Thrombotic Microangiopathy in the Transplant
Kidney
Dr Weng Oh
ST7 in renal medicine
Background
•
•
•
•
•
33 year old Caucasian female
Kidney transplant from brother 2011
Primary renal disease: chronic pyelonephritis
Crohns disease
Tacrolimus 5mg bd, Azathioprine 100mg od, Prednisolone
5mg od
• Baseline creatinine: 130 – recent rise to 160 umol/L
• Urine PCR 49mg/mmol
• Awaiting transplant biopsy
Admitted 7.8.15
• 2 week history of RUQ pain
• Vomiting 8-9x in last 48 hours
• ‘Not passing as much urine as she ‘s used to’
• No recent flare-ups
• AKI with Creat 330umol/L
• Denies taking any nephrotoxic agents
8.8.15
• Seen by renal on-call team
• Creat risen further to 471
• ABG – no acidosis/hyperkalaemia
• LFTs and amylase normal
• Hypovolaemic
• Urinalysis – 4+blood, 3+ protein
• USS – normal transplant kidney, no hydronephrosis
• No evidence of sepsis
Changes in lab parameters
9.8.15
•
•
•
•
•
•
•
•
LDH 1644
Platelet 90 – falling
Hb 90
Blood film – red cell fragments
Plasma exchange started
RIJ vascath inserted
Methylpred 500mg IV od for 3 days
Tacrolimus stopped
• Azathioprine switched to MMF
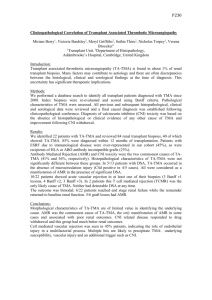
Peripheral blood film
10.8.15
• Anuric AKI - Commenced on HD
• Daily plasma exchange against octoplas
• Transplant biopsy 12.8.15
• CT chest/abdo/pelvis – no
lymphadenopathy/masses
• ADAMTS13 test – normal activity
• On advice of Prof Goodship – commence
eculizumab
Histology
Normal Glomerulus
Histology
Histology
Just to recap ..
• 33 yr old lady
• Kidney Tx 2011
• AKI, TMA
• Diagnosis: post – transplant TMA
Definition of TMA
• A pathological process of microvascular
thrombosis, consumptive thrombocytopenia and
microangiopathic haemolytic anaemia (MAHA)
• First described by Prof W Symmers in 1952
• Hallmarks of TMA
• Thrombocytopenia
• MAHA
• Renal impairment
• Neurological deficits
TMA – a feature seen in ..
• HUS
• Atypical HUS
• TTP
• Malignant hypertension
• Pregnancy
• Renal transplantation
• HIV
Post transplant TMA
• Recurrent disease
• Drug-induced (Tacrolimus, cyclosporine)
• Rejection
• Malignancy
TMA – laboratory features
• FBC : thrombocytopenia and anaemia
• Blood film: red cell fragmentation
• Coombs test: negative
• Haemolysis screen: elevated bilirubin and LDH, low
serum haptoglobins, high reticulocyte count
• Liver enzymes and coagulation screen: normal
• Serum creatinine: elevated in renal involvement
TMA – histological features
• Arteriolar thrombosis
• Intracapillary glomerular thrombosis
• Ischaemic glomerular tufts
• In native kidneys – biopsy adds little diagnostic
information
• In transplant kidneys – biopsy distinguishes
antibody –mediated rejection from other causes of
TMA
Let’s go back to the patient ..
• STEC –HUS unlikely as no diarrhoeal prodrome and
recurrence is rare in transplants
• Tacrolimus levels within range
• Anti HLA antibodies negative
• No rejection in biopsy
• Malignant hypertension absent
• No evidence of malignancy on CT scan
• Pregnancy test negative
• TTP less likely given renal involvement and normal activity
of ADAMTS13
• No family history of renal disease
Is this atypical HUS?
• Rare genetic condition
• First reported by Dr Conrad Von Gasser in 1955
• Often presents in childhood
• Diarrhoea prodrome less common
• Renal involvement predominates
• Disorder of complement dysregulation
• a low plasma C3 may be present
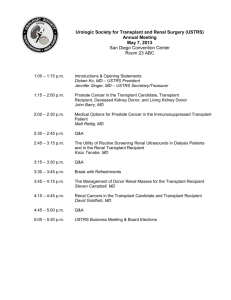
Initiation of complement activation, with amplification and downstream effects of the AP.
Thomas Barbour et al. Nephrol. Dial. Transplant.
2012;27:2673-2685
© The Author 2012. Published by Oxford University Press on behalf of ERA-EDTA. All rights
reserved.
Regulation of the AP of complement.
Thomas Barbour et al. Nephrol. Dial. Transplant.
2012;27:2673-2685
© The Author 2012. Published by Oxford University Press on behalf of ERA-EDTA. All rights
reserved.
Pathophysiology of aHUS
•
•
•
•
•
•
•
•
Disorder of alternative pathway
Over-activation of C3 convertase
Increased cleavage of C3b
C3a and C5a formation
Formation of lytic membrane attack complex (MAC)
Pathogenic surfaces are not just the target
Host cell becomes target – inflammation, cell damage
Renal vasculature (glomerular capillaries and arterioles) are
site of injury
• Endothelial cell injury – prothrombotic phenotype
Genetic mutations of aHUS
•
•
•
•
•
•
Complement regulatory protein mutation
Factor H, Factor I, MCP, Factor B, C3
Autoantibodies (anti CFH)
Combined mutations have been reported
Mutations carriers have 50% penetrance
Genetic/environment modifiers are required for disease
penetrance
• Identification of mutations important as they affect renal
survival, transplant outcomes and mortality
Screening tests
• Complement abnormalities
• Measure C3, C4, factor H, factor I before onset of plasma
exchange
• Screening for factor H autoantibodies
• Mutation screening of CFH, CFI, CD46, C3 and CFB
• Mutation screening of DGKE and THBD (when
recommended by national aHUS service)
Treatment
• Empirical treatment with plasma exchange
• Methylprednisolone
• Tacrolimus re-started
• Azathioprine changed to MMF
• Eculizumab
Plasma exchange
• Removes the abnormal complement regulatory proteins and
autoantibodies
• Replace defective complement regulators
• Started as soon as diagnosis made
• Should be given daily (minimum 5 days) until LDH, Hb and
platelet count normalizes
• Renal function is a marker
• Before the introduction of PEX, mortality of TMA was almost
100%
• PEX has improved survival to 90%
Limitations of plasma exchange
• Treatment resistant cases
• Dependence on PEX
• Requires central vascular access
• May develop anaphylactic reactions to plasma
replacement products
Eculizumab
•
•
•
•
Targets terminal pathway of complement activation
Inhibits C5a and formation of C5b-9 (MAC)
Prevents MAC attack on endothelial surface
However, risk of Nessieria Meningitidis is high – so need
vaccination
• Greater chance of renal recovery with early initiation
• Recommended once TTP excluded
• Treat for 6 months minimum
• Beneficial to those on dialysis as prophylactic treatment to
enable renal transplantation
The complement system is a major innate immune defence mechanism.
Veronique Fremeaux-Bacchi Clin Kidney J 2012;5:4-6
© The Author 2012. Published by Oxford University Press on behalf of ERA-EDTA. All rights
reserved. For permissions, please e-mail: journals.permissions@oup.com
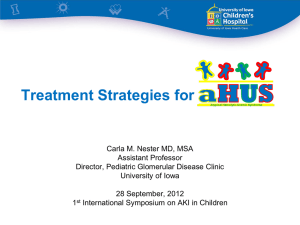
Figure 2 Recovery of renal function is better with a shorter interval between
onset of aHUS and initiation of eculizumab
Zuber, J. et al. (2012) Use of eculizumab for atypical haemolytic uraemic syndrome and C3 glomerulopathies
Nat. Rev. Nephrol. doi:10.1038/nrneph.2012.214
Prognosis
•
•
•
•
•
•
•
•
•
•
Poor prognosis -mortality and ESRD is 53% at 3 years
Risk of recurrent disease high -60%
90% subsequent graft loss despite plasma exchange
De novo aHUS – poor outcome with plasma exchange
Response from Eculizumab promising
Genetic screening allows refined prediction of recurrence
Living-related transplant contraindicated
Combined liver kidney transplant may help
CFH mutations are at highest risk of recurrence
MCP mutations have low risk
What is the future for the patient?
• Hope for renal recovery
• If recovers, how much residual function?
• If no recovery, then chances of re-transplant?
• Options for dialysis?
• How long should she continue with eculizumab?
• Family/job adjustments
Learning points
• Post transplant TMA – serious cause of graft injury
• Wide differential diagnosis
• Rejection must be excluded (thus biopsy crucial)
• Prompt diagnosis is vital
• Important to discuss with experts
Elementary, my dear Watson…
"How often have I said that when you have excluded
the impossible whatever remains, however
improbable, must be the truth."
Sherlock Holmes
Figure 3 Diagnostic algorithm and therapeutic options for aHUS
Zuber, J. et al. (2012) Use of eculizumab for atypical haemolytic uraemic syndrome and C3 glomerulopathies
Nat. Rev. Nephrol. doi:10.1038/nrneph.2012.214
References
1.
Complement Inhibitor Eculizumab in Atypical Hemolytic Uremic
Syndrome. Mache et al. CJASN Aug 2009 vol 4 no 8 1312-1316
2. Thrombotic microangiopathy and associated renal disorders. Barbour et
al Nephrol Dial Transplant 2012, 27(7): 2673-2685.
3. Complement-mediated injury and protection of endothelium: Lessons
from atypical haemolytic uraemic syndrome. Kerr and Richards.
Immunobiology 2012 Feb 217 (2); 195-203
4. Outcome of renal transplantation in patients with non shiga toxinassociated haemolytic uraemic syndrome: prognostic significance
of genetic background. Bresin et al. CJASN 2006; 1:88-99.
5. New insights into post renal transplant hemolytic uraemic syndrome.
Nat Rev Nephrol 2010; 7:23-35
6. Treatment of atypical uraemic syndrome in the era of eculizumab
Bachi et al Clin Kidney J 2012 5(1); 4-6
References
7. ASH 2012 haemotology education program
8. Symmers. Thrombotic microangiopathic haemolytic anaemia. Br Med J
1952 2:897-903.
9. Sommerfield et al. Thrombotic microangiopathy: case report and review
of literature. JASN 1992;3: 35-41.
10. Bell et al. Improved survival in HUS/TTP syndrome New Eng J Med
1991: 325: 398-403
11. Zuber et al. Use of eculizumab for aHUS and C3 glomerulopathies. Nat
Reviews Nephrology 2012 ; 8: 643-657.
12. Loirat et al. Plasma therapy in atypical HUS. Seminars in thrombosis
and haemostasis 2010. Vol 36 (6).
.