The Case for a New Model for Training Requirements
advertisement

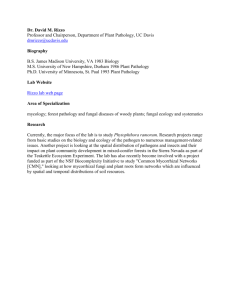
The Case for a New Model for Pathology Residency Training Requirements Ron Domen, MD Penn State Hershey Medical Center and College of Medicine Hershey, PA Special Thanks to my Co-Author • Jennifer Baccon, MD, PhD • Domen RE, Baccon J. Pathology residency training: time for a new paradigm. Human Pathology 2014;45:1125-1129 Historical Notes • Prior to 1900 – pathology was the study of “morbid” anatomy (autopsy) • 1900 – AMA established “Section on Pathology and Physiology” – Helped to define scope and educational requirements – 1924: Minimum training for a pathologist: preferably some hospital experience, 2 (better 3) years of “special study under a good pathologist in a laboratory where there is plenty of material” • Early 1900s – clinical physiology and clinical chemistry increasingly became aids in disease diagnosis and treatment and began to define “clinical pathology” as a separate area of medical practice Historical Notes (cont) • In the early decades of the 20th century “clinical pathologists” also performed AP duties (Today, should CP more properly be called, Laboratory Medicine?) • Pre-WW II – growing numbers of hospital and state-run clinical laboratories with increased oversight by pathologists • 1932 – ASCP designated an arbitrary time of 3 years of study for qualification in clinical pathology (accepted by the Council on Medical Education and Hospitals of the AMA) American Board of Pathology • Formed in 1936 • 1938 examination requirements (5 years) – – – – • • • • Clinical internship (1 year) Clinical pathology training (1 year) Pathologic anatomy (2 years) Additional pathology training or practice in pathology (1 year) 1973/74 - Clinical internship year eliminated 1985 – fifth year added (intention was to be a clinical year) 2002 – fifth year eliminated 2002 – present: AP (18 months) + CP (18 months) + Electives (12 months) Thomas M. Peery, MD JAMA 1959;171(15):2065-2068 “This rapid expansion of services accounts for most of the pressing problems which confront the clinical pathologist today. First and foremost, we find that no one pathologist can possibly encompass all that must be known for the proper expansion and development of laboratory services.” Townsend JF, Van Peenen HJ, Senhauser DA, Lucas FV. J Med Educ 1971;46:456-460 “Physicians preparing for academic careers really require more than four years of educational experience to become competent in clinical and anatomic pathology. In the authors’ experience, they need six years. At end of that time, they…have begun to attain depth in one area of pathology.” Gorstein F, Weinstein RS. Hum Pathol 2001;32:1-3 “Remarkable scientific advances have broadened the potential scope of practice and have made mastery of the entire body of pathology information an impossibility.” Christopher N. Otis, MD Hum Pathol 2006;37:929-931 “Aside from the basic medical knowledge in anatomic pathology, the other areas [molecular pathology, cytogenetics, bioinformatics, management skills] are different angles on the same topics necessary for clinical pathology training…Is it time to consider an entirely new approach to residency training in pathology, an approach that allows for training in the basic core competencies while providing enough latitude for the trainee to differentiate throughout training?” The Current State • 2-plus-2 years paradigm of combined AP/CP training – Minimum of 18 months in each area – 12 months of elective time – Up to 6 months of research • AP-/CP-only (24 months + 12 months of electives) • Employers increasingly want fellowship trained graduates • >90% of residents pursue a fellowship (30-40%, 2 fellowships)* – – – – Required for a desired position To enhance their skills and develop area(s) of expertise To enhance their ability to secure employment (top 6) surg path, cytopath, hemepath, GI/hepatic, dermpath, forensics *2014 ASCP Survey; and, Lagwinski N, Hunt JL. Archiv Path Lab Med 2009;133:1431-36 The Current State (cont) • What do employers want/look for: – – – – – Diagnostic competency Fellowship training (surg path, dermpath, cytopath, bb/tm, GI path) Strong interpersonal and communication skills Laboratory management and administrative competency Professionalism (cooperation, collegiality, flexibility, knowing when to ask for help, etc) – Able to engage with, and understand, clinicians and can serve in the role of consultant – Able to work well with others at all levels, be involved with medical staff governance, and be an advocate for pathology (leadership skills) • Most of these are “cross over” skills that could be learned as part of an AP-only program with 1 or 2 areas of concentration in CP Hum Pathol 2006;37:969-73; Arch Pathol Lab Med 2007;131:545-55; Arch Pathol Lab Med 2009;133:1139-1147 The Current State (cont) • What employers are getting: – Nearly 1/3 of new hires have a major deficiency in a critical area, and 71% of employers report difficulty hiring entry-level pathologists. Why? (for example): • Preparedness in clinical and administrative areas • Inadequate training/experience – Independent sign-out in surg path and clinical decision-making – Poor technical proficiency • Laboratory management and administrative skills • Professionalism and Work Ethic – – – – – Unrealistic expectations about work-load/hours Interpersonal and communication skills Flexibility regarding responsibilities and willingness to acquire new skills Interpersonal interactions Honesty and reporting/recognizing errors • Regulatory and compliance skills/knowledge Arch Pathol Lab Med 2007;131:545-55; Arch Pathol Lab Med 2009;133:1139-1147; and, Post MD, et al. Employer expectations for newly trained pathologists…(manuscript submitted). Why Change the Current Training Model? • Knowledge is rapidly increasing and changing • Current graduates are not optimally prepared • Maintaining competency in all areas of AP and LM/CP (shortand long-term) is unrealistic • Many/most graduates are currently pursuing fellowships and specializing/sub-specializing • Community practices are increasing in size allowing for/requiring more specialization – changing practice patterns (impact of ACA?) • Acquiring the basic LM/CP skills needed in community practice can be obtained in both AP- and CP-only programs either as part of core training or during a focused fellowship • Tailoring MOC requirements should become easier Why Change? (cont) • Is length of training less important than subject mastery? Achievement of defined competency and outcome goals/Milestones? • Does a “one size fits all” approach to length or content of training make sense in light of the current gaps in training, knowledge explosion, and employer needs? • Could changing the training paradigm offer more standardization of content and increased educational opportunities across all residency programs (large vs small programs)? Role of technology? • Future of reimbursement for GME? • Impact of student loan debt on career choice and length of training • Pathology is ever-changing and expanding and more tailored approaches to training are called for Proposed Changes in Residency Training APC Park City Report on Combined AP/CP Residency Training (Oct 1988) • 3 years combined AP/CP training to include overlap areas (molecular pathology, computer science, management) • 2 years of additional training which could include: – – – – General AP and/or CP A subspecialty of pathology Research A clinical year (IM, Peds, etc) • AP/CP ABPath certification after 5 years of training • Up to 1 year of subspecialty training during the 5 years could count towards certification in that subspecialty • AP- and CP-only training would still be offered Wells A, Smith BR Clin Lab Med 2007;27:229-240 • More and more community practices are getting larger where specialty-based practice can more easily occur • Many (most?) residents choose AP/CP training because most will go into community practice (where <20% of their time will be spent on LM/CP issues) • Full global skills in LM not required and targeted expertise in 1 or 2 areas of CP could be obtained Wells A, Smith BR. The goals of resident training in laboratory medicine in combined anatomic pathology/clinical pathology programs: an overview. Clin Lab Med 2007;27:229-240 Rethinking Pathology Residency Training (Domen RE, Baccon J. Hum Pathol 2014;45:1125-1129) Core AP/LM(CP) Training AP-Only Track Fellowship (1-2 years) Cytopathology Dermatopathology Forensic Pathology Hematology Medical Microbiology Molecular Genetic Pathology Neuropathology Pediatric Pathology Surgical Pathology Selective Pathology Clinical Informatics Research 24 months 12 months of AP and CP rotations or other clinical rotations tailored to resident’s career plans LM(CP)-Only Track Fellowship (1-2 years) BB/TM Chemical Pathology Hematology Medical Microbiology Molecular Genetic Path HLA Selective Pathology Clinical Informatics Research Barriers Against Change • Impact on residency training programs? • Impact on patient care/pathology work-flow in hospital? • Significant changes in current ABPath and RRC policies (and Milestones)? • Affect on billing, hospital contracts, CLIA regulations, etc? • Impact on community practice; small groups vs large(r) groups? • Job market concerns in general? Academic vs private/community practice? • Would pathology become too fragmented and lose control/distinctness as a specialty? • Planning the future - change is usually not sought out or embraced until pressures or incentives force it to happen (run the risk of being “too little, too late”) Additional Recommendations • All trainees would be expected to be competent in overlapping areas: laboratory management and administration, basic informatics, clinical consultation, regulatory and accreditation, molecular pathology, quality improvement, professionalism, interpersonal and communication skills, problem-solving/critical thinking skills, etc • Formation of a task force with representatives from key groups – ABPath, CAP, APC, PRODS, ASCP, ACGME/RRC, community pathologists, etc – to formulate a White Paper with a binding plan for recommendations and implementation References • • • • • • • • • Domen RE, Baccon J. Pathology residency training: time for a new paradigm. Hum Pathol 2014;45:1125-1129 Wells A, Smith BR. The goals of resident training in laboratory medicine in combined anatomic pathology/clinical pathology programs: an overview. Clin Lab Med 2007;27:229-240 Talbert ML, Ashwood ER, Brownlee NA, et al. Resident preparation for practice: a white paper from the College of American Pathologists and Association of Pathology Chairs. Arch Pathol Lab Med 2009;133:1139-1147 Peery TM. Horizons in pathology. JAMA 1959;171:2065-2068 Weinstein RS (chair), et al. Park City Report on Combined AP/CP Residency Training. October 1, 1988 Townsend JF, Van Peenen HJ, Senhauser DA, Lucas FV. The education of physicians for specialties in laboratory medicine. J Med Educ 1971;46:456-460 Horowitz RE. Expectations and essentials for the community practice of pathology. Hum Pathol 2006;37:969-973 Horowitz RE. The successful community hospital pathologist – what it takes. Hum Pathol 1998;29:211-214 Kass ME, Crawford JM, Bennett B, et al. Adequacy of pathology resident training for employment: a survey report from the Future of Pathology Task Group. Arch Pathol Lab Med 2007;131:545-555 References • • • • • • • • • • Otis CN. Residency training in anatomic pathology: looking forward in the 21st century. Hum Pathol 2006;37:929-931 Lagwinski N, Hunt JL. Fellowship trends of pathology residents. Arch Pathol Lab Med 2009;133:1431-1436 Gorstein F, Weinstein RS. Rethinking pathology residency training and education. Hum Pathol 2001;32:1-3 Frank K, Wagner J. ASCP Fellowship & Job Market Surveys: A Report on the 2014 RISE, FISE, FISHE, NPISE, PISE, and TMISE Surveys. www.ascp.org Editorial. Clinical pathology and modern medicine. JAMA 1932;99:1430-1431 Magath TB. The importance of clinical pathology to modern medicine. Science 1932;76(1972):333-336 Chemistry and its relation to medicine. The Lancet 1890;135(3466):260 Dreschfield J. The relations of pathology and its study. Br Med J 1886;2(1337):323-326 Approved examining boards in medical specialties: American Board of Pathology. JAMA 1940;9(115):737-738 Post MD, Johnson K, Brissette MD, Conran RM Domen RE, et al. Employer expectations for newly trained pathologists: report of a survey from the Graduate Medical Education Committee of the College of American Pathologists. (manuscript submitted for publication) References • • • • • • • • • • • Wells A, Smith BR. The challenge of training pathologists in the 21st century. Hum Pathol 2006;37:932-933 Sanford AH. The role of the clinical pathologist. JAMA 1930;95(20):1465-1467 Alter NM. The functions of the full time pathologist in hospitals. JAMA 1934;103(16):1189-1192 Blumer G. Pathology and practice. JAMA 1935;105(17):1311-1312 Wahl HR. The responsibility of the pathologist. JAMA 1928;91(7):441-443 Wood FC. The relation of pathology to practice. JAMA 1919;73(8):569-570 Bishop LF. The relation of clinical pathology to actual practice. Boston Med Surg J 1905;153(25):689-690 Shattuck FC. Specialism, the laboratory, and practical medicine. Boston Med Surg J 1897;136(25):613-617 Henderson Y. Clinical pathology – an opportunity and a duty. JAMA 1911;57(11):857-859 Lynch KM. The specialist in pathologic anatomy. JAMA 1924;83(2):79-81 Foster WD. A Short History of Clinical Pathology. E & S Livingstone: Edinburgh and London; 1961.