Transcript_GetImmunized
advertisement

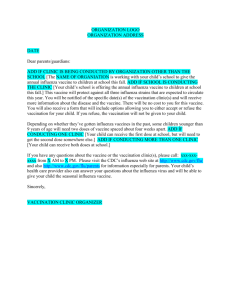
Event ID: 2704277 Event Started: 8/19/2015 12:59:21 PM ET Please stand by for real-time captions. Good afternoon. At this time, welcome to the 2015 Influenza update. All lines have been placed on mute to prevent any background noise. After the speakers remarks, there will be a question and answer session. If you would like to ask a question at this time, press --. If you would like to withdraw your question, press the pound key. Karen, you may begin your conference. Thank you Chris. Good afternoon everyone and welcome to the 2015 influenza update. As Chris said, this is Karen Boland. We are excited to have a variety of healthcare providers on our call today, including hospitals, nursing homes, physician offices and physician clinics. In addition we have some home care folks with us today. We are also excited to have our Iowa and Colorado staff. We have a number of other state colleagues joining us on the webinar. Thank you. I noticed there are a couple questions around the timing of the webinar. The webinar started at 12:15 PM central time. As Chris said, this is an operator assisted call. There will be time for questions at the end of the webinar. At the end of the webinar, please take time to fill the evaluation. It is meaningful for programs in the future. I want to share and introduce my colleague’s speaking today. Dr. Sheam Bakri attended the University of Pittsburgh graduate school of public health went on to work at the lake County health Department. After that, she went on to graduate with a Pharm.D. From the Chicago College of pharmacy at Midwest University. She has the experience of working with patients using medication therapy management and counseling, education and disease state management. Here, at Telligen, she works on the ADE and multiple other tasks and facilities quality improvement initiatives. She works with teams across Illinois integrating clinical pharmacy expertise the into patient care practices. Our second speaker will be Dr.Paul Mulhausen. He received his medical three from the University of Minnesota, his Masters in public health sciences from Duke University and completed his postgraduate training at the University school of medicine. Prior to joining Telligen, he worked as a member of the faculty at the University of Iowa's Carver College of medicine and served various clinical and educational roles. He has multiple other roles with the Iowa medical society. He is speaker for the House of Delegates as well as treasurer for the American geriatrics Society and he still sees patients. It is my pleasure to turn the program over to Dr Bakri after I review the objectives today, briefly. We want you to understand what the 2015 recommendations are in terms of who should be vaccinated. We want you to understand the different types of vaccines available, be able to understand what the immunization rates are across in various age groups and the demographics and really, we want to focus so that you are well prepared to encourage your staff to actively to get protected by being immunized. So, I will pass it to you Dr Bakri. Thank you Karen. Good afternoon everyone and thank you for joining us. As Karen said, I would like to discuss the recent updates and recommendations from the advisory committee on immunization practices or as better-known, the ACIP. For those of you who may not be familiar with them, they are a group of medical and public health experts that develop recommendations for how to use a vaccine to control disease. The recommendations were released for the 2015, 2016 influenza season and are all essentially the same as last year's recommendation with the exception of one change. Last year's flu season, it is recommended the use of a nasal spray vaccine which is a life, attenuated, influenza vaccine. The recommended live virus for healthy children ages two through eight, so long as there are no contraindications. However, in February of this year, the committee did renew the product -- the recommendation for this current flu season. I would also like to note that this is not a comprehensive list. Please a visit the website for more information on the guidelines. As you can see, all persons six months and older should receive the influenza vaccine. There is no preference of live over inactivated. Please be aware that the only live, attenuated influenza vaccine that is available is indicated for ages two through 49 years old. With regards to the ACIP, everything else is the same as last year. Again, less than two and greater than 49 should not be vaccinated with the live vaccine. If there are any concerns, patients shouldn't use it. If the patient is pregnant, patients are compromised, and of course, those with a history of egg allergy should not be vaccinated with the live vaccine. I honestly include this for you to read it at your leisure. What I try to remind you as a provider is to ask your patients that you are vaccinating whether they are personally or if they are living with someone who is immunocompromised. You really should avoid contact with such persons for about seven days after receiving the live vaccine. Honestly, because of the theoretical risk for transmission of a live attenuated vaccine virus to those persons. So, this year we have a mixture of trivalent versus quite revealing. The of live and inactivated. We also have recombinant available. There have been a few changes in this year's batch of flu shots. So, this year, as like last year, the California strain and Switzerland strain has been included. This will cover the H3N2 strain. This slide shows the various trivalent vaccines available this year. The trivalent vaccine includes A California, A Switzerland and B Phuket. This shows the quadravalent. Each specific information relates to the flu zone. Patients younger than 18 and older than 64 should not receive the intradermal flu zone. The age indication and the pathogen certification is five years old. However, it was recommended that it not be used in children ages six months through eight years of age. This is because of the increased risk of -- reaction. -- Seasonal influenza vaccine is available for a child, who then have a medical condition, it increases the child's risk for complications. Then, this could be used. Our, providers should consult the parents and caregivers that the benefits -- should inform the caregivers of the concerns. This slide doesn't contain anything you haven't seen. This is standard contraindications and precautions. This is for both the trivalent and Quadravalent. Next we have inactivated cell culture based vaccine. It was approved and 2012. This is the only cell culture-based flu vaccine. It is good for patients 18 years and older. -Refers to how that vaccine is manufactured. These are similar to the egg-based vaccine but they are grown on the -- cells. A major advantage of the cell culture technology includes faster startup -- keep it frozen and ready. Doing so assures an adequate supply cells readily available for vaccine production. Is not dependent on this. Side effects include the pain and redness and soreness at the site of injection, but something that is not included in the package insert is that, albumin, is used in this process. So, theoretically, caution should be used with patients who are allergic to eggs or have egg allergies. Next, we have the flu mist. It is the only approved in the US. It is served bit natal to nasal spray. As you can see, it is indicated for patients from ages 2 to 49. This is pretty much identical to the ginning of the presentation but I included it just for you to have everything on one slide so you can reference every thing easily and quickly. It's really interesting because it was improved a couple of years ago. It was the only egg free vaccine in the US. The production method is not required egg growing vaccine and does not use chicken eggs at all. Only egg free vaccine available in the US. The way this vaccine was actually used, proteins were made from a wild type vaccine virus that are combined with another virus and are grown within insect cells. They are then allowed to replicate. Advantages of this process is that the vaccine can be reproduced in the shortest amount of time. It doesn't depend on the egg supply. Again, the traditional precautions should be used with this vaccine. This does conclude my portion of the presentation. I liked to turn it over to Dr. Paul Mulhausen. Thank you. Karen gave me such a nice introduction at the start of the program. But, I have to correct at least one of those things. I am not chairman of the American geriatrics Society. Although, that would be a wonderful opportunity for me. I am chairman of the clinical practice and models of care committee which is a small, volunteer arm of the American geriatrics Society. So, if you give me a call thinking I can move the American geriatrics Society for you, I cannot. But, I appreciate the confidence that Sharon, I mean Karen expressed in that sentiment. And then, it is wonderful to follow-up after -- because that was a terrific review of the vaccinations, influenza vaccinations that are available to us. The last thing I have to point out is, if you look at the WebEx I am an internist and geriatrician. Karen is correct. I continue to practice for one of the week at a federal quality -- qualified health center. Let's get started. My task here is to give an overview of the influenza illness, discuss with you some issues related to the vaccination and specifically the mismatch that took place last year between the vaccination and the predominantly circulating influenza virus over the course of the flu season last year. And, we'll talk some about how to overcome barriers to the vaccination. In all honesty, our discussion about the mismatch is so that you are informed when you're patients come to you this year and say, why should I get the flu shot? There is this huge mismatch and it didn't work last year. Have some additional information that you could use. You engage them in conversations about why to get the influenza vaccination. So, let's just start out with the actual flu. So, influenza, which we commonly call the flu, is actually the most frequent cause of death from a vaccine preventable illness in the US. So, it is a serious healthcare problem. Influenz a A is a highly contagious disease. And, it makes us ill by attacking the body’s airways. After you get exposed to the virus, only takes one to four days for you to become ill. The signs and symptoms of the illness include fever, high fevers in fact, headache, cough, runny nose, nasal congestion, and really prominent muscle aches. I have had the misfortune of having a full-blown case of influence at least once my career and what I recall from that experience was just that my muscles felt like I had gotten beaten up because of the severity of the myalgias during the illness. Each year somewhere between five and 20% of us develop influenza. It will result in 200,000 hospitalizations each year. It is estimated that somewhere around 35,000 influenza associated pulmonary and cardiac deaths take place each year in the United States. When an outbreak occurs, as many as 10% to 40% of people are attacked by the virus. My story, as a clinician is an influenza outbreak in a nursing home. Early in my career as a clinician, I worked extensively in rural, long-term care settings in Iowa. During the course of one of the seasonal influenza outbreaks, I was working in a nursing home in which, on one day, everybody was well. And, within three days, a third of the people had developed an influenza like illness that proved to be influenza A. A third of those people died. It was an incredibly sobering experience. It really brought -- it made it very concrete for me to understand just how severe this illness can be and the potential impact it can have on the lives and health of our patients. This is a bad healthcare problem. Influenza spreads primarily through the air. You see this picture here. This is a man sneezing and the droplets - Spittle, I guess you would call it, respiratory droplets. That is the primary motive of transmission. So, coughing, sneezing, even talking can generate these that can spread the virus incredibly fast. And important part to note in light of this incredible contagious problem is that people infected start being contagious the day prior to showing signs and symptoms. So if you get exposed to somebody with and for once, you breathe in the respiratory droplets, you don't yet know you are getting sick but you are starting to show the virus and you can be contagious. Even though it is one day before you recognize that you might have the flu. It is important to recognize, it is spread by air droplets. When those get on your hand, you can spread them by person to person contact. Preventing the flu is probably the most effective strategy we have two remain healthy and avoid competitions of influenza. Vaccination remains the single best way to prevent the flu. If you spend some time looking at the research on the influenza vaccine, you see that there is very good evidence that it reduces the severity and frequency with which people have flulike illnesses. It reduces the need to go to the doctor. So, we use fewer healthcare resources. Those could be applied to other conditions. And, we don't have to be inconvenienced by the need for a visit to the doctor because of an influenza A like illness. It has been mistreated to prevent flu related hospitalizations and deaths. If you are as interested in antimicrobial stewardship, is also useful to know that a vaccination, does it reduce the frequency of this influenza like illness and influence of. It reduces the need to use antibiotics and the over-the-counter medications that people use to manage their symptoms of influenza and influenza like illnesses. So, take-home point is, vaccination remains the single best way to prevent the flu. Many people come up -- have asked me the question, why do I have to get the influenza vaccine every year? I put this slide in here to illustrate, how the circulating virus, how it can change from year to year. Hopefully this slide is clear to you. You can see I put the distribution of circulating viruses for the 2012, 2013 influenza season. You can see that the various subtypes of influenza viruses change from year to year. For instance, look at the 2012, 2013 curve. You can see the dominance of the red bars that represent the influenza A type. And a contrast that with the 2013, 2014 where the predominance of bars is the orange, the 2009 virus that many of us learned to call or learned about, as the swine flu. You see that is from year to year. The virus that circulates predominantly changes and the time at which those viruses are circulating can change. So, just to reflect the time, take a look at 2012 and 2013. You can see the influence of the influenza B virus was prevalent through the entire season. Contrast that with last year. The influenza B virus was the dominant virus circulating at the tail end of the season. So, both the timing of viruses circulating and the actual types of viruses circulating, each season can change from year to year. Therefore, the influenza vaccination has to be tailored for the expected virus to be circulating and new vaccination has to be received every year to optimize the preventive protection from the influenza vaccination. We recognize the information we just talked about is relatively complicated. If you questions about it, we can discuss it more in the question and answer session. Last year there were a lot of concerns about a mismatch. The point I really want to make here, by showing you the last three seasons as well as being very open about what happened last year is that, the flu vaccine is really an excellent preventive option. It is not perfect. Last years’ experience with the influenza vaccination illustrates the imperfection. So, if you take a look at this graph which shows the types of influenza viruses that were circulating through last year, 2013, 2014, you can see the predominance of red and yellow. It was a really peeking around the turn of the New Year. In the right gray box you can see the virus that were contained in the 2014, 2015 influenza vaccine as their color-coded for that you can see there is not a red in there. So, the Reddit virus, which was the specific strain of the -- virus was not effectively covered by last year's influenza vaccination. But, importantly, if you look at that tail end of the season, where all of the green bars are located, at the tail end of the influenza vaccination was the predominant --. The predominance of the B which was actually covered by last year's influenza vaccination. So, we got it partially right but we didn't get it perfect. In general, you look at, from year to year, two year, the vaccination generally, nicely matches with the influenza virus types that are circulating the year of the vaccination. If you look at the overall effectiveness, you can break this down by effectiveness. The centers for the disease control has its own methodology to define effectiveness. I won't get into that. I need this to say, you can use these numbers to compare effectiveness. If you look down at the bottom, the fifth bullet point there, where it would be mismatched you can see it was only 9% effective against that particular virus type a year ago but against the other viruses that were circulating over the course of last year's flu season, you can see that the virus, the vaccination was really quite effective and certainly, as effective as the vaccination in previous years. So, it worked very well against the matched viruses that were circulating last year. It just did not work well with that influenza A virus that was really circulating in December influenza A virus. So, it is a good intervention. It is an excellent preventive measure, but like all of our treatments, it is not perfect. One strategy to improve its effectiveness is to give more of us vaccinated you can see here that there is considerable room for improvement. If you look at the experience of 2013, 2014, again, what we're finding is that only around 40% of those eligible for the influenza vaccination get vaccinated. And so, there is considerable room for us to improve the vaccination of both healthcare providers and our patients. So, more of us can get the influenza vaccination. We are here to put out early recommendations for the influenza vaccination. So, I asked the question, if only around half of us get the flu shot, why aren't the other half getting the flu shot? This has been studied quite a bit. I think these are the takehome points. The conversation that you are patients will bring up with you. Many under estimate the impact of influenza. It is just the flu. What a big deal. I would have to say, maybe earlier in my life I felt that way until I actually had a flu bone just fullblown case of the illness. When I watched what happened in a flu epidemic, it really is quite a severe illness. It has a lot of potential to degrade both the quality of life and health of the patient. People underestimate the morbidity. One of the things we anticipate hearing a lot this year, last year the flu shot did not even worth. That is why I wanted to share with you the details around what happened last year. Some people say I cannot afford it. Some people underestimate the need for the annual vaccination. Again, highlighting the importance of understanding how the virus changes from year to year. Many people have a fundamental concern about vaccination. I have heard over and over again, patients say, my friend took the flu shot and they got the flu. And of course, concerns about discomfort. Lastly, I want to highlight that many people do not know that they needed. This is the dominant theme . They have never been told by their healthcare provider, you should get the flu shot. So, most of the people say, why didn't you get a flu shot? They didn't know they needed it. That has important applications for us as we interact with patients. Last year, when we discussed the influenza vaccination, we spent a lot of time busting the myths. Some of these myths have come up in the previous slight. For instance, the concept that the flu vaccine will give you the flu has and busted over and over again. The injectable flu vaccinations are inactivated. They can't give you influenza. The experience the people are describing is, and influenza like illness from another virus that people sometimes get during the flu season around the time they get the flu vaccine. So, there is a number of myths surrounding the influenza vaccination that you should be aware of and that you should be prepared to address for your patients. One of the things I've learned over the years is that people strongly hold to some of these myths. Pointing out the incorrect belief can sometimes get them over the hump. I think there are some other strategies, more than just educating people, that can be equally or even more effective at helping to break down the barriers that our patients experience with it comes to the influenza vaccination. I want to spend some time on these particular strategies. Providing a strong intentional message, it is the whole issue of, your doctor recommends this. And intentional messaging program during the season that presents the opportunity to provide the vaccination. Building systematic reminders. There is a significant body of literature that says, for those patients who do not ask for the flu shot, they have a higher probability of not getting it than those they come in and ask for the flu shot. Building systematic reminders into our daily work and help us to break down the barriers for those who are thinking they should be asking when they are at the healthcare setting. Standing orders that allow the nonphysicians give the vaccination will be important. In my own practice, the whole strategy, they have standing work orders so that the nurses could ask, did you have the flu shot and if not, deliver the vaccination so it didn't require me to write an order. Safety of vaccination but also empathically recognize concerns. There are and continue to be uncertainties around surrounding the influenza vaccination. Think about last year. Last year there was a substantial mismatch. That is a reflection of some of the uncertainty. When patients raise concerns, there is something we don't know about the influenza vaccination. I think it is important to acknowledge the concepts yet bring up the fact that it can potentially help them move to a position of choosing to receive the vaccination and helping to educate them about their preconceived and incorrect notions of the influenza vaccination. It is helpful to message the potential to protect loved ones. Many people are motivated to receive the vaccination to actually prevent the spreading of the illness to others rather than worrying about themselves. And then, ask about the barriers. Many of our partners have incorporated these strategies into their practice. We asked some of them to share their best practices with us so that we could bring those best practices to you. Over the next three slides, I tried to highlight some of the responses we received from our partners. This particular one describes a scenario in which a physician interacts with a patient who has chosen not to receive the influenza vaccination. I think there are several really important points highlighted. One is a very patient center approach that validates the concerns of the patient. In the phrase, I can respect that decision. In messages the potential to protect loved ones in which it says, you can actually carry the flu and spread it to somebody else. And, it acknowledges some of the uncertainties around the influenza vaccine when the provider or physician says, I know that number has been called into question. Being able to empathically respond, and acknowledge some of the uncertainty and build a strong message of advocacy for the vaccination and trying to incorporate our generous motivation to protect others. It is being applied in this particular best practice. Here, we see another partner who shares their best practices. What they have done is a breakdown the workflow barriers. They have reduced the inconvenience barrier that many of our patients experience when they go to get a flu shot. How many of us say they won't sit in a doctors office for half a day to get a flu shot. It reduces the inconvenience barriers. This particular practice is being incorporated interest to vaccination clinics which I see is very innovative. They built systematic reminders, both into the workflow and into outreach. They are sending reminders to their patients and reaching out to them with telephone calls. They are using standing orders so that the nurses and their practices can both advocate for the influenza vaccination and administer it without having to disrupt the workflow of the visit -- the physicians with whom they work. Our partners incorporated the strategies to optimize the application of the influenza vaccination. Here is what happened. Once people start to get it, they start to become believers and as they start to share their own personal experience with the vaccine, they breakdown additional barriers through their own peer to peer testimonials. I think some useful experiences from the field of our clinical partners. Lastly, in terms of influenza prevention, I want to spend a little bit of time discussing the importance of hand washing. It very important because of the air droplet spread through respiratory secretions. Handwashing can also be a helpful part of the prevention strategy. Live viruses can live in the environment on nonporous services and the transmitted for up to a day. Handwashing becomes an important strategy for preventing the spread of the influenza virus. I want to make sure that some of our messaging includes handwashing, especially among healthcare professionals. Now, knowledge sharing is something we could do as well. Remind people of the indications. Everybody over the age of six should be vaccinated if they have no contraindications. If there is a contraindication, you may want to explore some alternatives. Getting vaccinated as soon as possible, as soon as the vaccine is available is a reasonable strategy for us to share with our patients and colleagues. It is possible to get a respiratory virus during the flu season which is white many people think they get the flu from the vaccination itself. It is important to share with people how the virus spreads because, it is difficult the block that spread through the air droplet and the vaccination proves to be the most effective strategy. I think it is important to share that people can be contagious one day before the symptoms appear. What can we all do? Get the vaccination as soon as possible and encourage patients to get the influenza vaccination as soon as possible during the course of the influenza season. I wrote here, avoid contact with sick people. I don't mean all sick people, I mean people who have influenza like symptoms. Limit your contact with others who have influenza like illness and of course, when you have an influenza like illness, you want to limit your contact with others. Encourage handwashing as part of the strategy. Cover your nose and mouth with a tissue. Be careful as you touch your eyes, nose, and mouth so you do not spread the virus through contact with secretions. And then, of course, keep the workplace and the home clean. Alcohol-based hand rubs are effective for killing the influenza virus when it is on our hands. So, that concludes my portion or least my dedicated portion of the presentation. This is an opportunity for us to have some questions and answers. I will pass the ball back over to Karen so they can manage the WebEx during the time for question and answers. And, thank you for letting me speak. But I much time for Q&A, but if there's anyone who has a question, we will be happy to entertain its. Or if you want to type into the chat, we get back with answers. Pam Nelson. Your line is open. No question. Thank you. There are no further questions at this time. Okay. Thank you. If any of you have questions, we can get the questions to the most appropriate person. As you sign off, you should drop into an evaluation. I ask you please complete the evaluation and provide suggestions for topics you would like to hear about in the future. Thank you for joining. I hope you have a great day. We have one question about Tamiflu. If people have symptoms after a couple of days of Tamiflu, what are your recommendations? The earlier in the course of the illness that you start Tamiflu, the more effective it will be. I think it is 72 hours into it, it is not effective. Cannot be confirmed? Yes. I agree. It needs to be taken within 48 hours of symptoms. For those of you with difficulty getting slides and handouts, there are specific directions for how to slides are available. There are directions that will tell you about this. In the of issues and you cannot do this, type in my email address and I will be happy to forward it to you. I think we have exhausted our time. I like to thank all of you again for joining. Again, have a good afternoon. Thanks. Thank you everyone. This concludes today's conference call. You may now disconnect. [ Event concluded ]