EXPECTED. THIS FEATURE OF ASPIRIN HAS BOTH GOOD AND BAD SIDE EFFECTS. GENERALLY, HOWEVER, ASPIRIN IS NOT RECOMMENDED 7 TO 10 DAYS BEFORE UNDERGOING SURGERY. • SECOND POINT, INJESTION OF ASPIRIN IN DOSES OF 1 TO 3 GM PER DAY WILL INDUCE ACULT GASTROINTESTINAL BLEEDING IN ABOUT 70% OF NORMAL SUBJECTS. • THIS AMOUNTS TO 5 ML OF BLOOD PER DAY, WHICH IS 5 TIMES THE NORMAL LOSS OF BLOOD VIA THE GASTROINTESTINAL TRACK. • IN SOME PEOPLE, THIS BLOOD LOSS MAY BE GREAT ENOUGH TO CAUSE ANEMIA. • BASIS FOR THIS FACT IS BELIEVED TO BE A DIRECT ERODING BY ASPIRIN ON THE GASTRIC MUCOSA LAYER. THEREFORE, DRINK LOTS OF WATER WHEN TAKING ASPIRIN. BETTER YET, CRUSH THE ASPIRIN AND TAKE THEM IN ORANGE JUICE OR OTHER LIQUID. • THIRD POINT, ASPIRIN USE INCREASES THE NUMBER OF VIRUSES PRODUCED IN SUFFERERS OF THE COMMON COLD. • WHAT THIS MEANS IS THAT ASPIRIN IS MORE LIKELY TO LEAD TO THE SPREAD OF GERMS OR FOR THE USER TO REINFECT HIMSELF THAN AS A NON-ASPIRIN USER. • FOURTH POINT, ASPIRIN IS THE NUMBER ONE CAUSE OF ACCIDENTAL POINSONING DEATH IN CHILDREN UNDER 5 YEARS OF AGE. • HOUSEHOLD PLANTS AND HOUSEHOLD SOAPS ARE FIRST AND SECOND CAUSES OF NON-FATAL ACCIDENTAL POISONING IN YOUNG CHILDREN. ASPIRIN IS THE FIRST CAUSE OF MORTALITY IN THE YOUNG. • USUALLY, THE POISONING AGENT IS "BABY ASPIRIN." ANTI-INFLAMMATION • THIS IS THE MAJOR USE FOR ASPIRIN IN THE NATION. PATIENTS WITH RHUMATORY ARTHRITIS MAY CONSUME 3,000 MG TO 4,000 MG PER DAY. LATENCY OF ONSET • WHEN BUYING ASPIRIN TABLETS, ONE MUST CONSIDER THAT THE TABLETS DEVELOP A HARDER EXTERNAL SHELL THE LONGER THEY SIT. • THIS DOES NOT EFFECT OR CHANGE THE AMOUNT OF ACTIVE INGREDIENT, BUT IT DOES MAKE THE ACTIVE INGREDIENT LESS EFFECTIVE BECAUSE DISINTEGRATION TIME IS INCREASED. • ALSO, MOISTURE AND HEAT SPEED DECOMPOSITION OF ACETYLSALICYLIC ACID INTO SALICYLIC ACID WHICH CAUSES GASTRIC DISTRESS, AND ACETIC ACID. • WHEN ASPIRIN BOTTLES SMELL LIKE VINEGAR, THEY SHOULD BE DISCARDED. • ACETAMINOPHEN (TYELNOL) IS EQUIPOTENT WITH ASPIRIN AS AN ANALGESIC MECHANISM OF ACTION • THE ANTIPYRETIC AND ANALGESIC MECHANISM IS SIMILAR TO THAT OF ASPIRIN, I.E. BY INHIBITION OF PROSTAGLANDIN SYNTHESIS. • ACETAMINOPHEN IS NOT ANTI-INFLAMMATORY AND THUS IS OF MINIMAL VALUE IN ARTHRITIS, GOUT, ETC. • ACETAMINOPHEN ACUTE TOXICITY CAN OCCUR IN ADULTS TAKING 7 GM. 14 GM CAUSE REVERSABLE DAMAGE TO THE LIVER. MORE THAN 14 GM MAY LEAD TO HEPATIC COMA, AND POSSIBLY TO DEATH. • IBUPROFEN IS AN NSAID, OR NONSTEROIDAL ANTI-INFLAMMATORY DRUG. • BLOCKS CYCLOOXYGENASE ACTIVITY - INHIBITION OF PROSTAGLANDIN SYNTHESIS. EXACT MECHANISM UPON COX ENZYME IS NOT KNOWN. • ACTIONS OF ALL NSAIDS • THEY SUPPRESS THE NOCTURNAL SURGE IN MELATONIN SYNTHESIS. • THEY ALSO ATTENUATE THE NIGHTTIME DECREASE IN BODY TEMPERATURE. • THESE ALTERATIONS MAY INFLUENCE SLEEP PATTERNS. • THEY PRODUCE ADVERSE REACTIONS IN GI TRACT, E.G. BLEEDING AND PERFORATION OF BOWELS. • NEXT GENERATION OF NSAIDS TARGETED ONLY THE TYPE II CYCLOOXYGENASE WHICH SHOULD HAVE AFFECTED INFLAMMATION BUT NOT THE GI TRACT. COX-2 selective inhibitors are associated with an increased incidence of serious adverse events as compared to non-selective NSAIDs. Anti-Histamines Histamine containing neurons are a part of the Brain’s Ascending Arousal Systems Histamine Origin: tuberomammillary nucleus of hypothalamus projects widely. Functions: sleep-wake cycle, arousal. Antihistamine medications used to treat allergies are thought to cause drowsiness by blocking CNS histamine receptors. During NonREM sleep, GABA neurons inhibit histamine neurons. This reduces histamine activation of forebrain and reduces activation of cholinergic neurons (like scopolamine). -leading to sleep. -Anti-histamines therefore lead to sleepiness. Many OTC anti-histamines also block acetylcholine muscarinic receptors in the brain. – also leading to sleepiness. HERBALS Gingko: The Single Most Popular Brain-specific Nutrient. The theory: as we age, tissue damaging free radicals become more prevalent and cause age-related loss of neurons. • Ginkgo may neutralize these chemicals. • Gingko may increase function of acetylcholine neurons. • Three good research studies with doubleblind design. • Two smaller studies found that gingko slightly improved memory. Gingko: The Single Most Popular Brain-specific Nutrient. Patients had significant memory problems caused by mild to moderate AD or strokerelated dementia. Almost two-thirds of patients did not complete the first study. If all the subjects had completed the study the authors speculated that the effects would have washed out. Overall, the improvement in cognitive function scores are small, variable and required 4-6 weeks to appear. • Use of Ginkgo Biloba can be traced back centuries in Chinese traditional medicine • Most widely-used herbal treatment for cognitive functions – memory, learning, alertness • Approved in Germany for dementia treatment • NIH is supporting a clinical trial of Ginkgo Biloba in Alzheimer's • Typical dose (used in many experiments) is 120 milligrams of dried extract in two or three oral doses. • Extract in German product is named EGb 761, manufactured by Schwabe Pharmaceuticals. • The extract contains – flavonoids and biflavonoids, a large group of natural plant products – terpenes (active ingredients in catnip and marijuana) • Dozens of clinical trials have examined the cognitive effects of gingko in humans. • Great majority of studies have involved subjects with mild to moderate impairment, usually an early diagnosis of Alzheimer's. • Most experiments test learning and memory; less often attention, motivation or anxiety. • Most subjects were selected and tested long after they began using gingko, typically several months, so their cognitive level before using gingko is unknown. • This may introduce a bias, if those with better cognitive abilities are more likely to take gingko. • For example, higher scores on the memory and learning tests may come from subjects who could read and understood articles suggesting gingko might help them, or who were better able remember to take the drug. • Researchers need to give tests both before and after the patients start taking gingko, or else the experiment results are suspect. • Another recent, large, well-controlled clinical trial of EGb 761 sponsored by its manufacturer involved patients with mild or moderate dementia. • The results showed no "systematic and clinically meaningful effect of gingko" on any of the cognitive tests used. Improvement in ADAS-cog Efficacy of Ginko Biloba 4 3 2 1 0 -1 0 12 26 39 52 -2 -3 -4 Weeks of Double-Blind Medication Le Bars et al. JAMA: 1327, 1997 Placebo (n=157) 24 mg (n=131) Solomon et al., JAMA, Aug, 2002 Is gingko safe? • Few health risks at typical doses (120 to 240 milligrams per day) • Some complications have occurred in people taking gingko: – subdural hematomas (blood clots between skull and brain) – gastrointestinal problems – nausea and vomiting Scientific American, April, 2003 Potatoes, tomatoes & Eggplants Contain two solanaceous glycoalkaloids: a-Solanine and α-chaconine Inhibit acetylcholinesterase and butyrylcholinesterase leading to an elevation of synaptic levels of acetylcholine. GINSENG Widely used to improve overall energy and vitality, particularly during times of fatigue or stress. While there is not much clinical evidence to support an energy boosting effect, there are studies showing its potential value in normalizing glucose levels after meals in diabetics, stimulating immune function and symptoms of attention deficit-hyperactivity disorder (ADHD) in children. Ginsenosides may underlie ginseng's bioactivity. Polluted and Diluted 2003 studies: A high amount of the pesticide hexachlorobenzene — a potential human carcinogen — was found in one of five products labeled as containing "Korean Ginseng." Levels of two other pesticides, quintozene and lindane — were also above acceptable levels. "Chinese Ginseng" labeled "EXTRA STRENGTH" contained less than 10% of the expected ginsenosides. Single doses of Panax ginseng (G115) reduce blood glucose levels and improve cognitive performance during sustained mental activity. J Psychopharmacol, 2005; 19: 357 - 365. Numerous potential mechanisms of action upon a variety of neural systems, e.g. acetylcholine, bioamines, nitric oxide, calcium channels and steroids. The lack of unanimity in the research (on Ginseng use in humans) can be explained on the basis of various methodological problems such as inadequate sample size and lack of double-blind, control and placebo paradigms. Report to NIH in 2000. Vinpocetine: Extract From the Periwinkle Plant May increase blood flow and circulation in the brain and increase neuronal glucose transport and uptake. • May stimulate the acetylcholine neural activity. • May reduce the loss of neurons due to decreased blood flow (ischemia). Vinpocetine: Extract From the Periwinkle Plant Two good studies: • Older adults with memory problems associated with either circulation problems or mild-moderate dementia. • Patients given vinpocetine showed modest to very modest (3 points over 13 wks on the Mini-Mental) vs placebo for tests measuring attention &memory. Vinpocetine: Extract From the Periwinkle Plant • In a larger study, 16 wks of therapy gave patients just a one point gain in memory and concentration vs. placebo. • Evidence for cognitive benefits of vinpocetine is similar to that for Gingko. Statistically significant improvements in a only few studies with benefits that are very modest at best and tend to disappear in larger studies. NADH • NADH is abundant in meat, less so in fruits & vegs. • NADH levels tend to decrease slightly with aging. • Open label trial, 17 AD. No controls. 8-12 wks, 10 mg/day, p.o., by Jorg Birkmayer, MD, Austria. • WEB Site: Within 2 wks, “noticeable improvements in cognitive function, increased production of norepinephrine and dopamine.” “remarkable improvements in cognition” “No negative sideeffects.” • 1996 Publ: “This represents a pilot study from which no definitive conclusion can be drawn.” Patent Holder? Dr. Jorg Birkmayer. Fava Beans BBB L-DOPA is a precursor to the production of Dopamine in the brain OTC Strategies for Enhancing Cognition Via Neuroprotectants • Anti-Oxidants to protect us from the consequences of breathing oxygen Probability of dying from any cause Data for 1,000,000 people OXYGEN: A Pro-Aging Molecule • The risk is simply being alive, e.g. breathing, eating, exercising… • 2% of oxygen used in energy metabolism forms oxygen free radicals that are toxic and may damage DNA. • The complement of anti-oxidant systems your species possesses is directly related to how long your species lives. Effect of Caloric Restriction Fewer cancerous tumors among those on restricted diets 50 Normal Diet (control group) Caloric Restrictions 45 40 30 20 15 11 9 10 2.1 0 Hepatoma 1 Lymphoma All Tumors Degenerative Diseases Control Rats vs. Restricted Rats % Degenerative Disease 100 95 Normal Diet (control group) Caloric Restrictions 80 75 80 55 60 35 40 25 19 18 20 0 Kidney Muscle Heart Disease Type Vascular Vitamin E Vitamin E is an anti-oxidant that easily crosses the Blood Brain Barrier. • The theory: by neutralizing chemicals that kill neurons, vitamin E may slow memory decline due to aging or brain diseases. • Beneficial Effects of Vitamin E. The largest and best study on vitamin E investigated patients with moderate AD. Vitamin E • 2000 IU/day delayed by about 9 months the entry into a nursing home. Patients did not lose daily living skills as rapidly as patients given the placebo. • Vitamin E did not halt the speed of memory decline! • FDA has not approved use of vitamin E for treatment of AD because it did not slow cognitive and memory decline. Effects of Vitamin-E and Selegiline on Institutionalization, Loss of ADLs, StageChange or Death Percent Event-Free 120 100 80 Placebo Selegiline Vitamine E 60 40 20 0 0 100 200 300 400 Days of Study 500 600 700 CAFFIENE CAFFIENE (1,3,7-TRIMETHYLXANTHINE) SIMILAR TO PURINE. COFFEE, CHOCOLATES AND TEA. IMPORTS INTO USA, CRUDE COFFEE 3,000,000,000 LBS/YR. HISTORY USED IN CHINA FOR MEDICAL AND RELIGIOUS PURPOSES FOR MANY CENTURIES. THE HISTORY OF COFFEE AND CAFFEINE CONTAINING BEVERAGES IN THE WESTERN WORLD PROVIDES A WONDERFUL EXAMPLE ON HOW SOCIETY AND MEDICINE RESPOND TO MILDLY PSYCHOACTIVE SUBSTANCES. THE STIMULANT EFFECTS OF CAFFEINE WERE CALLED A PANACEA AND THE SOLUTION FOR MAN'S MENTAL STRESS BY MANY; BUT WERE DENOUNCED BY OTHERS. WORLDWIDE USE OF CAFFEINE: S. AMERICANS PREPARE DRINKS FROM MATE LEAVES, YOCO, AND GUARANA. W. AFRICANS CHEW ON KOLA NUTS. IN 1800'S ALL OF THESE WERE FOUND TO CONTAIN CAFFEINE. DAILY INTAKE: U.S. 2.5 MG/KG BODY WEIGHT; EUROPEANS 3.5 MG/KG OR ABOUT 165 MG/DAY IN U.K.; 246 MG/DAY IN U.S.; OR 465 MG/DAY IN FINLAND. TODAY, COFFEE COVERS 44 PERCENT OF THE PERMANENT ARABLE CROPLAND IN NORTHERN LATIN AMERICA. INTERPLANETARY: THE APOLLO 11 ASTRONAUTS WERE DRINKING COFFEE 3 HOURS AFTER LANDING ON THE MOON. SOURCE: CAFFEINE IS FOUND IN AT LEAST 63 PLANT SPECIES, BUT 54% OF WORLD'S CONSUMPTION DERIVES FROM TWO DIFFERENT BEANS OF COFFEA ARABICA AND COFFEA ROBUSTA AND 43% FROM THE TEA PLANT Camellia sinensis. C. MAURITIANA AND C. HUMBOLTIANA HAVE NO CAFFEINE. DOSE: 1 MG/KG AVERAGE CUP OF COFFEE INSTANT COFFEE HAS 60-70 MG; BREWED HAS 100 MG; ESPRESSO (100 MG); DRIP HAS 150 MG; DECAF (2-4 MG). MINIMUM STIMULANT DOSE IS BETWEEN 85 AND 250 MG. TEA: BUDS HAVE GREATEST CAFFEINE CONTENT. BLACK TEA HAS ABOUT 40 MG; GREEN TEA ABOUT 35 MG. DEPENDS METHOD OF PREPARATION AND VARIETY OF TEA USED. ICED TEA HAS ABOUT 70 MG. WHITE TEA (STEAMED RATHER THAN FERMENTED OR ROASTED) MAY CONTAIN MORE. CHOCOLATE (1 OZ BAR) CONTAINS 75-150 MG OF METHYLXANTHINE (90% AS THEOBROMINE). HAS LOW LIPID SOLUBILITY SO WEAK CENTRAL ACTIONS. EXPRESSO HAS LESS CAFFIENE THAN PEPSI COLA DUE TO WAY ITS PREPARED AND DRANK JOLT COLA (100 MG); SUGAR-FREE MR. PIBB (59 MG); MELLOW YELLOW (52 MG); MOUNTAIN DEW(53 MG), COKE (45 MG); PEPSI (36 MG). Coffee is rich in biologically active substances such as trigonelline, quinolinic acid, tannic acid, pyrogallic acid and, of course, caffeine. Niacin in particular is formed in great amounts from trigonelline during the coffee-bean roasting process (Czok, 1977; Casal et al. 2000). The amount of niacin can vary from 2 to 80 mg/100 g coffee. Coffee is a rich source of antioxidants (caffeic, chlorogenic, coumaric, ferrulic and sinapic acids). A by-product of coffee-bean roasting, silverskin, has marked antioxidant activity. The caffeine content of caffeinated coffees ranges from 58 to 259 mg/dose. In one study, the mean caffeine content of brewed specialty coffees was 188 mg for a 16 oz cup. Variability is high. McCusker et al. (2003) reported a wide range of caffeine concentration (259–564 mg/dose) in the same coffee beverage obtained from the same outlet on six consecutive days. EFFECTS ON SLEEP 2 CUPS WILL DOUBLE SLEEP LATENCY WITH 150 MG DOSES (I.E. A SINGLE CUP OF COFFEE). 100 MG IS MINIMUM DOSE TO DETECT AN EFFECT OF CAFFEINE. HEAVY DRINKERS ARE IMMUNE TO THIS SLEEP LATENCY EFFECT. CAFFEINE INCREASES STAGE 2 SLEEP TIME, DECREASES STAGES 3 & 4 SLEEP. NO EFFECT ON REM (DREAM) SLEEP Effects of major xanthine derivatives Major Source CNS Heart Diuretic Theophylline Tea Moderate Potent Potent Caffeine Coffee Potent Moderate Moderate Slight Minimum Slight Theobromine Coco nut Elements found in tea leaves Aluminum, arsenic, boron, calcium, copper, iron, flourine, mercury, iodine, manganese, molybdenum, sodium, nickel, phosphorus, lead, potassium, selenium, silicon, sulfur & zing. Cellular Defense and Carcinogenesis Section CH3 O HO OCH33 CH=CHCOCH22COCH=CH Kaempferol, Quercetin OH Curcumin, DBM Galangin Resveratrol Diosmetin, Diosmin CAFFEINE PASSES VERY QUICKLY INTO THE BRAIN. BRAIN UPTAKE INDEX (BMI) NICOTINE ETHANOL COCAINE WATER CAFFIENE HEROIN PHENOBARBITAL MORPHINE ASPIRIN 131 (ONLY ONE PUFF) 104 100 100 90 68 22 2.6 1.8 80% OF CAFFIENE IS REMOVED BY BRAIN IN SINGLE PASS. CAFFEINE IN CSF REACHES 1/2 ITS PLASMA LEVELS IN 48 MINUTES. BRAIN LEVELS REMAIN STABLE FOR 1 HOUR. 2 GROUPS OF PEOPLE IN US. 80% WHO USE COFFEE AND 20% WHO AVOID IT. HIGH CONSUMERS AND LOW CONSUMERS. RESPOND VERY DIFFERENTLY TO CAFFIENE. HIGH CONSUMERS SHOW LESS EFFECT ON SLEEP THAN LOW CONSUMERS. PHYSIOLOGY: ONLY NEED 5 UG/ML INCREASE IN BLOOD LEVEL TO FEEL EFFECTS. MOST DRINKERS TITRATE THEIR BLOOD LEVELS FROM 1-3 UG/ML OF CAFFIENE. 10 UMOLAR BRAIN CAFFIENE IS EXPERIENCED BY 80% OF ALL N.AM PEOPLE FROM EMBRYO TO DEATH. PEAK LEVELS IN 15-30 MIN AFTER DRINKING FIRST SIP. I.E. BEFORE THE CUP IS FINISHED USUALLY. LETHAL LEVEL IS 500 uM IN BLOOD. LETHAL DOSE IS 5-10 GRAMS, ORAL OR IV. THIS IS ABOUT 75 CUPS OF COFFEE. SMOKING INCREASES CAFFIENE HALF-LIFE FROM 3 HRS (I.E. NORMAL) TO 6 HRS. LITTLE PROTEIN BINDING. TOLERANCE DEVELOPS TO SOME PERIPHERAL SYMPTOMS; SLOWER TO CENTRAL EFFECTS. DOWNREGULATION OF ADENOSINE TYPE-2-a RECEPTORS AND UPREGULATION OF ADENOSINE TYPE-1 RECEPTORS IN AMYGDALA – THE EMOTIONAL PART OF THE LIMBIC SYSTEM WITHDRAWAL: HEADACHE - "WEEKEND TENSION HEADACHES" MAY BE DUE TO LARGE COFFEE INTAKE DURING WORKWEEK, THEN WITHDRAWAL ON WEEKENDS. LARGE DOSES: MOOD CHANGES, NERVOUSNESS, IRRITABILITY, LACK OF ALERTNESS. 1 GM (7-10 CUPS) CAFFIENE: INSOMNIA, WEARINESS, ANXIETY, RESTLESSNESS, SENSORY DISTURBANCES SUCH AS RINGING IN THE EARS, MUSCLE TENSENESS, WEAKNESS, TREMOR, CARDIAC IRREGULARITIES, EXACERBATION OF ULCERS, DIARRHEA, NAUSEA, APATHY. REPORT ON WOMEN WITH FIBROCYSTIC BREAST DISEASE: FINDING-- ABSTENTION FROM CAFFEINE RESULTED IN DISAPPEARANCE OF SYMPTOMS. PREGNANCY AND CHILDREN ORAL CONTRACEPTIVES WILL DECREASE METABOLISM OF CAFFIENE. LIVER P450 SYSTEM IS ESTROGEN SENSITIVE. HALF-LIFE FOR WOMEN IN LAST TRIMESTER IS 10.5 HOURS. PREGNANT WOMEN ARE ESTIMATED TO CONSUME 144 MG/DAY. BREAST FEEDING HAS INCREASED FROM 24.7% IN 1971 TO 55.3% IN 1980. CAFFEINE IS RAPIDLY TRANSMITTED INTO BREAST MILK. BREAST MILK CAFFIENE IS SAME AS MOTHER'S PLASMA LEVELS. STUDY OF 6 HEALTHY LACTATING WOMEN (AGES 28 35): 100 MG DOSE OF CAFFEINE IN WATER ON EMPTY STOMACH. BLOOD AND BREAST MILK WAS SAMPLED FOR NEXT 24 HRS. PLASMA PEAK TIME WAS 0.5 TO 1 HOUR. LEVELS WERE 3.6 TO 6.1 UG/ML. BREAST MILK PEAK TIME WAS 0.75 TO 2 HR. LEVELS WERE 2.0 TO 4.3 UG/ML. IN A PRETERM INFANT WITHOUT LIVER FUNCTION, I.E., WITHOUT METABOLISM, THE HALF-LIFE WOULD BE 80 100 HOURS. IT IS DIFFICULT TO FIND A NEWBORN BABY WITHOUT CAFFEINE IN ITS BLOOD! THEOPHYLLINE (IN TEA) HALF-LIFE IS 77 + 65 HOURS IN PRETERM INFANTS. FETAL LIVER CAN CONVERT THEOPHYLLINE TO CAFFEINE! BEGINNING IN 3RD TRIMESTER, BABY BRAIN REACTS TO CAFFIENE JUST LIKE ADULT BRAIN. RECEPTORS MUST BE THERE? CAFFEINE AT VERY HIGH DOSES (80 CUPS/DAY) IS A TERATOGEN. XANTHINES HAVE A POSITIVE INOTROPIC EFFECT ON THE HEART XANTHINES ARE DIURETICS (BLOCKS NA+ AND K+ REABSORPTION, LOSS OF WATER IS PURPOSE OF CAFFEINE IN OTC WEIGHT LOSS PILLS) CAFFEINE IS USEFUL IN MIGRAINE HEADACHES (CAFERGOT): INCREASES VASODILATION IN PERIPHERY, DECREASES VASODILATION IN CNS, INCREASES GLUCOSE UTILIZATION (INCREASED NEURONAL ACTIVITY). BENEFICIAL EFFECTS: ENHANCES MENTAL CLARITY, ALLAYS FATIGUE. CAFFEINE IS MOST EFFECTIVE IN IMPROVING PERFORMANCE WHICH HAS BEEN DETERIORATING DUE TO EXCESSIVE STRESS OR FATIQUE. IT HAS LESS DRAMATIC EFFECTS ON WELL RESTED SUBJECTS. THIS IS DUE TO THE LAW OF INITIAL VALUE. Coffee melanoidins showed higher antioxidant activity than melanoidins isolated from beer (Morales & Jimenez-Perez, 2004). Coffee is the main contributor of dietary antioxidant intake in the diet in the USA (Svilaas et al. 2004). There is an inverse association between coffee consumption and liver cirrhosis (Tverdal & Skurtveit, 2003). Total testosterone was positively associated with coffee consumption in adult men. The consumption of at least one cup of coffee per day was associated with a higher prevalence of sexual activity in elderly women and with a higher potency rate in elderly men. Coffee consumption protects women from the development of diabetes (Rosengren et al. 2004). Long-term coffee consumption is associated with a statistically significant lower risk of type 2 diabetes. Regular caffeine use (250 mg twice daily) might have the potential to reduce the risk of cardiovascular events in patients with longstanding type 1 diabetes. The combination of coffee and exercise elicited a higher lipolytic response than exercise alone (Mougios et al. 2003). A study of 87,000 registered female nurses found a strong inverse association between coffee intake and risk of suicide. Coffee (or caffeine from non-coffee sources), but not decaffeinated coffee, has been associated with a low relative risk of Parkinson’s disease (Ascherio et al. 2001; Ross et al. 2000). However, this association is an inverse one for women using hormones (Ascherio et al. 2003). Coffee consumption was also associated with a slightly reduced risk of Alzheimer’s disease (Lindsay et al. 2002; Heuser, 2003). CAFFEINE AFFECTED THE MEMORY ABILITIES OF HIGHLY IMPULSIVE PEOPLE MORE THAN LOW IMPULSIVE PEOPLE. (PSYCHOPHARM. 1991; 105:137.) INCREASES VIGILANCE, PREVENTS DECLINE IN ATTENTION SEEN AFTER MEALS, IMPROVES INFORMATION PROCESSING AFTER LUNCH. RESPONSES ARE QUICKER - INTELLIGENCE IS NOT AFFECTED. WOMEN IN FIRST 5 DAYS OF MENTRUAL CYCLE HAVE ENHANCED MEMORY WITH CAFFEINE DOSE. DRINKING 2 CUPS (TYPICAL) OF COFFEE PER DAY MAY SIGNIFICANTLY SHORTEN THE MENTRUAL CYCLE IN SUSCEPTIBLE WOMEN. CHRONIC CAFFEINE TREATMENT SIGNIFICANTLY REDUCED NEURONAL DAMAGE AFTER 5 MINUTES OF BILATERAL CAROTID OCCLUSION. TEAS CONTAIN POWERFUL ANTI-OXIDANTS, ESPECIALLY WHITE TEA, WHICH IS BETTER THAN GREEN TEA. DRINKING TEAS OR COFFEE MAY REDUCE RISK OF COLON CANCER (DASHWOOD ET AL., 2000). COFFEE OR TEA DRINKING REDUCES THE RISK OF PARKINSON’S DISEASE. DECAFFEINATED DOES NOT HAVE SAME EFFECT. SEEN IN MEN BUT NOT WOMEN. NEUROPROTECTANT EFFECT DOES NOT SHOW TOLERANCE AFTER CHRONIC EXPOSURE (2002). ESTROGEN OR ERT CAN PREVENT THE NEUROPROTECTION IN WOMEN (2006). CAFFEINE AND ATHLETES 450 mg CAFFEINE - NO EFFECT ON SIMPLE COORDINATION IN ADULT MEN. 300-900 MG CAFFEINE - INDUCES ARM AND HAND TREMORS. COFFEE DRINKING CAN EXACERBATE HAND TREMORS ASSOC. WITH PARKINSON'S DISEASE AND LITHIUM THERAPY. STIMULATES RELEASE OF ENDORPHINS AND MAY LESSEN PAIN ASSOC WITH EXERTION WITH EXERCISE. CAFFEINE DOES NOT MODIFY THE DELAY BEFORE EXHAUSTION WITH EXERCISE, BUT IT DOES ATTENUATE THE PERCEPTION OF THE EFFORT REQUIRED. CAFFEINE EFFECTS ARE MORE PRONOUNCED AT HIGH ALTITUDES (2900 METERS), E.G. SKIING. AT HIGH ALTITUDES, CAFFEINE DOES INCREASE DELAY TO EXHAUSTION. AT HIGH ALTITUDES, CAFFEINE INCREASES ENDURANCE BY MOBILIZATION OF FATTY ACIDS. ADVICE FOR ATHLETES:: ABSTAIN FROM CAFFEINE FOR 4 DAYS PRIOR TO EVENT. ABSORB THE CAFFEINE 2-3 HOURS PRIOR TO EFFORT, SO THAT PLASMA FREE FATTY ACIDS, AND NOT CAFFEINE, WILL BE AT PEAK DURING EVENT. NEGATIVE SIDE EFFECTS CNS: GRAND MAL CONVULSIONS CAN BE ELICITED BY CAFFEINE AND THEOPHYLLINE. INCREASES CORTICAL EEG ACTIVITY; DECREASES THALAMIC EEF ACTIVITY: THIS MAY EXPLAIN SLEEP DISTURBANCES. HEART: PREMATURE VENTRICULAR CONTRACTIONS AND SERIOUS ARRHYTHMIAS. AT LOW DOSES, CAFFEINE CAN COUNTERACT THE PSYCHOMOTOR DISTURBANCE OF ALCOHOL. STIMULANT EFFECTS MAY BE MEDIATED BY INHIBITION OF CNS ADENOSINE RECEPTORS ANTAGONISM AT THESE RECEPTORS IMPROVES MENTAL CLARITY AND MOOD. (SCIENCE 263:689, FEB 1994) PROPENSITY TO SLEEP AND INTENSITY OF DELTA WAVES UPON FALLING ASLEEP ARE PROPORTIONAL TO THE DURATION OF PRIOR WAKEFULNESS. RISE IN BRAIN TEMP INDUCES SLEEPINESS AND INCREASED DELTA WAVE ACTIVITY. MESOPONTINE CHOLINERGIC CELLS MAY CONTROL CORTICAL EEG VIA THALAMUS. ADENOSINE MAY MODULATE THE ACTIVITY OF THESE NEURONS. PRODUCTION AND RELEASE OF ADENOSINE IN BRAIN IS LINKED TO NEURONAL METABOLIC ACTIVITY WHILE AWAKE. THEREFORE, ADENOSINE BUILDS UP WHILE BRAIN IS ACTIVE DURING THE DAY AND INHIBITS CHOLINERGIC MESOPONTINE NEURONS THAT ARE IMPORTANT FOR AROUSAL. THIS LEADS TO DECREASED EEG ACTIVITY IN FRONTAL CORTEX, INCREASED DROWSINESS AND DELTA WAVE SLEEP. CAFFEINE AND THEOPHYLLINE ARE POWERFUL BLOCKERS OF ADENOSINE RECEPTORS AND THEREFORE OF THIS ADENOSINE DRIVEN SLEEP. CHOCOLATE HAS MOSTLY THEOBROMINE (3,7DIMETHYLXANTHINE) WITH MUCH LESS CAFFEINE. THEOBROMINE IS A CONSIDERABLY WEAKER CENTRAL STIMULANT THAN CAFFEINE OR THEOPHYLLINE, WHICH HAVE SIMILAR POTENCIES. The Effects of Chocolate Upon Cognition are Due to: 1. Presence of Xanthine 2. Fats induce the release of endogenous opiates 3. Presence of Amphetamine-like drug (PEA) 4. A Marijuana-like drug known as anandamide 5. Presence of Glucose 6. Presence of Estrogen-like compounds 7. Magnesium Salts for post-menopausal women 8. Anti-oxidants, flavonoids = 1 glass of red wine THE END