Case Study 14
advertisement

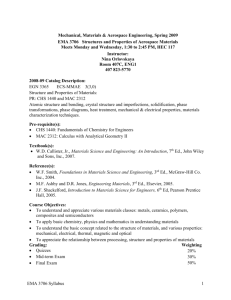
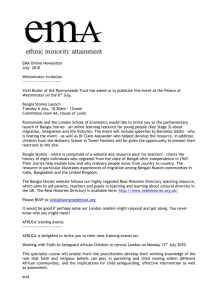
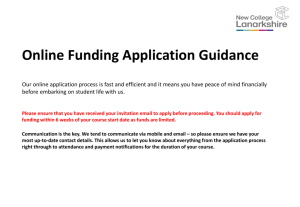
Case Study 14 Gabrielle Yeaney, M.D. Question 1 70-year-old man who complains of intermittent dizziness and unsteadiness for 1 week. Describe the MRI findings (location, enhancement, mass effect). MRI Sagittal T1 MRI axial FLAIR MRI axial T1 post contrast MRI Coronal T1 post contrast Answer The right posterior fossa (cerebellum) shows a wellcircumscribed homogeneously-enhancing duralbasedmass with extension through the tentorium to the right occipital lobe. There is some mass effect in the 4th ventricle and edema in the right cerebellar hemisphere. Question 2 Give your differential diagnosis for this dural-based mass. Answer Meningioma Hemangiopericytoma (HPC) Metastasis Secondary Lymphoma Other very rare entities: solitary fibrous tumor (some believe SFT may be the same as HPC but on one end of a morphologic spectrum); primary leptomeningeal melanocytoma (bright on T1, dark on T2); leiomyomatous and fibrohistiocytic tumors; synovial sarcoma Question 3 A right occipital and suboccipital craniectomy is performed and an intraoperative consult is requested. Describe the cytologic features of the touch prep and smear. Click here to view slides. Answer There are abundant dyshesive cells with uniform ovoid nuclei and scant cytoplasm. Nuclear outlines are smooth but occasionally indented. Nucleoli are inconspicuous. Mitotic figures are infrequent. There are no whorls. Question 4 What is your intraoperative diagnosis? (A. Neoplastic/Defer/Non-neoplastic, B. ______) Answer A. Neoplastic B. Atypical; Further classification would be difficult at this point but you could communicate a differential of atypical meningioma, hemangiopericytoma or some other mesenchymal neoplasm. Question 5 Review the permanent section of the morcellated specimen. Describe the histologic features. Click here to view slide. Answer This cellular lesion is arranged in sheets with a turbulent swirling pattern. There is little intervening stroma, but thin strands of eosinophilic collagen can be seen between the densely packed cells. A rare staghorn like vessel is present (black arrow). Mitotic figures are difficult to find. Question 6 What additional studies would you order to confirm your diagnosis? Answer Reticulin!!! IHC stains that may be helpful: CD34, factor XIIIa, bcl-2, CD99, smooth muscle markers, leu-7, EMA, vimentin (to access immunoviablility), Ki-67 Question 7 Interpret the reticulin stain and the following immunohistochemical stains. Click here to view slides. Answer Reticulin fibers are abundant and diffuse, surrounding individual tumor cells. Tumor cells diffusely express CD34, vimentin and CD99 but are negative for AE1/AE3. There is focal weak positivity for factor XIIIa and EMA. Ki-67 shows a tumor cell proliferation rate of 4%. Differentiating HPC from meningioma is a recurring challenge (nightmare?) for neuropathologists. The following data is from a study that compared 19 meningeal HPCs and 19 anaplastic meningiomas (MIIIs). IHC was performed by using EMA, CAM 5.2, CD99, Bcl-2, claudin-1 and Factor XIIIa (FXIIIa) antibodies. FISH was performed with NF2, 4.1B (DAL-1), chromosome 1p32, and 14q32 probes. HPCs showed strong CD99 (85% of cases), strong bcl-2 (86%), focal EMA (33%), focal claudin-1 (13%), and scattered individual cell FXIIIa (100%) positivity. Anaplastic meningiomas showed strong EMA (89%), strong claudin-1 (54%), weak or focal CD99 (15%), weak or focal bcl-2 (31%), and individual cell FXIIIa (84%) positivity. Focal CAM 5.2 expression was seen in 26% of HPCs and 15% of MIIIs. Deletions were extremely common in MIIIs: 1p (94%), 14q (67%), NF2 (100%), and 4.1B (67%). HPCs showed no 14q or 4.1B deletions, with 1 case each of 1p and NF2 deletions (6%). The sensitivities and specificities of the 3 most useful IHC markers (EMA, CD99, bcl-2) were 85%-89% and 67%-84%, respectively. Conclusions from the study were as follows: (1) EMA, CD99, bcl-2, and claudin-1 IHC and 1p, 14q, NF2, and 4.1B FISH are particularly useful for distinguishing anaplastic meningiomas from meningeal HPCs. (2) Focal EMA expression does not preclude a diagnosis of HPC. (3) The characteristic FXIIIa staining pattern reported for HPC also is encountered frequently in anaplastic meningiomas and therefore is nonspecific in this diagnostic setting. Rajaram V, Brat DJ, Perry A (2004) Anaplastic Meningioma Versus Meningeal Hemangiopericytoma: Immunohistochemical and Genetic Markers Human Pathology 35(11) Question 8 What is your final diagnosis? Answer Hemangiopericytoma—The meningeal hemangiopericytoma was first described in 1928 by Bailey et al., who considered the tumor an "angioblastic" variant of meningioma. HPCs are thought to be derived from pericytes. Question 9 What is the prognosis, standard treatment etc? Answer Despite their amenability to surgical enucleation, HPCs have a high local recurrence rate and propensity for late metastasis. 5-, 10- and 15-year survival rates have been quoted at 67%, 40%, and 23%, respectively. Favored metastatic sites are bone, liver, lung, CNS. Radiotherapy may improve survival. HPC can be subclassified into differentiated and anaplastic based on the presence of necrosis or brisk mitotic activity (>5/10 HPFs) and 2 or more of the following: hemorrhage, marked cytologic atypia, high cellularity. Ki-67/ MIB-1 indices vary from case to case, 1%-39% in one series with little relationship to outcome. Question 10 What is a pericyte? Answer Pericytes are specialized mesenchymal cells that are supportive to microvasculature. There is evidence that pericytes participate in vascular basement membrane synthesis, contraction and phagocytosis. Pericytes have been reported to act as oligopotential cells with the capacity to differentiate into adipocytes, osteoblasts and phagocytes when required. In addition, pericytes are considered to play a role in angiogenesis and antigen presentation.