Brain Function - Fragile X Ohio
advertisement

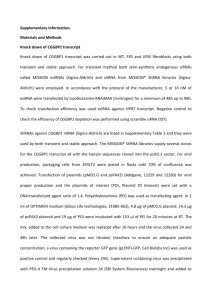
Research Progress in Fragile X Syndrome – Brain Function to New Ideas for Treatment Elizabeth Berry-Kravis MD PhD Rush University Medical Center, Chicago Disclosures: EBK has received funding from Neuropharm LTD and Seaside therapeutics to conduct clinical trials in FXS, and has served as a consultant for Novartis Pharmaceuticals and Roche Pharmaceuticals Fragile X Syndrome • Form of X-linked MR/ID discovered by Martin and Bell 1943 • Lubs fragile site 1969 • 1991 – Caused by mutations that inactivate FMR1 gene • Prevalence – 1:4000 males MOST COMMON KNOWN INHERITED and females FORM OF • Carriers – 1:100-250 COGNITIVE females, 1:250-800 males DISABILITY • All ethnic groups worldwide Features of Fragile X Syndrome • Physical: large prominent ears, long face, large head, prominent jaw and forehead, midfacial hypoplasia, hyperflexible joints, large testis • Intellectual Disability or LD • Behavior problems: anxiety, hyperactivity, distractibility, perseveration, aggression • Seizures – 15% • Strabismus – 30% • Medical: otitis, sinus, MVP, reflux, sleep apnea, loose stools, allergies FXS Intellectual Disability • Males - average adult IQ about 40 and mental age 5-6y, range severe ID to normal (mosaics) • IQ scores higher when young, decline with age • Specific cognitive profile • Achievement and Adaptive skills higher Fragile X Syndrome Characteristic cognitive pattern with prominent executive function deficits • Weaknesses • Strengths – Auditory processing – Receptive vocabulary – Sequencing – Syntax – Abstraction – Imitation – Short-term memory – Grammatical – Topic maintenance/ structure "connectedness" – Visual memory – Mathematics – Simultaneous – Working memory processing – Coordination/praxis – Experiential learning Why is Math so hard in FXS? FXS Developmental Problems • Motor delays in some • Hypotonia - orofacial when young • Fine motor problems poor writing ability • Gross motor clumsiness • Speech/language delays • Delayed imitative and symbolic play FXS Developmental Problems • Parents most frequently become concerned first about speech delay • Other concerns that may lead to child’s initial evaluation: – Motor delay – Extreme hypersenstivity/defensiveness – Hyperactivity or anxiety – Cognitive delays or LD at school age • Therapists for child with delay often first encourage testing – if parents don’t recognize magnitude of problem or doctors are discouraging testing FXS Developmental Problems • Most FXS patients can be identified with delay on developmental screens by 9-18 months • Average age of diagnosis still between 3-4 years – no change in past 10 years (Bailey) • Miss early intervention • New NFXF/FXCRC goal: diagnosis before age 2 – working on Pediatricians FXS - Pattern of Speech/Language Deficits • Most abnormal – Jargon/tangential language – “Jocular litanic phraseology” – Perseverative speech – Lack of use of gestures – Talking to self – Cluttering • Less abnormal – Fluency – Prosody • Strengths – Grammar – Vocabulary Language Characteristics in FXS Relative to Normal Mental-Age Matched Controls and Developmentally Delayed Subjects • Decreased intelligibility – Vowels sounds more variable than normal developmentally matched controls – Poor oromotor control – Faster rate of speech • Decreased length of utterances • Increased self-repetitious and perseverative language • Single word vocabulary a strength Language in FXS vs Autism • More impaired in non-verbal communication than autistic group • More impaired in expressive language • Less impaired in receptive language which is a strength • Tangential language more prevalent than in autism or general developmental delay (possibly due to anxiety, inhibitory control deficits) FXS Socialization Deficits Friendly but social anxiety • Good understanding of facial expression – different from typical autism • Deficits in peer entry • Defcits in interpreting social cues – correlate with anxiety, attention problems, social problems • Discrimination deficit - body language, hidden curriculum FXS - Female Affecteds • More mildly involved • Average IQ 80 • NVLD, VIQ>PIQ, poor math, very impaired executive function, distractibiity • Same cognitive pattern as males • Physical features/medical problems variably present • Social/psychiatric disability common – anxiety/shyness, oddness • Decreased education, job stability, socioeconomic status FXS Treatment in Clinic - Supportive Rush FXS Clinic since 1992 > 400 patients • Early intervention • Intensive speech therapy • OT with sensory integration • Inclusion in school as much as possible • Educational curriculum, environment, teaching style matched to FXS cognitive profile • Socialization program • Behavior plan • Behavior medications for ADD/anxiety • Aggressive tx of otitis – tubes/audiology • Manage sleep apnea • Yearly eye exams • Control seizures • Orthopedics if needed • Monitor for MVP/heart • Genetic counseling • Discuss reproductive options Psychopharmacology in Fragile X Syndrome • Targets behavior to improve functioning • Supportive, does not target underlying cognitive problem • Only one prior controlled trial in FXS (N=15) shows Ritalin effective in 2/3 of boys • Therapeutic decisions based on target largest problem symptom complex(es) – trial and error • May need to treat multiple behavioral domains Decision to Use Behavioral Medication • Individual engaging in dangerous behaviors • Individual is dysfunctional from behavior • Individual could accomplish more or be higher functioning if specific behavior is managed – Increase ability to participate – Able to be in more inclusive setting • Not necessarily “when all else fails” • ALWAYS an adjunct to behavioral, environmental measures FXS - Types of Medications and Indications* *meds may be targeting several clusters Problem Medication Behavior Cluster Class Medications Distractibility/ Hyperactivity Overarousal/ Hypersensitivity Anxiety/OCD/ Perseverative Mood Lability Stimulants Methylphenidate, Adderall, Provigil Alpha-agonists Clonidine, Tenex SSRIs Prosac, Zoloft, Celexa, Lexapro Antidepressants, AEDs, Lithium Atypical Antipsychotics, Tricyclics, Effexor, Li, SSRIs, VPA, TPX, CBZ Aggression/Self abusive Risperdal, Abilify, Seroquel, Geodon Abilify (aripiprazole) – New Mechanism • Partial agonist (activator) at dopamine D2 and serotonin 5HT1a receptors, antagonist at 5HT2a • May be particularly good in FXS because may help with ADHD symptoms (dopamine effect) as well as anxiety/irritability • Likewise can get aggravation of irritability, perseveration, agitation due to dopamine effect in subgroup • Social behaviors better in animal models compared to other antipsychotics • Thus far best antipsychotic response rate for FXS – can give dramatic social improvements Abilify – High Response Rate in FXS (2004-2007) Unknown 7% Abilify Responce <18 (n=43) Abilify Responce (n=64) Failed 30% Unknown 5% Failed 30% Successfully Treated 63% Abilify Responce >18 (n=21) Successfully Treated 65% Failed 29% Successfully Treated 71% Rush Fragile X Clinic: Supportive Psychopharmacology is Helpful in FXS… Berry-Kravis and Sumis, 2006 …but treating the underlying disorder would be better 208 trials 136 patients Attention Hyperactivity 52 trials 231 trials 100 trials 123 patients 58 patients 52 patients Anxiety Mood Aggression Irritability Hyperarousal Oversensitivity FMR1: The Fragile X Gene Normal X Chromosome Premutation (small size increase in FMR1) fragile X chromosome Full mutation (large size increase in FMR1) fragile X chromosome FMR1 mRNA FMR1 gene FMRP 12 - 50 CGG repeats FMR1 mRNA FMRP FMR1 gene 50 - 200 CGG repeats FMR1 gene blocked (methylated) CH3 CH3 200+ CGG repeats fragile site Simple DNA test to diagnose FXS – measures repeat size Carrier state passed through many generations before FXS No FMR1 mRNA Neural dysfunction Intellectual compromise Fragile X Syndrome No FMRP FMRP Expression and Disability 100 Social anxiety/shyness FMRP Distractibility/hyperactivity Executive deficits Spatial perceptual deficits NVLD Intellectual Disability 0 Disability The Fragile X Mouse (Knockout; K/O) • fmr1 gene inactivated • No active FMRP • Subtle cognitive problems • Audiogenic seizures • Good neurobiological model to answer question: WHAT DOES FMRP DO? Both FXS Mouse and Human Brains: Dendritic Spines are Abnormal in FXS with Immature Long Spines at Brian Connections FMRP regulates maturation of brain synapses (connections) McKinney et al, AJMG -B: Neuropsychiatric Genetics, 2005 FMRP in Dendrites (Brain Connections) FMRP in RED in tip of neural dendrites and where processes are forming •Antar et al, J. Neurosci 2004 FMRP regulates proteins made at brain connections (in dendrites) - proteins have to be made in right amount for connection to mature and work right. How loss of protein regulation causes weak connections in FXS glu LTD glu Excessive LTD – due to mGluR system overactivity AMPA AMPA AMPA mGluR AMPA mGluR FMRP ribosome ribosome AMPA AMPA FMRP Dendrite Normal Mature connection mGluR Theory of Fragile X Fragile X Immature connection (too weak) New Research is Leading to Future Treatments for Fragile X • Specific glutamate (group I mGluR) pathway regulated by fragile X protein (FMRP) in neurons • Regulates strength of neural connections needed for learning • Overactive when FMRP not there – messes up connections • Can block pathway with new drugs (mGluR blockers) being developed Normal Fragile X Drug glu AMPA 4 3 Other systems AMPA mGluR 1 X X 2 ribosome AMPA Potential Mechanisms for New Treatments of FXS AMPA Excessive LTD – due to mGluR system overactivity Dendrite Fragile X Immature connection (too weak) Targeted Treatments we have tried Ampakine Excessive LTD glu Stronger connection AMPA glu AMPA mGluR mGluR ribosome AMPA AMPA Activate AMPA receptors Raise BDNF – bring AMPA receptors to synapse Fragile X Immature connection (too weak) ribosome AMPA AMPA Ampakine Mechanism 3 Excessive LTD glu Stronger connection AMPA glu mGluR ribosome AMPA AMPA Fragile X Immature connection (too weak) Lithium blocks PI turnover, reduce mGluR signalling through PL-C/PK-C cascade, directly block protein synthesis by GSK3B block AMPA mGluR Li ribosome AMPA AMPA Lithium Mechanism 1 Lithium and FXS Models • Lithium corrects courtship memory deficits in dfxr mutant fly – McBride 2005 • Lithium corrects open field hyperactivity and decreases audiogenic seizures in fmr1 k/o mouse - Bauschwitz – FX-specific effect - lithium is convulsant in normals • Corrects several learning tests, LTD in mouse Li citrate dose titration 100 90 80 Data from R. Bauschwitz % total AGS 70 60 0 mg/kg 120 mg/kg 200 mg/kg 300 mg/kg 50 40 30 20 10 0 wt AGS wt SE FX AGS (FVB background) FX SE Audiogenic Seizures FXS Open-Label Lithium Trial Average Scores on ABC-C Subtests for Subjects with FXS During treatment with Lithium, n=11 • Test concept of mGluR pathway inhibition • 13 better at 2 mo, minimal toxicity 1 yr 70 Average ABC-C score 61.3 60 50 34.7 40 38.4 30 19.8 20 10 16 11.7 8.4 8.6 8 12.6 12.9 7 5.8 6.7 3.8 4.6 4.1 4.2 0 40 16 27 SD Stereotypy SD Hyperactivity SD Inappropriate 4.5 7.6 Speech SD 2.7 Baseline 2 Month Total SD 21.6 1 Year 12 -18 1 Group Mean Change -2 -5 -8 -20 -20 -25 -7 -22 10 8 8 7 6 -13 -15 -19 -40 Individual Change -44 -60 -67 ABC Total (range 0-174) 13 improved, p=0.005 Placebo change in CX516 study (N=25): -4 4 4 0 4 3 2 -2 -58 -80 Lethargy 6.6 14 20 0 Irritability SD 8.4 15 3 Group Mean Change Individual Change 0 4 -1 -2 -4 RBANS List Learning (range 0-40) 8 of 10 improved, p= 0.028 CX516 placebo change: 0.0 Also significant improvement in CGI, VAS, and Vineland Personal Daily Living Skills and Maladaptive Behavior Lithium Study Biomarker - ERK Activation in Lymphocytes ERK phosphorylation slower in K/O and FXS Berry-Kravis et al, JDBP 2008 6 N=11 Baseline mean: 4.87 min T1/2 Max Activation (Min) 5.5 5 2 Month Treatment mean: 4.11 min (p=0.007) 4.5 4 baseline (about 1 min is difference FXS and control) 3.5 3 2.5 2 mo 1 yr 2 1 Year Treatment mean: 3.56 min (P=0.00006) New Targeted Treatments in Trials - GABA Activators • Data from FXS animal models – GABA receptors abnormal – Glutamate toxic to fragile X fly, GABA activators rescue • Baclofen (available, used for spasticity) GABA-A agonist that blocks presynaptic release of glutamate – Can help irritability in FXS and autism – Reverses abnormal behaviors and seizures in FXS mouse – R form is much more active R-Baclofen and the mGluR Theory – Decrease Excessive Glutamatergic Transmission STX209 GABA-B Proteins Proteins FMRP Pre-synaptic Post -synaptic Mechanism 4 Clinical Trial of R-Baclofen (STX209) in FXS • Started in December • Goal is to show improves tantrums/aggression/agitation/irritability • Placebo-controlled crossover with 4 weeks of titrated treatment each arm • Tests before and after treatment each arm • Age 12 and up first 10 participants, now age 6 and up • Extension – can get drug after trial if it works • Good side effect profile • Have seen some positives during trial thus far New Targeted Treatments in Trials - mGluR5 Blockers • mGluR5 negative modulators = potent anxiolytics, also anticonvulsant • MPEP is prototype but not for humans • Being developed for anxiety disorders, neuropathic pain, irritable bowel • Like lithium, would correct mGluR overactivity in most areas of brain and would correct oversynthesis of all FMRPregulated proteins • Unlike lithium, specific for mGluR system Stronger connection Excessive LTD glu Ampakine glu AMPA AMPA mGluR mGluR5 blockermGluR Fenobam Li ribosome ribosome AMPA AMPA Fragile X Immature connection (too weak) Combination: Fragile X connection corrected AMPA AMPA mGluR5 Blocker Mechanism 1 AMPA Receptor Rescue by MPEP Nakamoto et al. 2007 FMRP Surface Internal AMPA AMPA Control FMRP Absent FMRP Absent and MPEP GluR1 = AMPA receptors that drive strength of neural connections ALL ABNORMAL Phenotypes Tested in Fragile X Fly Normalized by MPEP • Courtship memory deficits McBride et al. 2005 • Mushroom body beta lobe fusion • Lack of survival on commercial food (glutamate-containing) Warren 2006 • Odor shock long-term memory deficits Bolduc 2007 ALL ABNORMAL Phenotypes in FXS Mouse Normalized by MPEP (or Other mGluR5 Blockers) Audiogenic seizures Epileptiform bursts Open field behavior Prepulse inhibition Dendritic spine shape AMPA receptor internalization Excessive protein synthesis These and other phenotypes in the fmr1 K/O mouse also all reversed by crossing fmr1 K/O to mGluR5 heterozygous mutant Bauschwitz, 2006 Vehicle n=5 100 % status epilepticus • • • • • • • SE107 80 n=6 60 40 n = 13 n = 10 20 0 FVB KO Hybrid KO Wong et al. 2006 MPEP Controls Audiogenic Seizures in FXS Mouse WE CAN CURE THE FXS MOUSE! Video courtesy of R. Bauschwitz PhD But Mouse is not Man… human mouse Human brain a lot more wiring time mGluR5 Negative Modulators in Development for FXS • Fenobam – Old molecule – No major toxicity – Reduced anxiety in some adult phase II trials – Dropped - short half life/erratic pharmacokinetics (PK) – Found to be mGluR5 blocker (Porter et al. 2005) – 2008 – orphan drug status for FXS – Neuropharm – The first mGluR5 blocker used in FXS FENOBAM Open Label Escalating Single Dose Trial of Fenobam in FXS RUSH and UC Davis (Neuropharm and FRAXA) safety trial of 1 dose (50-150 mg), 12 adult FXS (6M, 6F), age 18-38, IQ 36-85 PPI improved 20% in 6/12 subjects (control test-retest group 2/13, p=0.03) Observation of positive behavioral changes in 9/12 subjects No fenobam-related adverse events Prepulse Inhibition (PPI) Studies 50 ms 105 db white noise Startle Alone Trials Auditory stimulus Latency Amplitude (volts) Obicularis Oculi EMG Prepulse Trials 50 ms 105 db white noise Prepulse: 50 ms, 75 db 1000Hz tone Auditory stimuli Prepulse interval: 60, 120, or 240 ms Obicularis Oculi EMG Amplitude (volts) Prepulse Inhibition in Fragile X Syndrome: Outcome Measure Ready for Treatment Trials Hessl et al. AJMG 2008 Test-Retest Reliability Group Effect: F(1, 74) = 36.00, p < 0.000001 !! Alphas = .88 (control), .85 (FXS), .89 overall!!! PPI improved on fenobam Berry-Kravis et al. JMG 2009 P=0.03 mGluR5 Negative Modulators in Development for FXS • STX107 – Seaside (from Merck) – Good safety profile, twice daily dosing – In Phase I - FXS trials projected in 2010 • AFQ056 – Novartis – Good safety, twice daily dosing – Randomized double-blind 28 day clinical trial in Europe just finished – 30 males with FXS – Test behavior and cognitive measures – New trial planned in Europe • Other companies developing for other conditions (Addex, AstraZeneca) mGluR5 Negative Modulators in Development for FXS • RO4917523 – Roche – Once daily dosing, good safety – Starts Phase II trial in USA November 2009 – Placebo controlled 6 week treatment – 60 males or females with FXS age 18 up – Cognitive, behavior measures, eye tracking, PPI – Lots of blood monitoring for PK • 2 Phases - dose finding and max dose • If safe and appears successful will extend to 6-17 age group Potential Other Future TRIALS • Minocycline – Mechanism 2 • Better ampakines – Mechanism 3 • Multicenter Abilify trial for FXS approval • PAK inhibitors • Combinations Still need work on design and outcome measures for these, many steps, but benefit may be overlap with autism pathways – treatments for autism too Minocycline • Works on MMP9 – one of proteins regulated by FMRP • Too much MMP9 in FXS • Minocycline inhibits the activity of the excess MMP9 • Normalizes spines and some behaviors in FXS mouse • Anitibiotic used for zits – available now – Causes teeth to turn yellow if used before age 10 – Trial in Canada – Lots of use in USA – variable positives and negatives – hard to interpret definitively – Big trial planned through FXCRC • Only affects one FMRP protein target so might need to use with other things New Measures of Function “Outcome Measures” for Clinical Trials Alertness KiTAP Test - Many subtests reliable in test-retest – will use in Roche study - Correlates with attention and hyperactivity measures - Crosses all levels Go-no Go Flexibility Eye Tracker as New Outcome Measure Validated this summer with test-retest to be ready for Roche mGluR trial in Fall – measures eye contact NIH Study Shows Increased Rates of Cerebral Protein Synthesis in Fragile X Knockout Mice WT KO Qin et al (2005) J Neurosci 25:5087. Current NIH Study to Prove Increased Protein Synthesis in Humans with FXS • • • • PET scans with anesthesia FXS males over 18 years All expenses paid to Washington No medications (or if on stimulants can stop for day of study) • Will be very helpful in proving the mGluR theory in humans and supporting the new medication development • Can be used to show the new meds work Testing for FXS Modifiers and Biomarkers Many proteins in this pathway may be implicated in autism Making Stem Cells from Skin Cells (iPS) …and brain cells from the stem cells for personal brain cell cultures to study treatment targets in different people with FXS Newborn Screening for Fragile X Comes to 7th Grade Pilot study on newborn screening for FMR1 mutations using blood spots: a) Identification of the frequencies and the allele size distribution of the FMR1 premutation and full mutation alleles Assessment of the severity of clinical involvement during early development for newborn probands with premutation and full mutation alleles To document the degree of clinical involvement of the wide variety of fragile X-related phenotypes in the extended family of the newborn proband identified by newborn screening. a) The CGG linker protocol allows the detection of expanded alleles in both males and females c f CGG repeat 1 5 2 Lane 3 4 b) (GCC)n c f CGG repeat Consent forms and information sheets approved by IRBs and being presented to each mother delivering a baby at Rush (Chicago) and UC Davis (Sacramento) since October 1, 2008 Sacramento and Chicago: 2000 blood spots collected Newborn Screening for FXS Pilot program (30,000 births) in California, Illinois • Need follow up for positives with early intervention and genetic counseling at FXS clinic • Benefits – – – – in early intervention right away avoid long process of diagnosis, extra tests avoid second (or third) affected child get diagnosis for symptomatic premutation carriers through cascade analysis of family • Problems – what to do with asymptomatic premutation carriers – no cure • If new treatments give partial “cure” – newborn screening will be key (treatments may work better earlier) Pilot FXS Newborn Screening • Will address epidemiology issues (eg. mutation frequencies) • Will address developmental questions (natural history of development and early intervention in pre and full mutation carriers) • Will address whether screening and diagnosis is helpful or not for families FXCRC Registry and Database • National Registry to find people who want to be involved in research and clinical trials – going up Fall 2009 • Database on participants with FXS entered to answer important questions about the disorder – hopefully up Summer 2010 • Enroll at any FXS Clinic – OHIO Clinic • De-identified at national level – names of participants kept at Fragile X Clinics • Can specify types of research can do • Need to sign consent for each person entered • For registry: one page form to fill out for each person – self and relative forms Acknowledgements • FRAXA Research Foundation • NIH – NINDS • Kiwanis Spastic Paralysis Foundation • National Fragile X Foundation • – • • Sue Ellen Krause PhD Sandy Block MS Steve Guter MS Ed Cook MD Randi Hagerman MD Maureen Leehey MD Paul Hagerman MD PhD Chris Goetz MD Don Bailey PhD Glenn Stebbins PhD Pete Van der Klish PhD • FXS Families Kristina Potanos Dahlia Weinberg Rebecca Lara Foster Lewin Allison Sumis Crystal Hervey Students – – – – Steve Porges PhD Mina Johnson PhD Isabel Boutet PhD • Steve Hooper PhD Ivan Jean Weiler PhD Bill Greenough PhD • Ning Weng PhD Mark Bear PhD Emily Osterweil PhD • Lili Zhou MD Study Co-ordinators – – – – – – • Collaborators – – – – – – – – – – – Lab Research Associate Ok-Kyung Kim Chinton DeSai Ravi Iyengar Hazel Perry Statistics – – Sue Leurgans PhD Joanna Wuu MS Cortex Pharmaceuticals – – Steve Johnson PhD Roger Stoll PhD Seaside Pharmaceuticals – Randy Carpenter PhD Study Co-ordinators off site – – – Tristan Jardini Penelope Decle Jennifer Cogswell