Document
advertisement

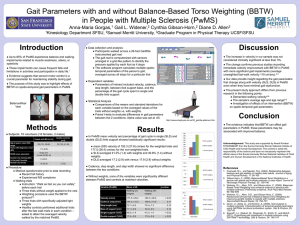
Fall Reduction during the Sensory Organization Test with and without BalanceBased Torso-Weighting in People with Multiple Sclerosis Gail L 1Samuel Introduction • Several recent studies have found that people with multiple sclerosis (PwMS) fall frequently.1-3 • Impairments in sensory systems or motor control systems that affect balance may result in falls.4 • Balance-based torso weighting (BBTW) has proven effective in improving static balance,5 but the impact on falling is unknown. • The sensory organization test objectively measures the contribution of sensory system to postural control • The purpose of this study was to investigate the effects of BBTW on balance and fall frequency recorded by the sensory organization test (SOT) in PwMS and healthy age and bin matched control participants. Merritt 1 Horn, Cynthia 2 University, Graduate 1 Gibson-Horn, Diane Methods Subjects: 60 PwMS with self-identified gait or balance problems, 10 bin-matched healthy controls Program in Physical Therapy UCSF/SFSU, CDP tests • Sensory organization test • Motor control test Sensory Organization Test (SOT) Healthy Controls n=10 Clinical tests • Timed up and go test • 25 Foot timed walk • Dynamic gait index Discussion Statistical Analysis • Comparisons of the means for each variable based on the averaged values of the trial without weights versus with weights • Paired t-tests to evaluate differences in gait parameters between the 2 conditions • Alpha value set at 0.05 PwMS (relapsing remitting, secondary and primary progressive) showed immediate statistically significant changes with weighting compared with no weight in: • SOT composite score • Equilibirum scores (trial 1 removed for NW) conditions 2-6 • Number of falls during SOT testing P value (Indep t-test, α=.05) CS NW Mean (SD) http://www.resourcesonbalance.com/neurocom/protocols/sensoryImpairment/SOT.aspx CS WT Mean (SD) PwMS showed immediate statistically significant changes with weighting compared with HC in: •SOT composite scores •Equilibirum scores (conditions 4-6) •Number of falls during SOT testing Averaged Equilibrium Scores Averaged Equilibrium Scores (ES) Trial 1 removed from prep=.048 weight condition ★p=.017 Two-tailed P value ★p=.022 ★p=0.022 Sex number male (%) Disease Steps mean (range) Self-report falls past 6 mon mean (SD) Weighting amount pounds (% body wt) 53.7 (12.1) 0.43 13.8 (8.4) 28 (17%) ★p=0.017 1.9 (1.3%) 59.7 (14.5) HC n=10 1 (10%) 73.9 (6.0) Two-tailed P value 0.0 1.1 (0.8%) 0.003 ★p<0.001 ★p=.004 *0.626 **0.001 ★p=0.004 ★p<.000 • BBTW shows promise for fall reduction in PwMS 70 ---- MSNW trials 2,3 60 MSWT trials 1-3 HCNW trials 2,3 50 HCWT trials 1-3 Acknowledgement: This study was supported by Award Number R15HD066397 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institutes of Child Health and Human Development or the National Institutes of Health. 40 30 20 10 60 References 0 1 2 3 4 5 6 SOT Conditions ★Significant difference MS NW/WT, α =0.05; Significant difference HC NW/WT, α =0.05 50 ★Significant difference MS NW/WT, α =0.05; Significant difference HC NW/WT, α =0.05 NW # falls (% total # trials) WT # falls (% total # trials) P value MS n=60 140 (19.4%) 91 (12.7%) *<0.001 HC n=10 3 (0.03%) 2 (0.02%) **0.484 40 Percentage Procedure • Informed consent explained and signed • Medical questionnaire prior to data recording • Order of testing (not randomized) • Computerized platform posturography (CDP) tests • Clinical tests (randomized) • BBTW weighting • Repeat CDP tests • Repeat clinical tests (same order as first time) • Impairment tests (not randomized) Conclusion 90 CS=composite score; NW=no weight; WT=weighted; MS=multiple sclerosis; HC=healthy controls; SD = standard deviation;* Dependent t-test; ** Independent t-test Indep = independent; SD = standard deviation; %=percent; mon=month; wt=weight 30 MS HC 20 10 0 ≤0 1 to 7 Future Research • Investigate if BBTW can reduce falls in people with MS living in the community. p=0.048 *<0.001 75.2 (9.5) **<0.001 • Composite scores were significantly improved for PwMS while weighted, over 64% changed 7 points or more • The SEM of the SOT calculated is lower for PwMS than Wrisley et al. minimal detectable change found for healthy young adults with repeated testing of the SOT over 2 weeks. • Even after removing the first SOT trial to reduced the learning effect, there was a significant reduction in falls and CS NW to WT in PwMS and MS to HC • These improvements occurred even when participants were fatigued due to lengthy testing • Number of falls for MS were significantly reduced with weighting during SOT; this did not happen in HC ★p<.000 ★p<0.001 80 2.6 (1-4) 1.8 (2.3) 50.5 (14.6) ES (percentage) Years with MS Mean (SD) 54.4 (11.1) MS n=60 Results • The standard error of the measurement was calculated to be 6.23 for the SOT for our population of 60 PwMS. 100 Age mean (SD) D. 2 Allen Results BBTW orthotic and weights People with MS n=60 1 Widener, Kristin ≥8 Change in Composite Score CS= composite score; NW=no weight; WT=weighted; MS=multiple sclerosis; HC=healthy controls; *Dependent t-test; ** Independent ttest 1.Peterson EW, Cho CC, Von Koch L, et al. Injurious falls among middle aged and older adults with multiple sclerosis. Arch Phys Med Rehabil. 2008;89:1031-1037 2.Cromwell, R.L., and Newton, R.A. (2004). Relationship between balance and gait stability in healthy older adults. Journal of Aging and Physical Activity, 11: 90-100 3.Widener, G.L., Allen, D.D., and Gibson-Horn, C. (2009). Randomized clinical trial of Balance-Based Torso Weighting for improving upright mobility in people with multiple sclerosis. Neurorehabil Neural Repair, 23: 784-791 4.Gibson-Horn, C. (2008). Balance-Based Torso Weighting in a person with ataxia and multiple sclerosis: A case report. Journal of Neurologic Physical Therapy, 32: 139-146 5.Widener, G.L., Allen, D.D., and Gibson-Horn, C. (2009). Balanced-Based Torso-Weighting may enhance balance in persons with multiple sclerosis: Preliminary evidence. Arch Phys Med Rehabil, 90: 602-609 6.Barthuly, AM, Bohannon RW (2011). Gait Speed is a responsive measure of physical performance for patients undergoing short-term rehabilitation. Gait & Posture, 10.1016/j.gaitpost.2012.01.002 7.Sosnoff, J.J., Weikert, M., Dlugonski, D., Smith, D., and Motl,R. (2011). Quantifying gait impairment in multiple sclerosis using GAITRiteTM technology. Gait & Posture, 34: 145-147 8.Givon, U., Zeilig, G., and Achiron, A. (2008). Gait analysis in multiple sclerosis: Characterization of temporal-spatial parameters using GAITRite functional ambulation system. Gait & Posture, 29: 138-14