Health Inequality & Welfare Capitalism
advertisement

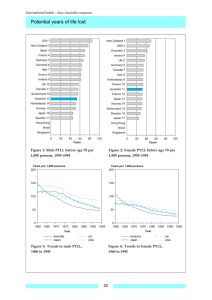
Health Inequality & Welfare Capitalism Nicky Hart Professor of Sociology University of California Los Angeles Reducing Health Inequalities What do we really know about Successful Strategies? 8-9th May 2009 • What is the most effective mode of social organization for promoting population health and, by implication, reducing health inequalities? • Can variations in the epidemiological history of welfare state regimes (WSR) answer this question? • Cautionary note: Assuming there is an affirmative answer to this question, we must not assume it would be easy to transfer successful policy interventions from one socio-historical context to another. Policy implies purposeful public intervention designed to achieve defined goals; WSR implies a whole repertoire of interlinked social institutions which have evolved over decades, even centuries, shaped in the course of their development by democratic class struggle punctuated by major historical events – world wars, economic crises, cultural antecedents and upheavals – a successful policy in one WSR may not be portable to another whose ethos is entirely different. Policy depends on the political will, and, to paraphrase one famous German social theorist: men make their own policy but they do not do it under conditions of their own choosing. Why we should expect the Welfare State Regime concept to offer the best approach to uncovering the secret of a healthy society? • WSRs are alternative modes of societal modernization developed to insulate population livelihood from the risks of market capitalism. • He introduced the concept of decommodification to capture variations in the capacity of WSRs to perform this function. It involves the removal of commodity status from essential human needs, on the grounds that these goods and services should be be subject to market exchange and profit. • From all that we know of the relationship between material inequalities and health over the life course, it makes sense to predict that decommodification will be an important variable differentiating health outcomes between welfare states. • However, as his feminist critics were quick to point out, commodification is not necessarily bad, it can entail liberation from dependency relations, and as far as women are concerned, the commodification of their labor is toi be welcomed not resisted. Defamilization and the Fourth Regime. • In face of feminist challenge, Esping Anderson added an additional concept and a fourth regime type to his typology. Defamilization measures a WSR’s capacity to liberate individuals from dependency on the most traditional of all welfare institutions – the family. In the same context, he also added a fourth ideal type to his model – the familist welfare regime associated with the Mediterranean region and to some extent Japan. • Applying both concepts, decommodification and defamilization, his original conclusion was unchanged, , the social democratic regime still emerges as the most successful mode of organizing social life to protect human wellbeing with the added benefit of strengthening the immemorial/ultimate purpose of social organization, the maintenance of the flow of population through the social fabric. • The defamilization concept is an interesting tool from the perspective of social epidemiology because the social support typically associated with family life is known to exert a powerful influence on survival. The health output of the Five regimes • Measuring health : The risks of premature death – YPLL 1- 75 years. • Nations included in the study • Britannia ( Old World Liberal) England & Wales, Scotland & Northern Ireland • New World Liberal : USA • Corporate: Austria, Belgium, France and Netherlands • Social Democratic: Denmark, Norway, Sweden • Mediterranean: Greece, Italy, Spain • Time period 1960 – 2000 • Two Types of Gender Inequality Female Trends in premature death in Welfare State Regimes So c D em 80 M e dit B rit a nnia C o rpo ra t e Pyll per 1000 population all causes E uro pe US A 70 60 50 40 30 1960 1970 1980 year 1990 2000 Trends in Premature Male Death : All Causes 1963-93 135.00 pyll per 1000 male pop 125.00 115.00 105.00 95.00 85.00 75.00 65.00 1963 Europe Britannia 1973 1983 Corporate Soc Dem 1993 2000 M editerranean US Liberal Types of Mortality in Welfare State Regimes • Early versus Late Premature Death : Potential years of life lost before and after Age 55. • External versus Universal Causes: The relative significance of accidents, suicide and violence versus aging . Contribution of early premature death (> 54 years) 2000 70.00 Males Females 65.00 60.00 55.00 50.00 45.00 europe Britannia Corporate Medit Soc Dem USA Type I male mortality 1963-93 45.00 40.00 pyll per 1000 male pop 35.00 30.00 25.00 20.00 15 . 0 0 10 . 0 0 19 6 3 19 7 3 19 8 3 19 9 3 2000 Europe Corporate Mediterranean Britannia Soc Dem US Liberal Trends in Type I premature death in Welfare State Regimes Females 1960-2000 15 So c D em M e dit Pyll per 1000 population all causes 13 B rit a nnia C o rpo ra t e E uro pe 11 US A 9 7 5 3 1960 1970 1980 year 1990 2000 Type II male mortality 1963-93 110 .0 0 10 0 .0 0 pyll per 1000 male pop 9 0 .0 0 8 0 .0 0 70 .0 0 6 0 .0 0 50 .0 0 19 6 3 19 73 19 8 3 19 9 3 2000 E uro pe C o rpo ra t e M e dit e rra ne a n B rit a nnia So c D em US Libe ra l Trends in Type II premature death in Welfare State Regimes Females 1960-2000 75 70 Pyll per 1000 population all causes So c D em M e dit 65 B rit a nnia 60 C o rpo ra t e E uro pe 55 US A 50 45 40 35 30 25 1960 1970 1980 year 1990 2000 Substantive Findings • The risks of premature death declined substantially in all WSRs 1960-2000 • The Social Democratic regime charted the shallowest decline, but this regime had a massive head start in 1960 • Gender is a major factor of differentiation: One man’s healthy society is not necessarily one woman’s healthy society. To illustrate, contrast the male and female trend of Britannia. • Among males, the social democratic charts the most progressive course; but Britannia also charts a progressive trajectory. . • For females, the familist Mediterranean regime is the surprising success story, charting low rates of type I mortality and the most progressive decline of type II. The familist regime does not enjoy a reputation as a female friendly society yet it emerges as the most propitious epidemiological environment for women . Social Democracy & Deviant Denmark Denmark makes a significant negative contribution to the sluggish performance of social democracy in the 2nd half of the 20th century In 1960, Denmark recorded rates of premature death below the European average but above the social democratic norm, the gap between Denmark and the other representatives of this regime type widened each decade , by 2000, Denmark displayed the highest relative risk of any nation. Circulatory 1993 - Denmark and other Nordic Cirrhosis 1993 - Denmark and other Nordic 50.00 Rate of PYLL 25.00 2.50 0.00 0.00 1-4 15-24 5-14 15-24 25-34 35-44 45-54 55-64 65-74 DenmarkAge Group other Nordic 25-34 35-44 Denmark Lung Cancer 1993 - Denmark and other Nordic 45-54 55-64 65-74 Age Group Other Nordic Breast Cancer 1993 - Denmark and other Nordic Rate of PYLL 25.00 Rate of PYLL Rate of PYLL 5.00 0.00 0.00 15-24 25-34 Denmark 35-44 45-54 55-64 65-74 25-34 35-44 Age Group Other Nordic Denmark 45-54 55-64 Age Group Other Nordic 65-74 The disciplining dimension of welfare capitalism • This example also underlines an important but neglected ingredient of WSRs, the fact that they exert an important disciplining function, and, perhaps, the greater the redistribution, the greater need for social discipline if the ideological integrity of the system is to be maintained. • Note also, the necessity and the utility of taking a long run view to understand the importance of the various factors impinging on population health status in different places. • From the trend in the social democratic regime, we can see that this regime had already made remarkable headway improving population health status before the Golden Age of the Welfare State. Ironically, the decline of mortality slowed down in this period when the policies which today characterize this mode of social organization were being established. As we have seen , Denmark goes some way to explain this unexpected finding, and exploring the reason reminds us the importance of long standing cultural influences directly impacting upon health while also furnishing an hospitable normative environment for institutional reform and development. In northern Europe, especially, temperance was an important element in the modernising project and one of the cornerstones of social democracy Explaining Danish Deviance • From all that we know of the class gradients in health, there are no grounds for doubting the benefits of the redistributive policies of the type pioneered by Social Democracy • At the same time, the WSR is not the only factor, other structural influences are at work shaping population health status and we must be aware of them in assessing the health generating capacity of a WSR. • How does Denmark differ form her neighbors? The proximate factor in Denmark’s relative disadvantage is cigarette smoking, why did Danish women turn to the cigarette with greater intensity than the women of Sweden or Norway. Possible factors include urbanization, male smoking culture, but I suspect the most significant is the legacy of Temperance. • Of the 3 social democratic nations, Denmark was alone in not embracing temperance with attendant legislation to civilize drinking behavior as the society modernized. Sweden by contrast, introduced the most rigorous controls to discipline the population in this respect. The absence of a temperance legacy may explain the resistance of Danes to anti-smoking propaganda and the toll of mortality that followed. • This reminds us that that we should not overlook the important civilizing mission of the ‘policy makers’ who made social democracy. Temperance was a strong element in the social ideology of Nordic social democracy, I believe it is an important component of the early epidemiological advantage of Scandinavia. Final Point: The Importance of Cigarette Smoking for Health Inequality • Cigarettes is a versatile accessory to modern life, in its time it has served as a style icon, a badge of adulthood, a symbol of liberation a source of pleasure not to mention, a handy self administered device for managing stress. For sociologists, it has even been put forward as a proxy for social class. • It is a very important factor in the widening health inequalities, it explains the bulk of the widening gradient in health inequality within and between nations. Ironically this is a public health triumph with a downside for health inequality. • Smoking explains the contrary experience of male and female trends in Britannia and for the relative disadvantage of Denmark. • It is also a factor, by its relative absence, in the advantageous Mediterranean female trend. • Cigarette smoking signifies the claim of autonomy even in contexts of extreme constraint, it reveals that part of the cause of health inequality is the extension of the freedom to choose.