Bariatric Surgery - 埼玉医科大学総合医療センター 内分泌・糖尿病内科
advertisement

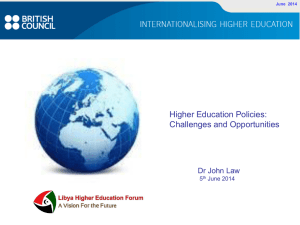
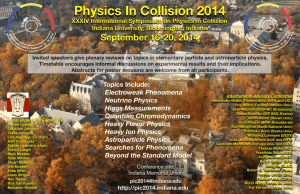
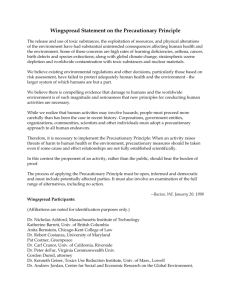
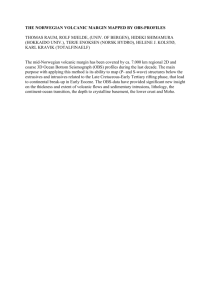
Journal Club Carlsson LM, Peltonen M, Ahlin S, Anveden Å, Bouchard C, Carlsson B, Jacobson P, Lönroth H, Maglio C, Näslund I, Pirazzi C, Romeo S, Sjöholm K, Sjöström E, Wedel H, Svensson PA, Sjöström L. Bariatric surgery and prevention of type 2 diabetes in Swedish obese subjects. N Engl J Med. 2012 Aug 23;367(8):695-704. DIAbetes Genetics Replication And Meta-analysis (DIAGRAM) Consortium Large-scale association analysis provides insights into the genetic architecture and pathophysiology of type 2 diabetes. Nat Genet. 2012 Aug 12;44(9):981-990. doi: 10.1038/ng.2383. Epub 2012 Aug 12. 2012年9月6日 8:30-8:55 8階 医局 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi Bariatric Surgery versus Conventional Medical Therapy for Type 2 Diabetes. 2012年4月5日 n=20 n=20 n=20 Italy N Engl J Med. 2012 Apr 26;366(17):1577-85. 2012年2月2日 Bariatric surgery and long-term cardiovascular events University of Michigan JAMA. 2012;307(1):56-65 2010年8月19日 Hospital complication rates with bariatric surgery in Michigan. University of Michigan JAMA. 2010;304(4):435-442 2009年8月6日 Perioperative safety in the longitudinal assessment of bariatric surgery. University of Washington N Engl J Med. 2009 Jul 30;361(5):445-54. the Institutes of Medicine (L.M.S.C., M.P., S.A., A.A., B.C., P.J., C.M., C.P., S.R., K.S., E.S., P.-A.S., L.S.) and Surgery (H.L.), Sahlgrenska Academy at the University of Gothenburg, and the Nordic School of Public Health (H.W.), Gothenburg, and the Department of Surgery, University Hospital, Orebro (I.N.) — all in Sweden; the Department of Chronic Disease Prevention, National Institute for Health and Welfare, Helsinki (M.P.); and Pennington Biomedical Research Center, Louisiana State University System, Baton Rouge (C.B.). N Engl J Med 2012;367:695-704. Adjustable gastric banding Biliopancreatic diversion Roux-en-Y gastric bypass Sleeve gastrectomy Vertical banded gastroplasty with duodenal switch A meta-analysis from University of California, Los Angeles reports the following weight loss at 36 months Biliopancreatic diversion - 53 kg Roux-en-Y gastric bypass (RYGB) - 41 kg Open - 42 kg Laparoscopic - 38 kg Adjustable gastric banding - 35 kg Vertical banded gastroplasty - 32 kg Sleeve gastrectomy ? BACKGROUND Weight loss protects against type 2 diabetes but is hard to maintain with behavioral modification alone. In an analysis of data from a nonrandomized, prospective, controlled study, we examined the effects of bariatric surgery on the prevention of type 2 diabetes. METHODS In this analysis, we included 1658 patients who underwent bariatric surgery and 1771 obese matched controls (with matching performed on a group, rather than individual, level). None of the participants had diabetes at baseline. Patients in the bariatric-surgery cohort underwent banding (19%), vertical banded gastroplasty (69%), or gastric bypass (12%); nonrandomized, matched, prospective controls received usual care. Participants were 37 to 60 years of age, and the body-mass index (BMI; the weight in kilograms divided by the square of the height in meters) was 34 or more in men and 38 or more in women. This analysis focused on the rate of incident type 2 diabetes, which was a prespecified secondary end point in the main study. At the time of this analysis (January 1, 2012), participants had been followed for up to 15 years. Despite matching, some baseline characteristics differed significantly between the groups; the baseline body weight was higher and risk factors were more pronounced in the bariatric-surgery group than in the control group. At 15 years, 36.2% of the original participants had dropped out of the study, and 30.9% had not yet reached the time for their 15-year follow-up examination. Figure 1. Cumulative Incidence of Type 2 Diabetes. Panel A shows the Kaplan–Meier unadjusted estimates of the cumulative incidence of type 2 diabetes in the bariatric-surgery group and the control group. The light shading represents the 95% confidence interval. The adjusted hazard ratio with bariatric surgery was 0.17 (95% confidence interval, 0.13 to 0.21). Figure 1. Cumulative Incidence of Type 2 Diabetes. Panel B shows the Kaplan–Meier unadjusted estimates of the incidence of type 2 diabetes in subgroups defined in the control group according to receipt or no receipt of professional guidance to lose weight and in the surgery group according to the method of bariatric surgery: gastric banding, vertical banded gastroplasty (VBG), or gastric bypass (GBP). RESULTS During the follow-up period, type 2 diabetes developed in 392 participants in the control group and in 110 in the bariatric-surgery group, corresponding to incidence rates of 28.4 cases per 1000 person-years and 6.8 cases per 1000 person-years, respectively (adjusted hazard ratio with bariatric surgery, 0.17; 95% confidence interval, 0.13 to 0.21; P<0.001). The effect of bariatric surgery was influenced by the presence or absence of impaired fasting glucose (P = 0.002 for the interaction) but not by BMI (P = 0.54). Sensitivity analyses, including end-point imputations, did not change the overall conclusions. The postoperative mortality was 0.2%, and 2.8% of patients who underwent bariatric surgery required reoperation within 90 days owing to complications. CONCLUSIONS Bariatric surgery appears to be markedly more efficient than usual care in the prevention of type 2 diabetes in obese persons. (Funded by the Swedish Research Council and others; ClinicalTrials.gov number, NCT01479452.) Bariatric Surgery — From Treatment of Disease to Prevention? Danny O. Jacobs, M.D., M.P.H. n engl j med 367;8 nejm.764 org august 23, 2012 The current study should provide an impetus to develop a more complete understanding of the mechanisms by which the various bariatric procedures exert their beneficial effects. Such understanding will be important because it will enable the identification of the persons who are the most appropriate candidates for surgery. Message 体格指数(BMI)が男性34以上、女性38以上の肥 満患者3429人を対象に、胃バンディング術、胃 バイパス術など肥満手術の2型糖尿病予防効果を 非無作為化前向き対照試験で評価。15年の追跡 調査の結果、糖尿病発症率は手術群で1000人年 当たり6.8人、通常ケアを受けた対照群で28.4人 だった(調整ハザード比0.17)。 Laparoscopic Roux en Y Gastric Bypass: LRYGB Dr. Kasama 減量手術 245件 (内訳) 腹腔鏡下胃バイパス手 術 143件 腹腔鏡下袖状胃切除術 58件 ラップバンド手術 17件 腹腔鏡下BPD/DS 27件 Laparoscopic Gastric Banding Before After その他 胃内バルーン挿入術 BIB 7件 Message 1.肥満度の指標であるBMI(=体重kg÷身長mの2 乗)が32以上で、糖尿病またはそれ以外の2つ合 併症をもつ方(身長160cmで82kg以上) 2.BMIが37以上の方(身長160cmで95kg以上) ※ 上記の適応を満たす方で、内科的治療が効果がな かった方 楽をしてやせるための手術ではなく、患者様の命を守 るための手術であることを十分に理解することです ■四谷メディカルキューブ 減量外科 笠間和典先生 http://wwwmcube.jp/ 〒102-0084 東京都千代田区二番町7番7 T2DM Candidate Polymorphisms • IGF2BP2 インスリンの作用を調整していると考えられているイン スリン様成長因子2に関係する • CDKAL1 β細胞に作用するタンパク質 • CDKN2AとCDKN2B β 細胞の成長に関与するタンパク質、ガンの 成長でも研究されていた遺伝子 • TCF7L2 β細胞の機能障害 インクレチンシグナル障害 • SCL30A8 β細胞だけで発現する亜鉛輸送体遺伝子 • KCNJ11 新生児糖尿病に関与 • HHEX • PPARα 脂肪酸化障害 • PPARγ • FTO 肥満 • GCKR 中性脂肪を調節 • WFS1 インクレチンシグナル障害 • SLC30A8 • KCNQ1 • KCNJ15 • UBE2E2 • C2CD4A-C2CD4B 2010年9月9日 Nat Genet. 2010 Oct;42(10):864-8. 2010年9月9日 SNP Single Nucleotide Polymorphism Chr., chromosome RAF, risk allele frequency OR, odds ratio Nat Genet. 2010 Oct;42(10):864-8. 2010年12月16日 McCarthy MI.: Genomics, type 2 diabetes, and obesity. N Engl J Med. 2010 Dec 9;363(24):2339-50. 2010年12月16日 McCarthy MI.: Genomics, type 2 diabetes, and obesity. N Engl J Med. 2010 Dec 9;363(24):2339-50. 血糖レベルに関する形質と2型糖尿病に関連する遺伝的多様体 the DIAbetes Genetics Replication And Meta-analysis (DIAGRAM) Consortium Wellcome Trust Centre for Human Genetics, University of Oxford, Oxford, UK. Broad Institute of Harvard and Massachusetts Institute of Technology (MIT), Cambridge, Massachusetts, USA. Nat Genet. 2012 Aug 12;44(9):981-990. Wellcome Trust Centre for Human Genetics, Univ. of Oxford, Oxford, UK. Andrew P Morris, Teresa Ferreira, Anubha Mahajan, Inga Prokopenko, Ashish Kumar, Vasiliki Lagou, Cecilia M Lindgren, N William Rayner, Steven Wiltshire, Antigone S Dimas, John R B Perry, Neil Robertson, Ghazala Mirza, Joseph Trakalo, Peter J Donnelly & Mark I McCarthy Broad Institute of Harvard and Massachusetts Institute of Technology (MIT), Cambridge, Massachusetts, USA. Benjamin F Voight, Ayellet V Segrè, Elizabeth J Rossin, Soumya Raychaudhuri, Pierre Fontanillas, Noël Burtt, Jason Carey, Andrew T Crenshaw, George B Grant, Candace Guiducci, Melissa Parkin, Wendy Winckler, Sekar Kathiresan & David Altshuler Department of Pharmacology, Univ. of Pennsylvania–Perelman School of Medicine, Philadelphia, Pennsylvania, USA. Benjamin F Voight Department of Biostatistics, Univ. of Michigan, Ann Arbor, Michigan, USA. Tanya M Teslovich, Hyun Min Kang, Laura J Scott, Heather M Stringham, Anne U Jackson, Goncalo R Abecasis & Michael Boehnke Center for Human Genetic Research, Massachusetts General Hosp., Boston, Massachusetts, USA. Ayellet V Segrè, Elizabeth J Rossin, Jose C Florez, Sekar Kathiresan & David Altshuler Department of Medicine, Harvard Medical School, Boston, Massachusetts, USA. Ayellet V Segrè, Jose C Florez, James B Meigs & David Altshuler deCODE Genetics, Reykjavik, Iceland. Valgerdur Steinthorsdottir, Augustine Kong, Gudmar Thorleifsson, Unnur Thorsteinsdottir & Kari Stefansson Atherosclerosis Research Unit, Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden. Rona J Strawbridge, Karl Gertow, Bengt Sennblad, Angela Silveira & Anders Hamsten Center for Molecular Medicine, Karolinska Univ. Hosp. Solna, Stockholm, Sweden. Rona J Strawbridge, Karl Gertow, Bengt Sennblad, Angela Silveira & Anders Hamsten Department of Public Health and Primary Care, Univ. of Cambridge, Cambridge, UK. Hassan Khan, Kay-Tee Khaw, Danish Saleheen & John Danesh Research Unit of Molecular Epidemiology, Helmholtz Zentrum Muenchen, Neuherberg, Germany. Harald Grallert, Norman Klopp & Thomas Illig Oxford Centre for Diabetes, Endocrinology and Metabolism, Univ. of Oxford, Oxford, UK. Inga Prokopenko, N William Rayner, Neil Robertson, Christopher J Groves, Katharine R Owen & Mark I McCarthy Institut National de la Santé et de la Recherche Médicale (INSERM) Unité Mixte de Recherche (UMR) 1087, Nantes, France. Christian Dina Centre National de la Recherche Scientifique (CNRS) UMR 6291, Nantes, France. Christian Dina Department of Biology, Medicine and Health, Nantes Univ., Nantes, France. Christian Dina Estonian Genome Center, Univ. of Tartu, Tartu, Estonia. Tonu Esko, Krista Fischer, Kaarel Krjutškov & Andres Metspalu Institute of Molecular and Cell Biology, Univ. of Tartu, Tartu, Estonia. Tonu Esko & Andres Metspalu Centre for Population Health Sciences, Univ. of Edinburgh, Edinburgh, UK. Ross M Fraser, Harry Campbell, Jackie F Price & James F Wilson Wellcome Trust Sanger Institute, Hinxton, Cambridge, UK. Stavroula Kanoni, Sarah E Hunt, Simon Potter, Kathleen Stirrups, Sarah Edkins, Cordelia Langford, Eleftheria Zeggini, Ines Barroso, Samuli Ripatti & Panos Deloukas Medical Research Council (MRC) Epidemiology Unit, Institute of Metabolic Science, Addenbrooke's Hosp., Cambridge, UK. Claudia Langenberg, Jian'an Luan, Ruth J F Loos, Nita G Forouhi & Nicholas J Wareham Institute of Medical Informatics, Biometry and Epidemiology, Ludwig-Maximilians-Universität, Munich, Germany. Martina Müller-Nurasyid Institute of Genetic Epidemiology, Helmholtz Zentrum Muenchen, Neuherberg, Germany. Martina Müller-Nurasyid, Julia Meyer & Christian Gieger Department of Medicine I, Univ. Hosp. Grosshadern, Ludwig-Maximilians-Universität, Munich, Germany. Martina Müller-Nurasyid Institute for Medical Informatics, Biometry and Epidemiology, Univ. Hosp. of Essen, Univ. Duisburg-Essen, Essen, Germany. Sonali Pechlivanis, Karl-Heinz Jöckel & Susanne Moebus CNRS UMR 8199, Institute of Biology and Lille 2 Univ., Pasteur Institute, Lille, France. Loic Yengo, Elodie Eury, Stéphane Lobbens, Stephane Cauchi & Philippe Froguel Laboratory of Mathematics, CNRS UMR 8524, Univ. Lille 1, Model for Data Analysis and Learning (MODAL) Team, Institut National de Recherche en Informatique et en Automatique (INRIA) Lille Nord-Europe, Lille, France. Loic Yengo Diabetes Prevention Unit, National Institute for Health and Welfare, Helsinki, Finland. Leena Kinnunen & Jaakko Tuomilehto Health Science and Technology MD Program, Harvard Univ. and Massachusetts Institute of Technology, Boston, Massachusetts, USA. Elizabeth J Rossin Harvard Biological and Biomedical Sciences Program, Harvard Univ., Boston, Massachusetts, USA. Elizabeth J Rossin Division of Rheumatology, Immunology and Allergy, Brigham and Women's Hosp., Harvard Medical School, Boston, Massachusetts, USA. Soumya Raychaudhuri Partners Center for Personalized Genomic Medicine, Boston, Massachusetts, USA. Soumya Raychaudhuri National Heart, Lung, and Blood Institute's Framingham Heart Study, Framingham, Massachusetts, USA. Andrew D Johnson, Caroline Fox & Josée Dupuis Department of Genetic Medicine and Development, Univ. of Geneva Medical School, Geneva, Switzerland. Antigone S Dimas Biomedical Sciences Research Center Al Fleming, Vari, Greece. Antigone S Dimas Charles R Bronfman Institute for Personalized Medicine, Mount Sinai School of Medicine, New York, New York, USA. Ruth J F Loos Child Health and Development Institute, Mount Sinai School of Medicine, New York, New York, USA. Ruth J F Loos Department of Preventive Medicine, Mount Sinai School of Medicine, New York, New York, USA. Ruth J F Loos Program in Medical and Population Genetics, Broad Institute of Harvard and MIT, Cambridge, Massachusetts, USA. Sailaja Vedantam & Jose C Florez Division of Genetics and Endocrinology, Children's Hosp., Boston, Massachusetts, USA. Sailaja Vedantam Department of Biostatistics, Boston Univ. School of Public Health, Boston, Massachusetts, USA. Han Chen, Ching-Ti Liu & Josée Dupuis Diabetes Research Center, Diabetes Unit, Massachusetts General Hosp., Boston, Massachusetts, USA. Jose C Florez Division of Endocrinology and Metabolism, Brigham and Women's Hosp. and Harvard Medical School, Boston, Massachusetts, USA. Caroline Fox Boston Univ. Data Coordinating Center, Boston, Massachusetts, USA. Denis Rybin Collaborative Studies Coordinating Center, Department of Biostatistics, Univ. of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA. David J Couper Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, USA. Wen Hong L Kao & Man Li Department of Nutrition and Epidemiology, Harvard School of Public Health, Boston, Massachusetts, USA. Marilyn C Cornelis, Peter Kraft, Qi Sun, Rob M van Dam, David J Hunter, Lu Qi & Frank Hu Program in Molecular and Genetic Epidemiology, Harvard School of Public Health, Boston, Massachusetts, USA. Peter Kraft & David J Hunter Channing Laboratory, Department of Medicine, Brigham and Women's Hosp. and Harvard Medical School, Boston, Massachusetts, USA. Qi Sun, David J Hunter, Lu Qi & Frank Hu Saw Swee Hock School of Public Health, National Univ. of Singapore, Singapore. Rob M van Dam National Human Genome Research Institute, US National Institutes of Health, Bethesda, Maryland, USA. Peter S Chines, Lori L Bonnycastle & Francis S Collins Nord-Trondelag Health Study (HUNT) Research Centre, Department of Public Health and General Practice, Norwegian Univ. of Science and Technology, Levanger, Norway. Oddgeir L Holmen, Carl G P Platou & Kristian Hveem Centre for Genetic Epidemiology and Biostatistics, The Univ. of Western Australia, Nedlands, Western Australia, Australia. Robert Lawrence Genetics of Complex Traits, Institute of Biomedical and Clinical Science, Peninsula Medical School, Univ. of Exeter, Exeter, UK. John R B Perry, Andrew R Wood & Timothy M Frayling Department of Internal Medicine, Levanger Hosp., Nord-Trøndelag Health Trust, Levanger, Norway. Carl G P Platou Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden. Emil Rehnberg, Nancy L Pedersen & Erik Ingelsson Department of Vascular Medicine, Academic Medical Center, Univ. of Amsterdam, Amsterdam, The Netherlands. Suthesh Sivapalaratnam, Mieke D Trip & Kees Hovingh Department of Medicine, Univ. of Eastern Finland and Kuopio Univ. Hosp., Kuopio, Finland. Alena Stančáková, Markku Laakso & Johanna Kuusisto Institute for Molecular Medicine Finland (FIMM), Helsinki, Finland. Emmi Tikkanen & Samuli Ripatti Department of Chronic Disease Prevention, National Institute for Health and Welfare, Helsinki, Finland. Emmi Tikkanen, Satu Männistö, Johan G Eriksson, Samuli Ripatti & Veikko Salomaa Department of Clinical Science Malmö, Lund Univ. Diabetes Centre, Scania Univ. Hosp., Lund Univ., Malmö, Sweden. Peter Almgren, Mozhgan Dorkhan, Anna Jonsson, Jasmina Kravic, Eero Lindholm, Valeriya Lyssenko, Olle Melander, Peter M Nilsson & Leif C Groop Institute of Biomedicine, Physiology, Univ. of Eastern Finland, Kuopio, Finland. Mustafa Atalay & Timo A Lakka Faculty of Medicine, Univ. of Iceland, Reykjavík, Iceland. Rafn Benediktsson, Unnur Thorsteinsdottir & Kari Stefansson Department of Endocrinology and Metabolism, Landspitali Univ. Hosp., Reykjavík, Iceland. Rafn Benediktsson, Astradur B Hreidarsson & Gunnar Sigurðsson Endocrinology-Diabetology Unit, Corbeil-Essonnes Hosp., Corbeil-Essonnes, France. Guillaume Charpentier Diabetes Research Centre, Biomedical Research Institute, Univ. of Dundee, Ninewells Hosp., Dundee, UK. Alex S F Doney, Colin N A Palmer & Andrew D Morris Pharmacogenomics Centre, Biomedical Research Institute, Univ. of Dundee, Ninewells Hosp., Dundee, UK. Alex S F Doney, Colin N A Palmer & Andrew D Morris Icelandic Heart Association, Kopavogur, Iceland. Valur Emilsson & Gunnar Sigurðsson Department of General Practice and Primary Health Care, Univ. of Helsinki, Helsinki, Finland. Tom Forsen & Johan G Eriksson Vaasa Health Care Centre, Vaasa, Finland. Tom Forsen Division of Cardiovascular Epidemiology, Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden. Bruna Gigante, Karin Leander & Ulf de Faire Institute for Clinical Diabetology, German Diabetes Center, Leibniz Center for Diabetes Research at Heinrich Heine Univ. Düsseldorf, Düsseldorf, Germany. Christian Herder & Michael Roden Busselton Population Medical Research Institute, Sir Charles Gairdner Hosp., Nedlands, Western Australia, Australia. Jennie Hui, Alan James, Bill Musk & John Beilby PathWest Laboratory Medicine of Western Australia, Queen Elizabeth II Medical Centre, Nedlands, Western Australia, Australia. Jennie Hui & John Beilby School of Pathology and Laboratory Medicine, The Univ. of Western Australia, Nedlands, Western Australia, Australia. Jennie Hui & John Beilby School of Population Health, The Univ. of Western Australia, Nedlands, Western Australia, Australia. Jennie Hui & Bill Musk Department of Pulmonary Physiology and Sleep Medicine, West Australian Sleep Disorders Research Institute, Queen Elizabeth II Medical Centre, Nedlands, Western Australia, Australia. Alan James School of Medicine and Pharmacology, Univ. of Western Australia, Nedlands, Western Australia, Australia. Alan James & Bill Musk Institute of Biometrics and Epidemiology, German Diabetes Center, Leibniz Center for Diabetes Research at Heinrich Heine Univ. Düsseldorf, Düsseldorf, Germany. Wolfgang Rathmann Institute of Human Genetics, Univ. of Bonn, Bonn, Germany. Thomas W Mühleisen & Markus M Nöthen Department of Genomics, Life & Brain Center, Univ. of Bonn, Bonn, Germany. Thomas W Mühleisen & Markus M Nöthen Respiratory Medicine, Sir Charles Gairdner Hosp., Nedlands, Western Australia, Australia. Bill Musk Department of Cardiology, Univ. General Hosp. Attikon, Athens, Greece. Loukianos Rallidis South Karelia Central Hosp., Lappeenranta, Finland. Jouko Saramies Department of Genetics, Evolution and Environment, Univ. College London (UCL) Genetics Institute, Univ. College London, London, UK. Sonia Shah & Delilah Zabaneh Department of Clinical Chemistry and Central Laboratory, Univ. of Ulm, Ulm, Germany. Gerald Steinbach & Roman Wennauer Institute of Epidemiology II, Helmholtz Zentrum Muenchen, Neuherberg, Germany. Barbara Thorand & Annette Peters Centro Cardiologico Monzino, IRCCS, Milan, Italy. Fabrizio Veglia, Damiano Baldassarre & Elena Tremoli MRC Institute of Genetics and Molecular Medicine at the Univ. of Edinburgh, Western General Hosp., Edinburgh, UK. Harry Campbell & James F Wilson Department of Epidemiology, Erasmus Univ. Medical Center, Rotterdam, The Netherlands. Cornelia van Duijn, Andre G Uitterlinden & Albert Hofman Netherland Genomics Initiative, Netherlands Consortium for Healthy Ageing and Centre for Medical Systems Biology, Rotterdam, The Netherlands. Cornelia van Duijn & Andre G Uitterlinden Department of Internal Medicine, Erasmus Univ. Medical Center, Rotterdam, The Netherlands. Andre G Uitterlinden & Eric Sijbrands Oxford National Institute for Health Research Biomedical Research Centre, Churchill Hosp., Oxford, UK. Katharine R Owen & Mark I McCarthy Molecular Medicine, Department of Medical Sciences, Uppsala Univ., Uppsala, Sweden. Ann-Christine Syvänen Unit of General Practice, Helsinki Univ. General Hosp., Helsinki, Finland. Johan G Eriksson Folkhälsan Research Center, Helsinki, Finland. Johan G Eriksson, Tiinamaija Tuomi & Bo Isomaa INSERM CESP U1018, Villejuif, France. Beverley Balkau Univ. Paris Sud 11, UMRS 1018, Villejuif, France. Beverley Balkau Department of Medicine, Helsinki Univ. Hosp., Univ. of Helsinki, Helsinki, Finland. Tiinamaija Tuomi Department of Social Services and Health Care, Jakobstad, Finland. Bo Isomaa Division of Endocrinology, Diabetes and Nutrition, Univ. of Maryland School of Medicine, Baltimore, Maryland, USA. Alan R Shuldiner Geriatric Research Education and Clinical Center, Baltimore Veterans Administration Medical Center, Baltimore, Maryland, USA. Alan R Shuldiner Program in Personalized and Genomic Medicine, Univ. of Maryland School of Medicine, Baltimore, Maryland, USA. Alan R Shuldiner Department of Medicine/Metabolic Diseases, Heinrich Heine Univ. Düsseldorf, Düsseldorf, Germany. Michael Roden Univ. of Cambridge Metabolic Research Laboratories, Institute of Metabolic Science, Addenbrooke's Hosp., Cambridge, UK. Ines Barroso National Institute for Health Research (NIHR) Cambridge Biomedical Research Centre, Institute of Metabolic Science, Addenbrooke's Hosp., Cambridge, UK. Ines Barroso Department of Community Medicine, Faculty of Health Sciences, Univ. of Tromsø, Tromsø, Norway. Tom Wilsgaard & Inger Njølstad Kuopio Research Institute of Exercise Medicine, Kuopio, Finland. Rainer Rauramaa & Timo A Lakka Department of Clinical Physiology and Nuclear Medicine, Kuopio Univ. Hosp., Kuopio, Finland. Rainer Rauramaa Department of Medical Sciences, Uppsala Univ., Akademiska Sjukhuset, Uppsala, Sweden. Lars Lind Department of Dietetics-Nutrition, Harokopio Univ., Athens, Greece. George Dedoussis Faculty of Medicine, Institute of Health Sciences, Univ. of Oulu, Oulu, Finland. Sirkka M Keinanen-Kiukaanniemi Unit of General Practice, Oulu Univ. Hosp., Oulu, Finland. Sirkka M Keinanen-Kiukaanniemi Finnish Diabetes Association, Tampere, Finland. Timo E Saaristo Pirkanmaa Hosp. District, Tampere, Finland. Timo E Saaristo Department of Internal Medicine, South Ostrobothnia Central Hosp., Seinäjoki, Finland. Eeva Korpi-Hyövälti & Jaakko Tuomilehto Department of Medicine, Central Finland Central Hosp., Jyväskylä, Finland. Juha Saltevo Department of Genetics, Univ. of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA. Karen L Mohlke Diabetes and Obesity Research Institute, Cedars-Sinai Medical Center, Los Angeles, California, USA. Richard N Bergman Red RECAVA Grupo RD06/0014/0015, Hosp. Universitario La Paz, Madrid, Spain. Jaakko Tuomilehto Centre for Vascular Prevention, Danube-Univ. Krems, Krems, Austria. Jaakko Tuomilehto Division of Endocrinology and Diabetes, Department of Internal Medicine, Univ. Medical Centre Ulm, Ulm, Germany. Bernhard O Boehm Genomic Medicine, Imperial College London, Hammersmith Hosp., London, UK. Philippe Froguel Department of Pharmacological Sciences, Univ. of Milan, Milan, Italy. Damiano Baldassarre & Elena Tremoli Institute of Cardiovascular Science, Univ. College London, London, UK. Steve E Humphries Center for Non-Communicable Diseases Pakistan, Karachi, Pakistan. Danish Saleheen Clinic of Cardiology, West German Heart Centre, Univ. Hosp. of Essen, Univ. Duisburg-Essen, Essen, Germany. Raimund Erbel Hannover Unified Biobank, Hannover Medical School, Hannover, Germany. Thomas Illig Department of Statistics, Univ. of Oxford, Oxford, UK. Peter J Donnelly Diabetes Genetics, Institute of Biomedical and Clinical Science, Peninsula Medical School, Univ. of Exeter, Exeter, UK. Andrew T Hattersley Human Genetics Center, Univ. of Texas Health Science Center at Houston, Houston, Texas, USA. Eric Boerwinkle Human Genome Sequencing Center at Baylor College of Medicine, Houston, Texas, USA. Eric Boerwinkle Cardiovascular Research Center, Massachusetts General Hosp., Boston, Massachusetts, USA. Sekar Kathiresan Division of Epidemiology and Community Health, Univ. of Minnesota, Minneapolis, Minnesota, USA. James S Pankow General Medicine Division, Massachusetts General Hosp., Boston, Massachusetts, USA. James B Meigs Department of Genetics, Harvard Medical School, Boston, Massachusetts, USA. David Altshuler Department of Molecular Biology, Harvard Medical School, Boston, Massachusetts, USA. David Altshuler Diabetes Unit, Massachusetts General Hosp., Boston, Massachusetts, USA. David Altshuler AIM To extend understanding of the genetic architecture and molecular basis of type 2 diabetes (T2D) Methods we conducted a meta-analysis of genetic variants on the Metabochip, including 34,840 cases and 114,981 controls, overwhelmingly of European descent. This custom array of 196,725 variants was designed to facilitate cost-effective follow-up of nominal associations for T2D and other metabolic and cardiovascular traits and to enhance fine mapping of established loci. The T2D component of Metabochip comprises 21,774 variants, including 5,057 ‘replication’ SNPs that capture the strongest independent (r2 < 0.2 in 1000 Genomes Project Utah residents of Northern and Western European ancestry (CEU) data) autosomal association signals from the GWAS meta-analysis conducted by the DIAbetes Genetics Replication and Meta-analysis (DIAGRAM) Consortium. This genome-wide meta-analysis (DIAGRAMv3) includes data from 12,171 T2D cases and 56,862 controls of European descent imputed at up to 2.5 million autosomal SNPs and augments the previously published DIAGRAMv2 meta-analysis4 with 4 additional GWAS (Supplementary Table 1). The T2D content of Metabochip includes an additional 16,717 variants, most chosen from 1000 Genomes Project pilot data, to fine map 27 established susceptibility loci. HNF1B FTO MAEA AP3S2 SLC30A8 ANKRD55 (TCF2) HNF4A KLHDC5 BCL11A SPRY2 HNF1A GLIS3 IGF2BP2 SRR JAZF1 ZBED3 (TCF1) HMG20A WFS1 TCF7L2 BCAR1 HMGA2 RBMS1 TLE1 GIPR CDC123/C ADAMTS9 VPS26A ST64GAL1 KCNQ1 C2CD4A AMK1D DGKB PPARG CDKAL1 THADA PTPRD IRS1 ZMIZ1 GRB14 HHEX/IDE CDKN2A/B PSMD6 KCNK16 TSPAN8/L GCK ZFAND6 PROX1 PRC1 CCND2 GR5 PEPD TLE4 MC4R MTNR1B ANK1 ZFAND3 DUSP8 KLF14 CILP2 KCNJ11 NOTCH2 ARAP1 GCKR UBE2E2 GCC1 ADCY5 (CENTD2) TP53INP1 Figure 2 Regional plots of T2D susceptibility loci with evidence of multiple association signals. Each circle represents a Metabochip SNP passing quality control in our combined meta-analysis plotted with its association P value (on a −log10 scale) as a function of genomic position (NCBI Build 36). For each locus, the lead SNP is represented by a purple diamond. The color of all other SNPs indicates LD with the lead SNP (estimated by CEU r2 from 1000 Genomes Project data, June 2010 release). Recombination rates are estimated from International HapMap Project data, and gene annotations are taken from the UCSC Genome Browser. Supplementary Figure 9. Plot of FG and T2D risk at novel and established T2D susceptibility loci obtained from the present meta-analysis and up to 133,010 nondiabetic individuals from the MAGIC Investigators. Each point represents a lead T2D SNP, aligned to the risk allele, coloured according to the significance of association with FG: red p<5x10-8; orange 5x10-8≤p<10-4; yellow 10-4≤p<0.01; green 0.01≤p<0.05; blue p≥0.05. Biological hypotheses related to disease pathogenesis tested with GSEA (gene-set enrichment analysis) Adipocytokine signalling. Adipocytokines have been implicated in the development of insulin resistance. Leptin and adiponectin are potential insulin sensitizers and TNF-alpha is a potential insulin antagonist19. Amyloid metabolism. The islet amyloid polypeptide inhibits insulin and glucagon secretion from pancreatic betaislet cells. Islet amyloid deposits have been associated with T2D and pancreatic beta-cell loss20,21. Branched-chain amino acid metabolism. Elevated branched-chain amino acid plasma levels are associated with high insulin resistance and/or low circulating levels of insulin in T2D cases. The branched-chain amino acids, isoleucine, leucine and valine, are strong predictors of future diabetes. Leucine acutely stimulates insulin secretion in pancreatic beta cells22-24. Cell cycle. Several cell cycle regulators lie in previously established T2D loci, including CDKN2B/A, CDKN1C, and CCNE2. The majority of these genes regulate CDK4 or CDK6, shown to play a role in beta-islet pancreatic cell proliferation, which in turn may affect insulin secretion. These regulators may also have an effect on peripheral tissues relevant to T2D25-27. Circadian rhythm. Several studies showed that people with an altered circadian rhythm have an increased risk of developing T2D. MTNR1B regulates circardian rhythm and contains common variants associated with T2D, fasting glucose, and pancreatic beta-cell function, suggesting a causal role for circadian rhythm in T2D. The melatonin system was shown to regulate glucose homeostasis28-32. Endoplasmic reticulum (ER) stress response (unfolded protein response). WFS1, a component of the unfolded protein response, lies near common variants associated with T2D and harbours rare mutations associated with Wolfram syndrome, a rare syndrome that causes diabetes mellitus, amongst other disorders. WFS1 is up-regulated during insulin secretion. Inactivation of WFS1 in beta-cells causes ER stress and dysfunction. Furthermore, EIF2AK3, a key component of the ER stress response pathway, contains rare mutations that cause neonatal diabetes33-35. Fatty acid metabolism. Elevated plasma free fatty acid (FFA) concentrations are linked with the onset of skeletal muscle and hepatic insulin resistance and are associated with T2D. Elevated blood fatty-acid concentrations reduce muscle glucose uptake, and increase liver glucose production, contributing to elevated blood glucose levels. FFA also affects insulin secretion from the pancreas. However, in pre-diabetic patients, FFA stimulation of insulin secretion is not sufficient to fully compensate for the FFA-induced insulin resistance, leading to hyperglycaemia36,37. Glycolysis and gluconeogenesis. Glucokinase, GCK, the first glycolytic enzyme, and GCKR, a regulator of GCK, contain or lie near common SNPs associated with T2D. Studies have shown that hepatic gluconeogenesis is increased in people with T2D compared with controls following overnight fasting38,39. Inflammation. Elevated levels of the inflammatory cytokines, TNF-alpha and IL-6, and the Creactive protein that rises in response to inflammation, predict the development of T2D. However, whether inflammation is a primary cause of T2D or secondary to hyperglycaemia (or other T2D features) is not yet clear. A potential mechanism of causality is through macrophages that release cytokines, causing neighbouring liver, muscle or fat cells to become insulin resistant. Inflammation in pancreatic islets could also lead to a decrease in beta-cell mass affecting insulin secretion levels40-43. Insulin signalling. Alterations in insulin signalling may lead to insulin resistance in peripheral tissues such as fat, liver and muscle, a major risk factor for T2D27,44. Insulin synthesis and secretion. Insufficient insulin secretion is one of the major causes of T2D. Many of the established T2D common SNP associations lie near genes implicated in beta-cell function, such as KCNJ11 and ABCC8. These ATP sensitive potassium channel subunits, proximal to each other on the chromosome, are targets of anti-diabetes drugs (sulfonylurea and/or meglitinides) that lead to an increase in insulin secretion. Mutations in these genes are also associated with different forms of neonatal diabetes27,44. Mitochondrial dysfunction. Mitochondrial dysfunction has been implicated in both rare and common forms of diabetes. T2D cases have less mitochondria in their skeletal muscle, and oxidative phosphorylation genes are collectively down-regulated in muscle, compared with healthy individuals. However, pronounced genetic evidence for a causal effect of decreased mitochondrial activity on T2D has not yet been shown45-47. NOTCH signalling. NOTCH2 contains a common variant associated with T2D. NOTCH signalling plays a role in pancreas development35,48. PPARG signalling. PPARG contains a common variant associated with T2D, and is the target of thiazolidinedione (TZD) drugs, used clinically to reduce insulin resistance in T2D patients. PPARG plays a role in fat, liver and muscle49,50. Vitamin D metabolism. Vitamin D deficiency has been suggested to be associated with T2D and insulin resistance. Vitamin D may also play a role in insulin secretion by promoting calcium absorption in the pancreas5153. WNT signalling. A strong common variant association signal lies in an intron of TCF7L2, a transcription factor that regulates WNT targets. The WNT signalling pathway may play a role in both the insulin secretion and insulin sensitivity features of T2D. For example, WNT signalling activation in the pancreas leads to pancreatic beta cell proliferation, and improved insulin sensitivity in skeletal muscle54-57. a nuclear protein that binds to cAMP-response elementbinding protein (CREB), We saw no evidence of enrichment for other processes implicated in T2D pathogenesis, including amyloid formation, endoplasmic reticulum stress and insulin signaling. Figure 3 Functional analyses. (a,b) PPI subnetwork for CREBBP (a) and adipocytokine (b) interactions. All direct interactions and common interactors between direct connections were extracted from the larger network of 314 proteins defined in DAPPLE network analysis. Genes in the network are represented as circles (nodes), colored according to the statistical relationship with T2D: gray, common interactors between GWASidentified or monogenic loci; blue, monogenic loci only; red, GWAS-identified loci only; green, loci with GWAS association and implicated by monogenic forms of diabetes. Each interaction defined in the in WEB network is depicted by a line (edge) between nodes. (c) GRAIL circle plot of locus connectivity. Each locus is plotted in a circle, where significant connections (P < 0.05) based on PubMed abstracts are drawn spanning the circle. Conservatively, we treated all monogenic loci (region 142) as a single locus by which connectivity was assessed. The strongest connections (P < 0.001) are colored in bright red. (d) GSEA of associations in the adipocytokine signaling pathway. Black bars represent the stage 1 meta-analysis P values of 63 autosomal genes in the adipocytokine signaling pathways (KEGG). Top, density plot of the black bars (red line). The replicating genes in the leading edge of the GSEA are listed. Stage 2 modified GSEA P = 1.6 × 10−4 was calculated on the basis of both the primary and secondary transcripts using the LD locus definition. Supplementary Figure 11. Plot of T2D and T1D risk at 37 established T1D susceptibility loci obtained from the present meta-analysis and up to 7,514 T1D cases and 9,045 population controls from the Type 1 Diabetes Genetics Consortium. Each point represents a lead T1D SNP, aligned to the risk allele, coloured according to the significance of association with T2D: red p<0.05; blue p≥0.05. Findings We identified ten previously unreported T2D susceptibility loci, including two showing sexdifferentiated association. Genome-wide analyses of these data are consistent with a long tail of additional common variant loci explaining much of the variation in susceptibility to T2D. Exploration of the enlarged set of susceptibility loci implicates several processes, including CREBBP-related transcription, adipocytokine signaling and cell cycle regulation, in diabetes pathogenesis. Message オックスフォード大学、米ハーバード・マサチューセッツ工科大 学(MIT)ブロード研究所および米ミシガン大学の研究者らによ る今回の研究では、2型糖尿病に関連する可能性のあるDNAに共通 する遺伝的多様性(バリエーション)について検討。2型糖尿病 患者約3万5,000人と、同疾患のない約11万5,000人のDNAを調べ、 DNAの変化と糖尿病リスクとの関連のみられる新たな遺伝子領域 を突き止めた。このうち2つは性別によって異なる作用がみられ、 1つは男性の疾患リスク増大に関連しており、もう1つは女性のリ スク増大に関連していた。 この研究から、2型糖尿病に関連する遺伝子タイプのパターン も浮上した。「60強の遺伝子全体を併せ見ることにより、疾患リ スクに影響を及ぼす遺伝子の種類の特徴を探ることができる」と、 McCarthy氏は述べている。細胞の成長、分裂および老化のプロセ スに関与する遺伝子、脂肪細胞が他の身体部位での生物学的プロ セスに影響を及ぼす経路に関与する遺伝子、他の遺伝子を制御す る転写因子遺伝子などが認められているという。