HLC revision lecture
advertisement

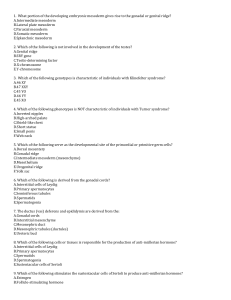
How to make a baby, or year 1 HLC in an hour Mark Chamberlain 21/5/09 how and why have sex? The key reason for sex is for the human species to procreate This requires •Intercourse or IVF •Fertilisation •Reproductive system MALE FEMALE GONADS Testes Ovaries INTERNAL DUCTS Efferent ducts Epididymis Vas Seminal vesicles Urethra Fallopian tubes Uterus Vagina EXTERNAL GENITALIA Penis Scrotum Vulva testis • • • housed in the scrotum spermatic cord leads to back of bladder, where it joins with seminal vesicles and leads into the ejaculatory duct, which opens into the prostatic urethra Consists of • seminiferous tubules - sperm production • Sertoli cells - maturation process • Leydig cells - production of testosterone ovaries • • • • • cortex - contains follicles with oocytes medulla - vascular area no duct system Contains developing follicles at varied stages At ovulation secondary oocyte (Graafian or vesicular follicle) (stopped in metaphase II) ruptures through ovarian wall, ovulated into pelvic cavity and is picked up by fimbrae of fallopian tubes and transported to uterus penile stimulation and erection Tactile stimulation → afferent fibres of pudendal nerve → spinal cord Thoughts from limbic system → efferent fibres → penis • parasympathetic via pelvic promotes • somatic via pudendal promotes • somatic via hypogastric suppresses Involves change from flaccidity → tumescence → erection Caused by ↑ parasympathetic activity to smooth muscle of pudendal artery, causing release of NO, stimulating ↑ cGMP to induce dilatation, leading to ↑ blood flow into the corpus cavernosum This counteracts the sympathetic-maintained myogenic tone Outflow of blood ↓ by compression of dorsal vein following ↑ in pressure Urethra protected from increased pressure by surrounding corpus spongiosum menstrual cycle Endometrium consists of 3 layers • stratum compactum • stratum spongiosum • stratum basale (basal layer) Cyclical events (~28 days) of menstruation and ovulation throughout a woman’s reproductive life UNLESS fertilization of a released ovum by a mature spermatozoon occurs USUALLY, this occurs following copulation (coitus) between man and woman BUT in vitro fertilization a reality ovulation GnRH acts on anterior pituitary to cause release of: • • FSH – stimulates maturation of follicle LH – stimulates ovulation at day 14 (leading to oocyte completing Meiosis I, stopping in Meiosis II at metaphase) Male germ cell = spermatozoa Female germ cell – 2o oocyte Meiosis - haploid chromosome # Fertilisation - diploid chromosome # Maternal and paternal chromosomes are the blueprint for new individual fertilisation • • • • • Takes place in fallopian tubes at the distal end of the ampulla Sperm capacitation needed before Sperm binds to the ZP3 receptor Sperm penetrates the several egg coats using the acrosome reaction Cortical reaction prevents multiple sperm entry Fertilisation causes oocyte to complete Meiosis II; restores diploid number of chromosomes; determines sex post fertilisation Takes 9 months (40wks) for a human baby to develop • 1st Trimester - most important as this is when body forms: • Weeks 1-2 Blastocyst stage • Weeks 3-8 Embryonic stage (Organogenetic period) • Weeks 9-onwards Fetal stage • • 2nd Trimester - rapid growth of fetus 3rd Trimester - fat production - zygote travels down fallopian tube - first division at approximately 30h - sheds zona pellucida and implants - hCG production initially from corpus luteum Days 1-6 twins ectopic pregnancy developmental abnormalities • Can arise at different levels: • Chromosone • Genetic • (Environment) • • • Chromosomal and genetic effects account for majority of losses of pregnancies or abnormalities in first few weeks – which often go unrecognised May be numerical or structural. 50% of conceptions end in abortion - 50% of these due to chromosomal abnormality.T hus, 25% of conceptuses have a chromosomal defect. Chromosomal abnormalities account for 7% of major birth defects. • • • • Downs syndrome(trisomy 21) Turner syndrome (45, X0) Patau Syndrome (trisomy 13) cri-du-chat (chr 5 partial loss) developmental abnormalities • Genetic accounts for 8% of major birth defects • • • • • vascular formation (lethal), holoprosencephaly (lethal) cleft lip Polydactyly Environmental influences have a major impact/influence on patterning and growth events in later development, less so on very early development • • • • • lack of Folic acid in diet alcohol abuse drug use Radiation viruses eg: Rubella teratogens implantation • • • Contact between maternal and fetal systems is dynamic Invasion of syncytiotrophoblast then cytotrophoblast causes vascular remodelling and the fetomaternal interface Point of contact is the placental villi and the placental spiral arteries Day 9 - invasion Day 13 – lacunae formation bilaminar disc @ day 9 gastrulation • • First stage of folding starts with gastrulation Primitive streak forms, setting up antero-posterior axis germ layer formation germ layers Germ layer organs ectoderm Skin, nervous system Mesoderm Skeleton, muscle, kidney, heart, blood endoderm Gut, liver, lungs notochord formation The notochord forms at the primitive node from invaginating epiblast cells, from around day 17, and extends cranially - forms the basis of the axial skeleton. -The notochord is involved in inducing the neural tube and somite formation neurolation • • • • Ectoderm is induced via notochord/mesoderm to become neuroectoderm Neuroectoderm gives rise to neural plate, neural groove and folds and ultimately to the neural tube Failure of this process leads to spina bifida Neurulation begins around day 19, and ends by day 27 with closure of posterior neuropore. body cavities • • • Cavities form in the preoral and lateral plate mesoderm these join to form a horseshoe-shaped space called the (intraembryonic) coelom. The coelom will develop into: • Pericardial cavity (cranially) • Pleural cavities (intermediate) • Peritoneal cavity (caudally) • The caudal ends open into the chorionic cavity (extraembryonic coelom) neural crest • • • arise from crest of the neural folds migrates from neuroectoderm into underlying mesoderm give rise to a whole host of tissues including: • • • • • connective tissue and bones of face & skull melanocytes glial cells and schwann cells cranial nerves odontoblasts somatogenesis • • form on either side of neural tube from paraxial mesoderm made up of 3 parts: • sclerotome - cartilage/tendon/vertebral column • myotome - muscle precursors • dermatome - skin precursors • • • first somite appears day 20 form anterior to posterior as the axis of embryo elongates by day 30 there will be 35 somites mesoderm • Intraembryonic • Paraxial mesoderm – somites • Intermediate mesoderm – urogenital • Lateral plate mesoderm - line body cavities and surround the organs • Extraembyonic • Body stalk - umbilical cord • Amnion, yolk sac, chorion Lateral folding • • • Axis elongates Lateral plate mesoderm develops a cavity (intraembryonic coelom) splits into two mesoderm layers • parietal (adjacent to ectoderm) lines body cavities and forms body wall • Visceral (adjacent to endoderm) forms gut wall • • • • Turns the embryo’s body into a cylinder instead of a sheet Rolls up the gut tube and nips it off from the yolk sac Cuts the intraembryonic coelom off from the chorionic cavity Means that the amniotic cavity surrounds the embryo except at the body stalk Head and tail • • • developing heart and pericardial sac (cranial coelom) tuck in ventrally gut tube pinches off from the yolk sac and narrows the body stalk Completion of the head-fold: • Forebrain now cranial to heart • Gut tube connected to yolk sac by a narrow stalk • Heart ventral to gut tube • Originally cranial part of coelom now ventral to intermediate parts (pericardial sac ventral to pleural sacs) Genetic regulation of development • All of the processes discussed are controlled by signals from genes. Complex gene interactions occur throughout development to form a normal fetus. • Example: Hox genes: • • • • • establish A-P axis, differences in the vertebrae, CNS divisions, pattern the limbs. One of the signals that control the activation of Hox genes is Retinoic acid, a derivative of Vitamin A. Developmental milestones • 1st Trimester • Wks1-2 Blastocyst stage – cell division/implantation • Wks 3-8 Embryonic stage – patterning and formation of organs/tissues • Wks 9- Fetal stage - growth • 2nd Trimester • Massive growth and development of fetus and maturation of internal organs. • Placental growth. • 3rd Trimester • Fat deposition • Movements • all patterning, organogenesis etc complete by 3 months; then ‘just’ growth of fetus Fetus in utero • • • • • • Higher vertebrates produce amniote eggs Complex system of cavities servicing the developing embryo Well wrapped up in membranes Floating in its own pond of amniotic fluid • Extraembryonic coelom develops from spaces in the trophoblast • Yolk sac – rudimentary apart from role in gut development • Chorion – gives rise to placenta • Chorionic cavity – obliterated early • Amniotic cavity – embryo floats in it, later tests its urinary and respiratory systems into it • Allantois – gives rise to part of urinary bladder • Allantoic mesoderm – gives rise to placental blood vessels Chorion and amnion eventually fuse, creating a chorioamnion and obliterating the chorionic cavity Amniocentesis may be used to test for fetal plasma protein (α-fetoprotein) in amniotic fluid – placenta • • • • • • A disc of fetal tissue Interface between maternal and fetal vascular systems Transporter Anchor Biosynthetic factory Immunological conundrum exchange • Products in: • Glucose, amino acids, lipids, oxygen • Peptides and proteins • Products (waste) out: • Carbon dioxide • Metabolites • Diffusion • Concentration gradient • Facilitated diffusion • • • Active transport Receptor-mediated Aqueous or lipid-specific immunoregulation • • Normally exposure of tissue to foreign antigens activates the immune response, leading to rejection within a few days or weeks. In pregnancy there is intimate contact between maternal and fetal tissues, with no evidence of any rejection separation • • Maternal blood and fetal blood never mix Pregnancy MAY be independent of the uterus - e.g. ectopic pregnancy biosynthesis • • • Hormones (pregnancy specific or general) Growth factors for placental development Cytokines to regulate feto-maternal interface Intermediate mesoderm Gives rise to most of the upper urinary and genital systems • Gives rise to Urogenital Ridge • Within which develops the nephrogenic cord • Source of most of UG system (except Primordial Germ Cells, lower urinary tract and perineum) Kidney differentiation • • • • • • sweeps cranio-caudally Cervical part (pronephros) never completes differentiation and regresses by wk 4 Thoraco-lumbar mesonephros differentiates but has mainly gone by wk 8 Mesonephric duct persists in male Sacral metanephros appears in wk 5 and becomes definitive kidney Ureter grows out from mesonephric duct Urinary bladder • The allantois is a hindgut outgrowth into the body stalk – gives rise to most of the bladder • The duct extending to the umbilicus normally closes but may persist and cause problems • The cloaca becomes partitioned into the urogenital sinus and the rectal sinus • Sometimes this is incomplete and a congenital fistula connects the urogenital and the alimentary tubes • • • The shared sections of the ureters and the mesonephric ducts (in the male) are absorbed into the back of the bladder The ureters now open into the bladder, the mesonephric ducts into the urethra Differential growth shifts the metanephric kidneys from their sacral site of origin to the posterior wall of the upper abdomen urinary maldevelopment • • Quite often a ureter may be completely or partially duplicated Less commonly a second ureter may be ectopic opening into the vagina, urethra or other organs instead of the bladder • One kidney may fail to reposition properly and so retains a sacro-pelvic position = pelvic kidney • If the kidneys are joined together, their ascent is prevented because they are trapped below the inferior mesenteric artery = a horseshoe kidney • • • The urogenital sinus and rectal sinus become separated by the uro-rectal septum At this stage the cloacal membrane still persists so that the urogenital and anal openings are closed. These subsequently open but may cause serious problems for the newborn child if this fails to happen • • • The gonads develop medially to the mesonephric kidneys Most of each mesonephros atrophies but the parts between the gonads and the mesonephric ducts persist These persistent mesonephric tubules will become the efferent ducts that connect the testis to the ductus deferens paramesonephric ducts • • • The paramesonephric (formerly called Mullerian) ducts develop in the most lateral part of the intermediate mesoderm in both sexes In males they play no important part in development In females they become the uterine tubes, uterus and upper vagina primordial germ cells • • PGCs are the cells that give rise to the eggs and sperms - the “germ line” is an expression describing this continuity of germ cells from generation to generation They arise from the yolk sac and in week 6 migrate via the hindgut and its mesentery to the genital ridges medial to the mesonephros • PGCs colonise the gonads: • They are the only cells that can become eggs or sperms • They are the only cells that can undergo meiotic (= reduction) division to form haploid cells • Unlike the somatic cells, a few of them survive to form the somatic tissues and PGCs of the next generation gonadal development • In both sexes, the gonads are derived from • Somatic mesenchymal tissues forming matrix • Primitive germ cells forming gametes • • • Gonads “indifferent” up to 6th week in utero Y chromosome then actively initiates formation of testes Otherwise undifferentiated gonads develop into ovaries the SRY gene • • • • Located on Y chromosome expressed in male Sertoli cells sry gene initiates formation of Sertoli cells sry gene expression • synthesis of a transcription protein - the SRY protein • • transcription factor regulating other gene activities other genes clearly involved in early gonadal development and sex determination SRY protein expression of Y chromosome (SRY gene) expression of X chromosome OVARIES TESTES Leydig cells Mullerian Inhibitory Hormone Mullerian (paramesonephric) Ducts Sertoli cells Female internal genitalia ANDROGENS External genitalia Wolffian (mesonephric) Ducts Male internal genitalia MALE FEMALE • • • The gonads develop medially to the mesonephric kidneys Most of each mesonephros atrophies but the parts between the gonads and the mesonephric ducts persist These persistent mesonephric tubules will become the efferent ducts that connect the testis to the ductus deferens Developing testes link up with the mesonephric duct though some persistent mesonephric tubules Mesonephric duct develops into the ductus deferens that will carry sperm to the male urethra Paramesonephric duct undergoes no further development • • During the 4th month the testes descend through the inguinal canal towards their final site in the scrotum Remember that the male genital duct system develops from the mesonephric duct and persisting mesonephric tubules • The accessory male genital glands (seminal vesicles and prostate) develop from buds from the lower end of the ductus deferens and from the urethra respectively • • Between week 8 and the 4th month the paramesonephric ducts link with each other and with the urogenital sinus to assemble the definitive female system The ovaries descend from their original upper lumbar location to the pelvis development of the external genitalia • Between the 3rd and 6th weeks the external genitalia develop in the same indifferent form in embryos of both sexes • • • In the absence of androgens the indifferent form progressively develops into the definitive female pattern The urethral folds and genital swelling form the labia minor and majora The urethra opens into the vestibule posterior to the clitoris • • • • Androgen stimulation in the male stimulates: Expansion of the phallus Fusion of the urethral folds to enclose the penile urethra – incomplete in hypospadias Expansion and fusion of the genital swellings to form the scrotum any questions?