Chief Financial Officer - Hull and East Yorkshire Hospitals NHS Trust

HULL AND EAST YORKSHIRE HOSPITALS TRUST
ANNUAL GENERAL MEETING
SEPTEMBER 2015
ANNUAL ACCOUNTS 2014/15
Lee Bond
Chief Financial Officer
FINANCIAL PERFORMANCE REVIEW 2014/15
The Trust achieved all of its financial duties in 2014/15
To Break Even on its Statement of Comprehensive
Income
To achieve a 3.5% Return on Capital
To operate within our External Finance Limit
To operate within our Capital Resource Limit
BREAK EVEN DUTY
As an NHS Trust we are required to at least break even. For the eighth successive year we achieved an operating surplus, with a surplus of £2.9m for
2014/15.
2007/08
£m
6.8
2008/09
£m
5.0
2009/10
£m
7.6
2010/11
£m
4.6
2011/12
£m
4.8
2012/13
£m
5.4
2013/14
£m
5.9
2014/15
£m
2.9
Total
£m
43.0
The £43m we have generated over the last 8 years has been used to repay loans and invest in our property, plant and equipment.
We generate surpluses so that we can ensure a sound financial basis for the future particularly recognising the challenging economic environment.
The Trust received a clean External Audit opinion (i.e. the financial statements give a true and fair view of the financial position of the Trust and have been properly prepared in accordance with the directed accounting policies).
UNDERLYING FINANCIAL POSITION
The Trust reported a surplus in 2014/15 of £2.9m. This was achieved through the benefit of nonrecurrent items totalling £10.6m which included winter resilience funding and part year benefits from slippage in specific developments including Francis and Keogh related clinical staffing investments. Without these items the Trust would have reported a deficit of £7.7m.
For 2015/16 the Trust had an initial planned deficit of £21.9m which reflects the underlying position from 2015/16 along with new cost pressures from the following:
•
Partial delivery of the 2014/15 efficiency program and only partial development of a program for 2015/16
• Increased Clinical Negligence costs
•
Cost of investments, for example in the new medical model within the Trust and in the new patient administration system
As a result of the planned deficit the Trust’s External Auditor made a referral to the Secretary of State under Section 19 of the Audit commission act 1998 that the Trust is likely to break its statutory break-even duty in 2015/16.
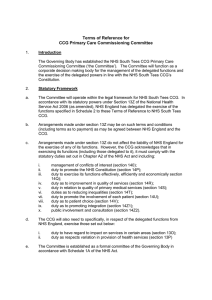
WHERE DOES OUR MONEY COME FROM?
Our income in 2014/15 was £527m, as shown below.
5%
5%
4%
23%
30%
NHS England: £157m
Hull CCG: £175m
East Riding CCG: £123m
Other CCG: £24m
Education & Training: £26m
Other: £22m
33%
HOW DO WE SPEND OUR MONEY?
Our expenditure in 2014/15 was £512m, as shown below.
3%
5%
9%
23%
60%
Pay: £305m
Clinical supplies and services: £117m
Other supplies and services: £15m
Premises & Establishment: £28m
Other: £47m
This year the cost of salaries and wages increased by £10M to £305M.
INVESTMENT IN INFRASTRUCTURE
We invested £18.8m in property, plant and equipment
(£m)
Major Building Projects
New Emergency Department
New Ward Block
– Ward 500
4.8
4.1
Equipment
Medical and Scientific Equipment
Information technology
Other
Backlog maintenance and Compliance
Other
3.6
1.0
TOTAL SPENT
1.8
3.5
____
18.8
____
In 2014-15, we also bought:
THE FINANCIAL FUTURE
• We expect demand for NHS services will continue to increase, but expectations are changing as to how and where that care should be provided.
• We will need to make changes in the way services are provided .
– Clinical Commissioning Groups are looking for services to be provided within the community rather than in a hospital setting
– Care should be more personalised to the patients needs
• Patients expectations about the quality of care that they receive will not change. Quality is not optional.
• Funding will be limited as the NHS faces a massive financial burden with estimates of a £20-30bn challenge by 2020
– The Trust will need to improve efficiency and productivity to deliver services within the funding available.
IN SUMMARY
• Historically we have delivered within the financial constraints we face but
2015/16 marks a stepped change in the size of the challenge being faced. This challenge is not likely to get easier over the next 5 years
• Sound financial management is a prerequisite for future success .
• Our financial plans reflect our desire to provide services locally that are safe, high quality and which meet the requirements identified by the Care Quality
Commission.
• The Trust is committed to developing a Financial Recovery Program. This is not a quick-fix. The level of transformation and change required will take time if services are to be provided safely throughout.
• The two keys to this are:
1. Transformation of our services to make them more efficient and productive
2. Collaborative working with commissioning colleagues and the wider health and social care economy.