Untangling the Controversy:
Emergency Contraception for
Adolescents
Erica Monasterio, MN, FNP
Division of Adolescent Medicine
University of California, San
Francisco
Emergency Contraception
• Definition: a device or drug used as an
emergency procedure to prevent
pregnancy following unprotected or
under-protected intercourse.
Methods Currently Available in
the U.S.
• Combined Oral Contraceptives
• Copper Intrauterine Devices
• Progestin-only Prepackaged ECPs
(Plan B)
Copper Containing IUD Insertion
Appropriate for low risk young
women who have had a child and
want to use an IUD as their method
of contraception
Yuzpe Regimen: OC
g EE/ mg levonorgestrel/
Formulations
Dose
Dose
Brand Name
Pills/Dose
Ovral
Alesse
Levlite
Nordette
Levlen
Levora
Lo/Ovral
Triphasil
Tri-Levlen
Trivora
2 white
5 pink
5 pink
4 light orange
4 light orange
4 white
4 white
4 yellow
4 yellow
4 pink
100
100
100
120
120
120
120
120
120
120
0.50
0.50
0.50
0.60
0.60
0.60
0.60
0.50
0.50
0.50
Adapted from ACOG Practice Bulletin. Int J Gynecol Obstet. 2002;78:191-198.
Slide Source:ContraceptionOnline www.contraceptiononline.org
“Plan B”
• Brand name for
progestin only
emergency
contraceptive pills
• Recently approved for
over-the-counter
purchase by women
>18 years old
Trends in Sexual Activity
YRBS 2003
Significant Decline in 15-17 year
olds
NSFG 2002
More than half of youth <18 are sexually
experienced
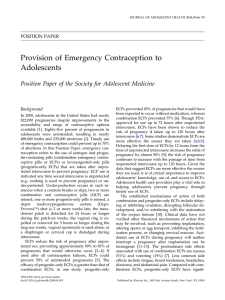
Cumulative % of teens who have had sex before reaching selected ages
%
100
80
43
39
40
20
58
54
60
27
25
8
15
6
13
0
Male
Female
<14
<15
<16
<17
<18
Abma JC et al., Teenagers in the United States: sexual activity, contraceptive use, and childbearing, 2002, Vital and Health
Statistics, 2004, 23(24).
33.2
28.5
26.7
30
35
30.9
25
26.0
20
25.1
WOMEN
15
17.4
10
12.6
AGE
14.0
MEN
16.9
Young people are at high risk of unintended
pregnancy for many years
The Alan Guttmacher Institute (AGI), In Their Own Right: Addressing the Sexual and Reproductive Health Needs of American Men,
New York: AGI, 2002, p. 8.
Many teens use contraceptives
• The majority of teens (74% of females and 82% of
males) used contraceptives the first time they had sex
• The majority of teens (83% of females and 91% of
males) used contraceptives the last time they had sex
• A sexually active teen who does not use contraceptives
has a 90% chance of becoming pregnant within a year
Abma JC et al., Teenagers in the United States: sexual activity, contraceptive use, and childbearing, 2002, Vital and Health Statistics, 2004,
23(24).
Many young teens become pregnant
each year
• 280,000 teens younger than 18 become pregnant
annually
• 87% of these pregnancies are unintended
• Of pregnancies to 15–17-year-olds:
– 56% result in live births
– 30% result in abortions
– 14% end in miscarriage
Guttmacher Institute, U.S. teenage pregnancy statistics: national and state trends and trends by race and ethnicity, New York: Guttmacher
Institute, September 2006, <http://www.guttmacher.org/pubs/2006/09/12/USTPstats.pdf >, accessed October 9, 2006; and Finer LB et al.,
Disparities in unintended pregnancy in the United States, 1994 and 2001, Perspectives on Sexual and Reproductive Health, 2006,
38(2):90–96.
ECPs: Mechanism of Action
• ECPs act by preventing pregnancy and never by
disrupting an implanted pregnancy, i.e. never as an
abortifacient
• If taken before ovulation, ECPs disrupt normal
follicular development and maturation, blocks LH
surge, and inhibit ovulation; they may also create
deficient luteal phase
• may have a contraceptive effect by thickening
cervical mucus (theoretical: no clinical data)
ECPs: Mechanism of Action
• If taken after ovulation, ECPs have little effect on
ovarian hormonal production and limited effect on
endometrial maturation
• ECPs may affect tubal transport of sperm or ova
Indications
• After unprotected intercourse
• After under-protected intercourse
–
–
–
–
–
–
–
After barrier method “accidents”
After missed OCPs (>2)
After missed progestin-only pills (1)
>14 weeks since last Depo-Provera shot
Transdermal patch detached >24 hrs.
Vaginal ring expelled/removed >3 hours
Vaginal spermacide used alone
Contraindications to ProgestinOnly ECP
• Pregnancy
• Hypersensitivity to any component
• Undiagnosed abnormal vaginal bleeding
Instruction for Use
• As soon as possible after unprotected or underprotected intercourse
• Effective up to 5 days (120 hours) after event
• Can take both pills at once (package instructions
are 1 pill followed by 2nd pill 12 hours later)
• Next menses may be earlier, later, and/or heavier
• Return for pregnancy test if no menses in 3 weeks
• Discuss STI screening and effective contraceptive
plan as appropriate
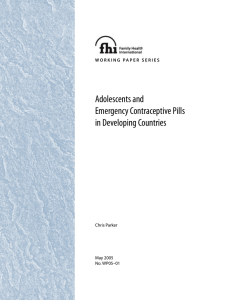
Levonorgestrel and Yuzpe Regimens:
Delay of Treatment and Pregnancy Rates
5.00%
4.00%
3.00%
2.00%
1.00%
0.00%
Daily (hours)
Women (N)
0-12
386
13-24 25-36 37-48 49-60 61-72
522
326
379
191
Piaggio G, et al. Lancet. 1999;353:721. Used with permission.
Slide Source: ContraceptionOnline www.contraceptiononline.org
146
Side Effects
• Nausea and vomiting (less with Plan B)
• Breast tenderness
• Menstrual disturbance in next menses
(early, late, heavier)
• Headache, mood changes, fatigue
EC and Sexual Risk Behaviors
• EC use is not associated with increased risk
taking behaviors among adolescent women.
• Expanding access to emergency
contraception impacts women's ability to
use the product – period.
Gold, MA, Wolford JE, Smith KA, Parker Am. The effects of advance provision of
emergency contraception on adolescent women’s sexual and contraceptive behaviors.
Journal of Pediatric and Adolescent Gynecology. 2004 Apr; 17(2): 87-96.
Answering the Concerns: Will
access increase risky behaviors?
Studies show that increased access to emergency
contraception among adolescents
• does NOT result in inappropriate use of Plan B as
a routine form of contraception
• does NOT result in an increase in number of
sexual partners,
• does NOT result in an increase in frequency of
unprotected intercourse
• does NOT result in an increase in the frequency of
sexually transmitted diseases
Raine T. et al, Increased Access to Emergency Contraception and Impact on Pregnancy and STIs: A
Randomized Controlled Trial, Journal of the American Medical Association, 2005; 293:54-62.
Answering the Concerns: Will
access to EC interrupt regular care?
• Young women who have easier access to EC are
also no more likely to use EC repeatedly, than
women who obtain it from a clinic or healthcare
provider
• Furthermore, research show that a request for
emergency contraception may actually lead to
initiation of routine gynecologic care, including
counseling about sexual behaviors and prevention
strategies
Stewart, HE, Gold MA, Parker AM. The Impact of Using Emergency Contraception on
Reproductive Health Outcomes: A Retrospective Review in an Urban Adolescent
Clinic. Journal of Pediatric Adolescent Gynecology (2003) 16:313–318.
Answering the Concerns: Is it a
contradictory message?
• 68% of adults and 77% of teens think making
emergency contraception more widely and
easily available is consistent with a strong
message to teens that abstinence from sex is
their best option by far
National Campaign to Prevent Teen Pregnancy Website. http://www.teenpregnancy.org.
• Removing the barriers to access ensures that
teens who have sex when they do not want or
do not plan to – as well as those who
experience a contraceptive accident – are able
to avoid unintended pregnancy
Access to EC
• Individual providers have an essential role:
– Counsel all youth, regardless of current sexual
activity or current method of contraception
– Assess for current risk
– Provide on-site access when possible
– Offer prescription along with a list of local
pharmacies where EC can be obtained
Access to EC
• Clinics play a significant role
– 2.2 million sexually active minors need
publicly supported contraceptive services and
supplies*
– Each year publicly funded family planning
clinics provide services to roughly 900,000
minors
– Therefore, clinics serve about 40% of minors in
need of publicly supported contraceptive
services
Guttmacher Institute, Women in Need of Contraceptive Services and Supplies, 2004, New York: Guttmacher Institute, 2006
Advocacy Has an Impact
QuickTime™ and a
TIFF (Uncompressed) decompressor
are needed to see this picture.
Access Issues to Consider
•
•
•
•
•
•
•
State funding of EC
Coverage by plans
Pharmacy Access
Pharmacy/pharmacist refusal to supply
Unrestricted OTC status
Protecting minor consent/confidentiality
Educating and Engaging Parents