Hernias - OU Medicine
advertisement

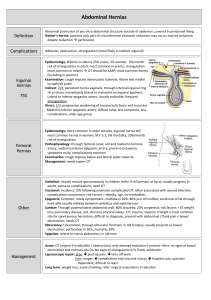
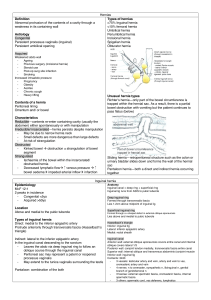
Hernia, Hydrocele Stephen Confer, MD Ben O. Donovan, MD Brad Kropp, MD Dominic Frimberger, MD University of Oklahoma Department of Urology Section of Pediatric Urology 3 year old male Incarcerated Inguinal Hernia Hernia Reduction • Unable to reduce: OR • If extremely difficult (sedation): repair next day • If able to reduce without sedation: repair soon From Surgery of Infants and Children, Oldham, et. al., 1997 Inguinal Hernia • • • • Most can be reduced in clinic or ED Bowel usually OK if able to reduce 17% reincarceration rate Beware the “inguinal node’ in females – incarcerated ovary From Atlas of Pediatric Surgery, Ashcraft, 1994 Overview • • • • Review Anatomy Biostatistics Operative Description Advanced Laparoscopic Anatomy • EBM-Core Competency DEFINITION • ”…..an abnormal protrusion of a viscus through its containing wall” Anatomy BOUNDARIES OF INGUINAL CANAL • • • • FLOOR: Inguinal ligament ANTERIOR WALL: External Oblique POSTERIOR WALL: Transversalis fascia MEDIAL-POSTERIOR WALL: Internal oblique and transversalis (when they fuse become conjoint tendon.) Inguinal/Scrotal Anatomy From Surgery of Infants and Children, Oldham, et. al., 1997 CONTENTS OF CANAL 3 ARTERIES: • Testicular Artery • Artery to Vas • Artery to cremaster 3 LAYERS OF FASCIA: • External spermatic fascia • Cremasteric fascia • Internal spermatic fascia. 3 NERVES: • Genital branch of genitofemoral nerve • Sympathetic fibres • Ilioinguinal nerve 3 OTHERS: • Vas deferens • Panpiniform plexus • Lymphatics ANATOMICAL DEFINITION • • • • INDIRECT Lateral to IEA Outside Hasselbach triangle. Therefore hernia goes from DR SR scrotum. Therefore, indirect hernias are controlled @ deep ring • • • • DIRECT Medial to IEA Inside Hasselbach triangle. It is a bulge in fascia transversalis. Therefore if bulge medial to fingers at deep ring it is direct. ANATOMICAL DEFINITION • Note that scrotal swellings are usually indirect. • However, large directs can cross superficial ring and enter the scrotum. This is rare. • An indirect and direct hernia occurring simultaneously is termed a pantaloon hernia. Biostatistics • All ages • Both sexes • % Incidence: Inguinal 80% Incisional 10% Femoral 7% Biostatistics • Approximately 700,000 hernia repairs are performed as an outpatient procedure each year • Approximately 75% of all hernias occur in the inguinal region • Approximately 50% of hernias are indirect inguinal hernias • A vast majority occur in males • Hernias more commonly occur on the right side Etiologies Increased Abdominal Pressure: • Heavy lifting • Chronic cough • BPH • Constipation • Ascites Weakened Abdominal Wall: • Increasing age • Malnutrion • Collagen disorders • Smoking Diagnosis • They may describe minor pain or vague discomfort associated with the bulge • Extreme pain usually represents incarceration with intestinal vascular compromise • Paresthesias may be present if inguinal nerves are compressed Surgical Management of Inguinal Hernias • Inguinal hernias should be surgically repaired following diagnosis by physical exam • The natural history of groin hernias is one of progressive enlargement and weakening with the potential for incarceration and obstruction of the intestine • Hernias do not resolve spontaneously or improve with time • Wearing a truss does not cure a hernia The Operation • The incision is made two finger breadths above the inguinal ligament • Careful dissection through the subcutaneous and external oblique fascia is made • The spermatic cord is mobilized • The cremasteric muscle fibers are divided and separated from underlying cord structures • The hernia sac is dissected from the cord structures and opened • The neck of the sac is suture-ligated at the level of the internal ring (excess sac is removed) Specific Surgical Procedures • Laparoscopic hernia repair – Early attempts resulted in exceptionally high reoccurrence rates Practice based learning and improvement • Prospective Randomized Controlled Trial to compare skin staples and polypropylene for securing the mesh in inguinal hernia repair. • British Journal of Surgery 1998, 85,790792. Ratliff et. al. Compare 2 fixation methods • • • • • 50 men unilateral inguinal repair Reevaluation in 6 and 12 weeks. Staple time 20 min Suture time 29 No difference in pain scores Inguinal hernia in bulls