THE NERVOUS SYSTEM
advertisement

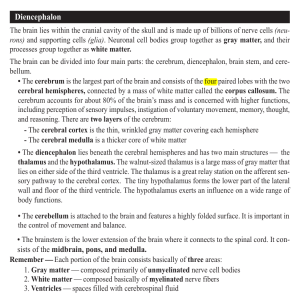
THE NERVOUS SYSTEM Divisions Central Peripheral Autonomic Sympathetic parasympathetic protected by the: skull vertebrae CSF- shock absorber and thus reduces the force of impact upon it Characteristics: color colorless, odorless spec gravity 1.007 occasional lymphocyte 1-3% mml protein 40 mg pressure 60-180 mmH2O total amount 125-150 ml traces of minerals and organic material of blood meninges dura mater arachnoid pia mater Brain CNS Cerebrum 2 hemispheres 4 lobes Cerebellum Brainstem Diencephalon mesencephalon rhombencephalon Spinal cord cerebrum 4 lobes frontal parietal taste and touch spatial orientation receives sensory impulses from the opposite side of the body with exception to special senses interpretation of pain, touch, temperature and pressure recognition of size and shape, weight, texture, consistency of object and the ability to distinguish two object between simultaneous skin contact temporal personality behavior and higher intellectual functions organization of thought body movement memories and emotions autonomic functions such as respiration, GIT, cardiovascular reactions and emotional responses contains auditory center important in understanding spoken words memory occipital visual area language CEREBELLUM located below the cerebrum receive information from all areas of the body aids in coordination of voluntary muscles, balance maintenance of muscle tone and maintain posture in space Brainstem interbrain or diencephalon thalamus- modifies and controls primitive emotional responses (pain, rage, love and hate) hypothalamus- where the pituitary body is attached; influence water, carbohydrate and fat metabolism, growth, sexual maturity, body temperature, pulse rate, blood pressure and sleep midbrain or mesencephalon- includes the RAS which control sleep, motor activity, consciousness and awareness hindbrain or rhombencephalon pons – bridge the gap structurally and functionally between hemispheres; primary motor pathway medulla oblongata- vital center for respiratory and cardiac function SPINAL CORD H-shaped gray matter (nerve cell bodies) surrounded by white matter (thousands of nerve fibers, descending motor and ascending sensory tracts) all outside spinal canal Contains long conducting pathways for the purpose as connecting link between brain and periphery such as skin and muscles PNS Cranial nerves Spinal nerves Peripheral nerves sensory (afferent) nerves- impulse to the brain motor (efferent) nerves- from brain down to the muscle mnemonics Sexy Secretary Make Money But My Brother Says Big Boobs Make More I. Olfactory II. Optic S= sensory III. Occulomotor M= motor IV. Trochlear B= both V. Trigeminal VI. Abducens VII. Facial VIII.Acoustic IX. Glossopharyngeal X. Vagus XI. Spinal accesory XII. Hypoglossal Spinal Nerves 31 segments 8 cervical 12 thoracic 5 lumbar 5 sacral 1 coccygeal Diagnostic Procedures ELECTROENCEPHALOGRAM (EEG) - records electrical activity of the brain - purpose: detect abnormalities that may be indicative of intracranial pathology or pathologic physiology determine existence and type of epilepsy nursing care: pretest: withhold sedatives, tranquilizers, stimulants for 2-3 days hair shampoo determine patient’s ability to lie still reassure patient that electric shock will not occur post test: remove electrode paste with acetone and shampoo hair LUMBAR PUNCTURE - introduction of hollow needle with stylet into the lumbar subarachnoid space of the spinal canal between L1/L5 and withdrawal of CSF for diagnostic and therapeutic purposes - purposes: measure CSF pressure (normal opening pressure 60-150 mmH2O obtain specimen for laboratory analysis check color of CSF and check for blood inject air, dye or drugs in the spinal canal - pretest: obtain consent determine patient’s ability to lie still in a flexed, lateral recumbent position have client empty bladder - post test: ensure labeling of CSF specimens keep client flat in bed for 12 hours force fluids assess neurologic status administer analgesics as prescribed check puncture site for bleeding or leakage assess sensation and movement in lower extremities monitor vital signs CISTERNAL PUNCTURE Introduction of a short-beveled hollow needle stylet in the median line below the occipital bone into the cisterna magna purpose: remove CSF when impossible to obtain in lumbar level potential complication: respiratory distress - nursing care: same as for lumbar puncture watch out for apnea, cyanosis and dyspnea X RAY OF THE SKULL - give radiographic picture of head and neck bones to reveal fractures, erosion of bone including size of sella turcica and configuration, density and vascular markings -nursing care: remove hairpins, glasses and hearing aids determine patient’s ability to lie still COMPUTED TOMOGRAPHY (CT) SCAN - used to identify brain abnormalities; produces a series of tomograms translated by a computer and displayed on monitor which represent cross sectional images of various layers of the brain; may be performed with or without dye - purpose: used to identify tumors of the brain and other lesions - nursing considerations: check allergy to iodine, seafood, dyes obtain consent inform patient of possible throat irritation and facial flushing if contrast die is injected MAGNETIC RESONANCE IMAGING (MRI) - use of magnetic and radiowaves to create a detailed visualization of brain and its structures - purpose: create a detailed visualization of brain and its structures - nursing considerations: be aware that patients with pacemakers, surgical or orthopedic clips, shrapnel should not be scanned remove jewelry or metal objects from patient determine patient’s ability to lie still administer sedation as required BRAIN SCANNING (RADIONUCLEIDE IMAGING STUDIES) - intravenous scanning of radioactive compound and the application of a scintillation scanner in the patient’s brain – there’s an increase uptake of radioactive compound at the site of pathology - purpose: detect intracranial masses, vascular lesions, infarct and hemorrhage - nursing considerations: check for allergy keep NPO 4-6 hours before the exam CEREBRAL ANGIOGRAM -injection of radiopaque substance into the cerebral circulation and visualization by means of X Ray - purpose: localization of tumors, abscesses, aneurysms, hematomas and occlusions - potential complications: anaphylactic reaction to dye, local hemorrhage, vasospasm, adverse intracranial pressure -pretest check for allergies to iodine take baseline assessment measure neck circumference NPO after midnight or clear liquid explain that warm flushed feeling and salty taste in mouth may be felt during the procedure - during and post test have emergency equipment available monitor neurologic status and vital signs or shock, LOC, hemiparesis, hemiplegia, and aphasia monitor swelling of neck and difficulty of breathing and swallowing administer ice collar / cap intermittently to relieve swelling and discomfort check insertion site fro bleeding and assess pulses distal to site maintain pressure dressing maintain bed rest until next morning as ordered force fluids if patient’s condition allows Electromyography (EMG) - uses electrodes to graphically record the electrical activity of muscle at rest and at contraction - nursing considerations: explain that patient must flex and relax the muscles during the procedure explain that discomfort might be felt but not pain administer analgesics after the procedure ENCEPHALOGRAM -visualization of the distribution of hydrogen molecules in the body in 3 dimensions - characteristics non invasive does not use harmful ionizing radiation superior imaging of body’s soft tissues - purpose differentiate types of tissues in normal and abnormal states clinical applications include: brain, both tumors and vascular abnormalities, cardiac and respiratory conditions, cardiac anomalies, blood vessels, liver disease, renal abnormalities, gall bladder - nursing care: remove all metallic objects and let patient lie on platform that will be moved into a table containing the magnet explain that nothing will be felt during the procedure but sound of magnetic coil as the magnetic field being pushed will be heard closely monitor client with potential respiratory or cardiac collapse VENTRICULOGRAPHY - introduction of air directly in the lateral ventricles by ventricular puncture thru opening made in the frontal, post, parietal or occipital regions for special X-ray study of brain - purpose to visualize ventricles, localize tumors - potential complications: headache nausea and vomiting meningitis increased intracranial pressure - nursing considerations: monitor vital signs check neurologic status elevate head of bed (15-20 degrees) PNEUMOENCEPHALOGRAPHY -introduction of air or oxygen into the subarachnoid space by lumbar or cisternal puncture to outline the ventricular system and intracranial subarachnoid space for special xray study - demonstrates intracranial subarachnoid space and ventricular system -purpose: localize intracranial lesion MYELOGRAPHY - injection of radiopaque dye by lumbar puncture followed by fluoroscopy - purpose: visualize subarachnoid space, spinal cord and vertebrae - pretest: obtain consent tell patient of possible throat irritation and facial flushing - post test: have patient flat on bed assess puncture site force fluids NEUROLOGIC ASSESSMENT LEVELS OF CONSCIOUSNESS orientation to time, place and person speech ability to follow commands, comprehension and action levels Hyperactive Conscious lethargy, drowsiness, obtundation Stupor Coma LEVELS OF CONSCIOUSNESS Mood Memory confabulation circumlocation Complex functions Reading Writing Abstract reasoning and speech VITAL SIGNS Respiratory Patterns Cheyne - Stokes Respiration Central Neurogenic Hyperventilation cluster of irregular breathing, irregularly followed by periods of apnea lesion in upper medulla and lower pons Ataxic Breathing prolonged inspiratory phase followed by a 2-3 sec pause pons dysfunction Cluster Breathing sustained rapid regular respirations (rate 25/min) with normal blood oxygen levels usually due to brainstem dysfunctions Apneustic Breathing regular rhythmic, altering between hyperventilation and apnea maybe caused by structural cerebral dysfunction of metabolic problems such as diabetic coma breathing pattern completely irregular, indicates damage to respiratory centers of the medulla Biots Respiration irregular and random deep and shallow breathing PUPILS affected pupil is usually on the same side (ipsilateral) as the brain lesion whereas the motor and sensory deficits are on the opposite side (contralateral) size, shape, equality of pupils reaction to light corneal reflex- blink reflex occulocephalic reflex (doll’s eyes)- present in patient with intact brainstem MOTOR FUNCTIONS muscle size muscle strength 5/5- normal full strength 4/5- muscle is able to move actively thru full ROM against gravity with weakness to applied resistance 3/5- muscle able to move actively against gravity alone 2/5- muscle able to move with support against gravity 1/5- muscle contraction is palpable and visible, trace or flicker of movement occurs 0/5- undetectable muscle tone- flabby or rigid muscle coordination – point to point maneuvers gait and station- stand still and walk in tandem SENSORY FUNCTIONS Pain touch Localization- pushes stimuli away Flexion- pulls away from stimuli Decorticate (abnormal flexion)- indicates damage to convex of brain Decerebrate (abnormal extension) – indicates damage to cerebellum No response- no visible movement to pain stimuli dysenthesia- localized irritating sensation, warmth, cold, itching, tickling, prickling, crawling, tingling paresthesia- distortions of sensory stimuli (light touch may be experienced as burning or painful) anesthesia- absent sense of touch hyposthesia- reduced sense of touch hyperthesia- overperception of touch hypalgesia- reduced sensation to pain hyperalgesia- increased sensation to pain analgesia- absence of pain perception heat and cold vibration REFLEXES papillary corneal biceps brachial triceps patellar Achilles plantar abdominal cremasteric anal gag CEREBRAL DYSFUNCTION aphasia- loss of language ability agnosia- inability to recognize objects (parietal lobe lesion) expressive- inability to send message (damaged Broca’s area) receptive- inability to perceive message (damaged posterior or temporal portion of dominant hemisphere) global- loss of all speech function visual tactile apraxia- loss of previously acquired ability to perform simple skills CEREBELLAR SYSTEM arms legs finger-nose test finger-finger test pronation-supination patting test heel-knee test heel-toe test trunk gait BRAINSTEM spontaneous motion of each eye occulocephalic reflex (Doll’s Eye) doll’s phenomenon- normal response if eyes move opposite to the direction of head turning occulovestibular test- done by slowly injecting ice water into the external auditory canal until eye deviation and nystagmus occurs implications: slow conjugate deviation of eyes towards the irrigated ear where they remain 30120 seconds is considered a response of comatose patient with intact brainstem abnormal movement such as skewing or jerky movement indicates brain stem lesion DISTURBANCES IN THE NERVOUS SYSTEM TRAUMATIC BRAIN INJURY (TBI) Traumatic Brain Injury (TBI) “Occurs as a result of an external force that produces a diminished or altered state of consciousness” (Iggy, p. 989) Can: Cause cognitive impairment Cause behavioral/emotional disturbances Be temporary or permanent Cause partial or total functional disability or psychosocial maladjustment Traumatic Brain Injury (TBI) Primary brain injury Two classifications: Open head injury Linear fracture Depressed fracture Open fracture Comminuted fracture Basilar skull fracture Penetrating injury Traumatic Brain injury Closed head injury Concussion Contusion Laceration Secondary brain injuries Any neurological damage that occurs after the initial injury TBI: Secondary Brain Injury Increased intracranial pressure (ICP) Hemorrhage Epidural hemorrhage Subdural hematoma Intracerebral hemorrhage Loss of autoregulation Hydrocephalus Herniation Epidural Hematoma Subdural Hematoma Subarachnoid Hemorrhage 1. Hematoma (accumulated blood) 1.Cerebrum 2.Skull 3.Cerebellum 4.Herniation of Brain into Spinal Column Increased Intracranial Pressure Description: Intracranial Pressure: The normal ICP depends on the position of the client and is 15 mmHg or less Increased ICP is more than 15 mmHg Untreated increased ICP can lead to displacement of the brain tissue The result of the amount of brain tissue, intracranial blood volume, and CSF within the skull at any time. Herniation Presents life – threatening situation because of pressure on vital structures in the brain stem, nerve tracts and cranial nerves Increased Intracranial Pressure Etiology: Head injury stroke inflammatory lesions brain tumor intracranial surgery any type of injury to the head may increase the ICP Cerebral edema Inflammation or abscesses Hemorrhage Increased Intracranial Pressure Pathophysiology: The only thing in the skull is brain tissue, blood and CSF If any abnormality occurs in the adult skull there is no room for expansion, which results in neurologic deficits because of the increased pressure in the closed cavity. The body compensate for this increased pressure or decompensate Compensatory mechanisms for maintaining ICP within normal limits include: Increased CSF absorption Shunting of blood to the spinal arachnoid space Decreased CSF production Failure of these compensatory mechanisms results in decompensation with the following sequence of events: Decreased cerebral blood flow with inadequate perfusion Increased PCO2 and decreased PO2 leading to hypoxia Vasodilation and cerebral edema Further increases in ICP ↑ ICP ↓ cerebral blood flow ↓ serum pH and ↑ CO2 cerebral vasodilation Edema ↑ ICP brain herniation irreversible brain damage death Increased Intracranial Pressure Clinical Manifestations: Earliest Signs: Headache Caused by the tension and displacement of pain sensitive structure such as intracerebral vessels (basal arteries, large venous sinuses and dura) Projectile vomiting Decreased LOC Progresses from restlessness to confusion and disorientation to lethargy and coma Recurrent and may be projectile Due to irritation of vagal nuclei in the floor of 4th ventricle Pupillary changes Unilateral dilatation of pupils which results from Truncal herniation and lateral brainstem compression Ipsilateral Same side dilation of pupil with sluggish reaction to light from compression of cranial nerve III Pupil eventually becomes fixed and dilated Papilledema Edema of the optic disc Increased in pressure thus optic disc becomes swollen and pushed forward above level of retina (Chorea disc) Increased Intracranial Pressure Changes in vital signs Maybe a late sign Decreased respiration Increased temperature Widening of pulse pressure Abnormal respiratory patterns Slow and bounding due to ischemia of Vasomotor center to medulla Increased blood pressure Increased pulse pressure Systolic blood pressure rises while diastolic pressure remains the same Due to compression of hypothalamus May also indicate other infection or dehydration Fever Increased metabolism in brain leads to increased oxygen consumption, which is detrimental to an ischemic and insulated brain. Decreased pulse Due to pressure and anoxia in respiratory center in medulla Cheyne – stoke respiration Motor abnormalities Contralateral Opposite side Hemiparesis from compression of corticospinal tracts Decorticate or Decerebrate rigidity Increased Intracranial Pressure Laboratory and Diagnostic Study findings: ICP monitoring reveals an ICP greater than 15 mmHg MRI scans, radiographs, and CT scans may identify the cause of the increased pressure Tumor, ischemic area Increased Intracranial Pressure Medical Management of Increased ICP Remove basic cause Drain a hematoma, treat if surgical removal is impossible use of temporary measures such as: Medications Promote diuresis thus decrease cerebral edema Furosemide (Lasix), Mannitol (Osmitrol) Mechanical decompression Removal of CSF or surgically providing for brain expansion. Nursing Management Maintain patent airway and adequate ventilation Limit suctioning to 15 minutes Produces hypocarbia Monitor vital sign and neuro check frequently to detect rises in ICP Maintain fluid balance: Position client with head of bed elevated to 30 to 45 degrees and neck in neutral position unless contraindicated Improves venous drainage from brain Prevent further increase in ICP Administer stool softeners and mild laxatives as ordered Nursing Management Administer antiemetics as ordered Prevent complications of immobility Administer medications as ordered Hyperosmotic agents Corticosteroids Phenytoin (Dilantin) To prevent seizures Analgesics for headache as needed Assist with ICP monitoring when indicated Furosemide (Lasix) To reduce cerebral edema Anticonvulsants Dexamethasone (Decadron) Anti-inflammatory effect reduces cerebral edema Diuretics Mannitol (Osmitrol) To reduce cerebral edema Monitor urine output every hour Normal ICP reading is 15 mm Hg Provide intensive nursing care for client treated with barbiturate therapy or administration of paralyzing agent Observe for hyperthermia secondary to hypothalamus damage DEGENERATIVE CONDITIONS Multiple Sclerosis Myasthenia Gravis Parkinson’s Disease Guillain Barre Syndrome Amyotrophic Lateral Sclerosis MULTIPLE SCLEROSIS Description: A progressively disabling demyelinating disease affecting nerve fibers of the brain and spinal cord Marked by periodic exacerbations and remissions Incidence is greater for women than men and is highest in temperate climate Age of onset is typically between 20 to 40 years old Etiology: Unknown cause Theories suggest that myelin damage is the primary event and that it results from a viral infection early in life that becomes apparent as a autoimmune process later in life It is believed that a defective immune response has a major role in the pathogenesis Pathophysiology: Produces patches of demyelination throughout the central nervous system The plaques in the involved area become Resulting in myelin being lost form the axis cylinders and degeneration of the axons themselves Sclerosed Interrupting the flow of nerve impulses Variety of manifestations depending on which nerves are affected Periodic an unpredictable exacerbations and remissions mark the course of MS Prognosis varies MS can cause rapid, sometimes fatal, disability, but about 70% of clients lead active, productive lives with long periods of remission 1. Nerve cell body 2. Axon with myelin sheath 3. Neuromuscular junctions 4. Muscle fibers Clinical Manifestations: Vary widely but may include: Visual problems Motor dysfunction such as: Diplopia Blurred vision Nystagmus Muscle weakness that typically worsens throughout the day Paralysis Spasticity Hyperreflexia Tremors Gait ataxia Fatigue Bladder or bowel incontinence Mental changes such as: Mood swings Irritability Depression Laboratory and Diagnostic Study findings: Lumbar puncture CSF analysis Reveal elevated CSF gamma globulins MRI Confirm the presence of demyelinating plaques Nursing management: Administer prescribed medications Which may include: Hormones such as corticotropin (ACTH) maybe prescribed to stimulate release of adrenal cortex hormones Corticosteroids Muscle relaxants Helps to improve nerve conduction Instruct the client to notify a physician if serious side effects such as: Fluid retention Muscle weakness Abdominal pain Headache Promote measures to avoid fatigue Assess the clients sleep and rest patterns Encourage adequate rest Assist the client in planning lifestyle modifications to decrease stress and fatigue and maximize functional abilities Encourage relaxation and coordination exercises to improve muscle efficiency Maximize functional abilities Assess the nature and degree of neuromuscular deficits and their effect on the client’s routine activities Prevent complications of immobility Promote self – care Maximize effective communication Encourage use of eye patch if Diplopia occurs Provide adequate care during exacerbations Provide measures to maintain adequate airway Provide client and family teaching Promote measure to enhance body image Promote client and family coping Help the client establish bladder and bowel control Prevent and treat muscle spasticity Maybe compromised because of the chronic, progressive disease process Provide referrals PARKINSON’S DISEASE Description: A progressive neurologic disorder resulting from degeneration of basal ganglia in the cerebrum The second most common neurologic disorder in the elderly Affects about 1 of 100 persons older than 60 years The incidence is higher among men than women Etiology: Cause is unknown Predominantly idiopathic Suspected causes include: Viral infection Chemical toxicity Cerebrovascular disease Effects of such drugs as major tranquilizers Reserpine Methyldopa (Aldomet) Haloperidol (Haldol) Phenothiazines Pathophysiology: Dopamine, a neurotransmitter secreted by the basal ganglia, is essential to extra pyramidal function. Depletion of dopamine diminishes normal neuromuscular inhibiting mechanisms leading to the characteristic neurologic deficits associated with parkinsonism such as: Bradykinesia Muscle rigidity Resting tremor Progressive deterioration continues for about 10 years Death commonly results from pneumonia or another infection Clinical Manifestations: Most common initial symptoms: Rigidity: Cogwheel type Bradykinesia Tremor: mainly of the upper limb “Pill rolling” Resting tremor Slowness of movement Fatigue Stooped posture Shuffling, propulsive gait Difficulty rising from a sitting position Mask – like face with decreased blinking of eyes Quiet, monotone speech emotional lability, depression Increased salivation, drooling Cramped, small handwriting Autonomic symptoms: Excessive sweating Seborrhea Lacrimation Constipation Decreased sexual capacity Nursing management: Administer medication as ordered Levodopa (L – dopa) Increases level of dopamine in the brain relieves tremor, rigidity and bradykinesia Side effects: anorexia nausea and vomiting postural hypotension mental changes such as: confusion agitation hallucinations cardiac arrhythmias dyskinesia Contraindications: Narrow angle glaucoma clients taking MAOI Reserpine guanithidine methyldopa antipsychotics acute psychoses Be aware of any worsening of symptoms with prolonged high – dose therapy administer with food or snack to decrease GI irritation inform client that urine and sweat may be darkened Carbidopa – Levodopa (Sinemet) Amantadine (Symmetrel) prevents breakdown of dopamine in the periphery and causes fewer side effects used in mild cases or in combination with L – dopa to reduce rigidity, tremor and bradykinesia Anticholinergic drugs: benzotropine mesylate (Cogentin) procyclidine (Kemadrin) trihexphenidyl (Artane) Inhibit action of acetylcholine Used in mild cases or in combination with L – dopa Relieve tremor and rigidity Side effects: antihistamines: stimulates release of dopamine in the substantia nigra often employed when L – dopa loses effectiveness Eldepryl (Selegilene) diphenhydramine (benadryl) decrease tremor and anxiety side effect: drowsiness Bromocriptine (Parlodel) dry mouth blurred vision constipation urinary retention confusion hallucinations tachycardia MAO Inhibitor inhibits dopamine breakdown and slows progression of disease Tricyclic antidepressants given to treat depression commonly seen in Parkinson’s disease Provide safe environment Side rails on bed Rails and handlebars in toilet, bathtub and hallways No scatter rugs Hard – back or spring – loaded chair to make getting up easier Provide measures to increase mobility Physical therapy: Active and passive ROM exercises Stretching exercises Warm baths Assistive devices If client “freezes” suggest thinking of something to walk over Encourage independence in self – care activities: Alter clothing for ease in dressing Use assistive devices Do no rush client Improve communication abilities: Instruct client to practice reading aloud to listen to own voice enunciate each syllable clearly Refer for speech therapy when indicated Maintain adequate nutrition Cut food into bite – sized pieces Provide small, frequent feedings Allow sufficient time for meals, use warming tray Avoid constipation and maintain adequate bowel elimination Provide psychologic support to client/significant others depression is common due to changes in body image and self – concept Provide client teaching and discharge planning concerning: Nature of disease Use of prescribed medications and side effects Importance of daily exercise: Activities/methods to limit postural deformities: Walking swimming Gardening as tolerated Balanced activity and rest Firm of mattress with a small pillow Keep head and neck as erect as possible Use broad – based gait Raise feet while walking Promotion of active participation in self – care activities MYASTHENIA GRAVIS Description: A progressive disorder affecting neuromuscular transmission of impulses in voluntary muscles The incidence is 1 per 25,000 Higher among women than men Initial symptoms typically occur between the ages of 20 and 40 years old Etiology: Thought to result from an autoimmune response Pathophysiology: The acetylcholine receptor (ACHR) antibodies interfere with impulse transmission across myoneural junctions Causes abnormal weakness and fatigability of the skeletal muscle particularly of the eyes, face, jaw and neck may involve muscles of upper extremities and respiratory muscles The disorder follows an unpredictable course of periodic exacerbations and remissions Drug therapy allows many clients to lead normal lives Progressive weakness of respiratory muscles may cause life – threatening respiratory distress or myasthenic crisis Clinical Manifestations: Abnormal weakness of any striated muscle Particularly of the: Face Neck Arms hands Sever fatigue Drooping facial muscles and ptosis Diplopia Impaired chewing and swallowing Breathing difficulty because of weak respiratory muscles Laboratory and Diagnostic Study findings: Positive Tensilon test result confirms the diagnosis Tensilon Test: Description: Performed to diagnose myasthenia gravis and to differentiate between myasthenic and cholinergic crisis To diagnose myasthenia gravis: Tensilon injection is injected into the client Positive for myasthenia gravis: Client shows improvement in muscle strength after the administration of Tensilon Negative for myasthenia gravis: Client shows improvement in muscle strength and strength may even deteriorate after injection of Tensilon To differentiate crisis: Myasthenic Crisis: Tensilon is administered and if strength improves the client needs more medication Cholinergic Crisis: Tensilon is administered and if weakness is more severe, the client is overmedicated, administer Atropine Sulfate Serum anti – ACHR bodies are present Nursing management: Monitor Respiratory status and ability to cough Monitor respiratory failure Maintain suctioning and emergency equipment at the bedside Monitor vital signs Monitor speech and swallowing abilities to prevent aspiration Encourage client to sit up when eating Assess muscle status Instruct the client to conserve strength Plan short activities that coincide with times of maximal muscle strength Monitor for Myasthenic and cholinergic crisis Myasthenic Crisis Description: Assessment: Acute exacerbation of the disease Caused by a rapid, unrecognized progression of the disease, an inadequate amount of medication, infection, fatigue or stress Restlessness Weakness Dyspnea Dysphagia Difficulty speaking Implementation: Assess for signs of myasthenic crisis Increase anticholinesterase medications Cholinergic Crisis Description: Assessment: Depolarization of motor end plates Caused by overmedication with anticholinesterase Restlessness Weakness Dyspnea Dysphagia Nausea, vomiting and diarrhea Fasciculations Sweating Salivation Increased bronchial secretions Implementation: Hold anticholinesterase medications Prepare to administer the antidote Atropine sulfate if prescribed Administer prescribed medications May include anticholinesterase agents Action: Medications: Sweating Salivation Nausea Diarrhea and abdominal cramps Bradycardia Hypotension Implementation: Neostigmine bromide (Prostigmin) Pyridostigmine bromide (Mestinon, Regonol) Edrophonium chloride (Tensilon) Side effects: Increase the levels of acetylcholine at the myoneural junction Administer medications on time Administer 30 minutes before meals with milk and crackers to reduce gastrointestinal upsets Monitor and record muscle strength Note that excessive does lead to cholinergic crisis Instruct the client to avoid stress, infection, fatigue, and over the counter medications AMYOTROPHIC LATERAL SCLEROSIS (Lou Gehrig’s Disease) Description: A progressively debilitating and eventually fatal disease involving degeneration of motor neurons Affects 2 to 7 every 100,000 persons Affecting men more than women Onset typically occurs between the ages 40 and 70 years Etiology: Unknown Pathophysiology: ALS is marked by destruction mo motor cells in the anterior gray horns and pyramidal tract As motor neurons die, the muscle cells they supply undergo atrophic changes Upper and lower motor neurons are affected Progressive paralysis results Prognosis varies Most ALS clients die within 3 to 10 years of onset, usually from secondary causes such as pneumonia Clinical Manifestations: Vary with the location of affected motor neurons and disease stage and may include: Progressive weakness, atrophy, spasticity and tremors of the upper extremities, followed by involvement of lower extremities and then respiratory muscles Fatigue Impaired speech, chewing and swallowing Breathing difficulty Depression Laboratory and Diagnostic study findings: Electromyograpic (EMG) studies of the affected muscles indicate reduction in the number of functioning motor units Nursing Management: Because no treatment is available to slow disease progression, provide supportive care Maximize functional abilities Ensure adequate nutrition Prevent respiratory complications Encourage the client to verbalize feelings about body image and self – concept changes Promote client and family coping Provide explanations for the cause, treatment, and expected course of the neurologic disorder Promote measures to enhance body image Because the client typically experiences no cognitive deficits and retains mental abilities Provide client and family teaching Promote measures to maintain adequate airway Promote measures to enhance gas exchange such as oxygen therapy and ventilatory assistance Promote measures to prevent respiratory infection Provide intellectually stimulating activities Prevent complications of immobility Promote self – care Maximize effective communication Encourage the client and family to verbalize feelings and refer to appropriate resources as needed Provide referrals GUILLIAN – BARRE SYNDROME Description: An acute, rapidly progressing motor neuropathy involving segmental demyelination of nerve roots in the spinal cord and medulla Demyelination causes inflammation, leading to edema, nerve root compression, decreased nerve conduction and rapidly ascending paralysis Both sensory and motor impairment occur Also called Landry’s paralysis Etiology: A postinfectious polyneuritis of unknown origin that commonly follows febrile illness Pathophysiology: Segmental demyelination of peripheral nerves causes inflammation and degeneration in sensory and motor nerve roots Most clients experience spontaneous and complete recovery, although mild deficits may persist normal Damaged myelin neuron nerve Myelin sheath Clinical Manifestations: Progressive weakness and paralysis begin in the lower extremities and ascend bilaterally Paralysis ascends the body symmetrically Paralysis of respiratory muscles Cranial nerve involvement, most often facial nerve, produces difficulty talking and swallowing Loss of sensation and function of bowel and bladder Manifestations may progress rapidly over hours or may occur over 2 to 4 weeks Muscle atrophy is minimal Paralysis decreases as the client begins recovery; most often, there are no residual effects Partial or total paralysis Laboratory and diagnostic studies: Based primarily on the clinical manifestations Lumbar puncture and CSF analysis Checks for elevated protein concentration Electromyogram Treatment (Supportive) Respiratory support, possibly mechanical ventilation Corticosteroids Immunosuppressive and immunoglobulins Plasmapheresis: plasma exchange Nursing management: Goal is to evaluate progress of paralysis and initiate actions to prevent complications Evaluate rate of progress of paralysis; carefully assess changes in respiratory pattern Frequent evaluation of cough and swallow reflexes Remain with client while client is eating; have suction available Maintain NPO status if reflexes are involved If paralysis is rapid, prepare for endotracheal intubation and respiratory assistance Prevent complications of immobility during period of paralysis Assess for involvement of the ANS Orthostatic hypotension Hypertension Cardica dysrhythmias Urinary retention and paralytic ileus Goal is to prevent complications of hypoxia if respiratory muscles become involved Position client to maintain patent airway Elevate head of bed and may position on side as well Encourage coughing and deep breathing Suction client as needed and as indicated by amount of sputum and ability to cough Maintain adequate fluid intake to keep secretions liquified Encourage exercises and ambulation as indicated by condition Administer Oxygen if dyspnea is present Goal is to maintain psychological homeostasis Simple explanation of procedures Completer recovery is anticipated Provide psychological support during period of assisted ventilation Keep client and family aware of progress of disease ….. COGNITIVE IMPAIRMENT DISORDERS Alzheimer’s Diseases Multi – infarct dementia Description: CID are a group of chronic, progressive, organic mental disorders resulting in deterioration of the cognitive processes Most common are Alzheimer disease and Multi – infarct dementia Alzheimer disease accounts for more than 50% of dementias and affects 2% to 4% of persons older than age 65 Increases with age, particularly after age of 75 Multi – infarct dementia accounts for about 15% of cases of dementia Incidence is greater among men than women Onset generally is earlier than in Alzheimer's Disease Etiology: Alzheimer's Disease Cause is unknown Many theory exist such as: Toxic chemical excess Autoimmune mechanism Slow virus mechanism One or more faulty genes Multi – infarct Dementia results from Cerebrovascular disease producing multiple small cerebral infarctions Pathophysiology Alzheimer's Disease: chronic and irreversible disease characterized by specific neurologic and biochemical changes including: Neurofibrillary tangles, granulovacuolar degeneration of neurons ad senile or neuritic plaques primarily in the cerebral cortex Brain atrophy with widened cortical sulci and enlarged cerebral ventricles decreased acetylcholine production Multi – infarct Dementia Pathologic changes include multiple areas of extensive localized softening, along with various changes in cerebral vessels Clinical Manifestations: Alzheimer's disease Signs and symptoms are highly variable and may include: Early, subtle changes such as forgetfulness, recent memory loss and poor concentration, which the client maybe able to hide Later more overt signs of impaired cognition Severe memory loss and forgetfulness Inability to hold a conversation Think abstractly Formulate concepts Poor hygiene, grooming and inappropriate dress Inability to perform instrumental ADL’s Behavioral changes, such as Depression Anxiety Wandering Impulsive behavior Catastrophic reaction Imitation Emotional lability Withdrawal Clinical Manifestations: Multi – infarct dementia Dizziness, headaches Confusion Patchy memory loss Hallucinations Focal neurologic signs Muscle weakness Dysreflexia Dysarthria Laboratory and diagnostic study findings: CT scan Electroencephalography (EEG) Positron Emission Tomography (PET) useful in excluding: hematomas brain tumors stroke normal pressure hydrocephalus atrophy not reliable in make a definitive diagnosis of Alzheimer Disease Autopsy is the definitive diagnosis of Alzheimer Disease Nursing management: Administer prescribed medications Tacrine HCL (Cognex) - slows progression of Alzheimer's Disease by maintaining the availability of dopamine but have very toxic hepatic effects Provide initial and ongoing assessments Record the clients usual routine as well as words and behaviors used to communicate ADL needs Chart words and techniques that get “through” to the client Request that a family member or other person stay with the client if the client wanders or cannot be sent to diagnostic tests by himself Avoid sedation and restraints whenever possible Assign the client to a room that maximizes the potential for observation and is not next to an exit or stairwell For clients who are prone to wanderer Orient the client to the room and the unit Mark the room and bedside area with familiar belongings Attach an ID bracelet Alert others to wandering special clothing, care plan, posted notice Determine and obtain copy if the client has a Living Will or Durable Power of Attorney Maximize effective communication Use short sentences, simple words, gestures and written or pictorial cues, if needed explain and repeat instructions unless this increase distress Maintain a calm demeanor and a consistent approach Avoid excessive questioning and confrontation Break down instructions into simple components Support the anxious or depressed client Attempt to analyze behavior for meaning Maximize environmental safety Install alarms on stairwells Institute injury, fire and poisoning precautions Provide adequate lighting in all rooms Keep the bed in a low position or place the mattress on the floor Side rails may pose as a hazard Provide wanderer’s bracelet on the client Intervene as necessary to manage evening agitation “Sun – downing” - provide night light, soft music and supervision If indicated, create a limited – access, safe unit to obviate activity restriction and decrease the need for supervision Promote optimal functioning Fit diagnostic and therapeutic procedures into the client’s usual schedule as possible Assign consistent caregivers Establish a daily routine for care, maintaining the client’s pre-admission sleep – wake cycle if possible and desirable Provide a clock, calendar and daily schedule in the room Avoid pressuring the client for accuracy Prompt for ADLs with memory aids and verbal cues Encourage performance within the limits of ability Avoiding pressuring for performance Focus the client on simple, repetitive and purposeful activities with sequencing of skills Monitor for adverse effects of drug therapy Encourage ambulation and other exercise Encourage good grooming and personal hygiene Use distraction to alter undesirable behavior Noise People Caffeine Regularly assess the skin, gums, teeth and feet for breakdown and infection and provide good skin and mouth care Maximize opportunities for social interaction Optimize nutrition and fluid balance Break episodes of preservation or remove from harm Intervene as necessary an agitated client Limit stimuli may trigger catastrophic reactions Monitor food and fluid intake, noting; Optimize elimination Provide discharge planning SEIZURES Description: Convulsion Epilepsy Involuntary contraction of muscles resulting from abnormal cerebral stimulation Refers to paroxysmal, uncontrolled, excessive firing of hyperexcitable neurons in the brain Not a disease entity in itself but rather an indicator of underlying pathology TYPES Generalized Tonic – clonic (grand mal) Absence (petit mal) Partial Complex (temporal lobe; psychomotor) Status epilepticus Jacksonian ETIOLOGY About 50% of cases of epilepsy are idiopathic, for which no underlying pathology can be identified. Incidence higher in those with family history of idiopathic seizures Possible causes: Birth trauma Head trauma Brain tumor Meningitis, encephalitis or brain abscess Metabolic disorders E.g. Hypoglycemia Phenylketonuria Cerebrovascular disorders Pathophysiology: After a task is completed, nerve cell impulses should cease. Sometimes these nerve cell impulses continuing firing even after the task is finished. During the continued firing of nerve cell impulses, the parts of the body controlled by the errant cells may perform erratically These erratic physical movements are called seizures Seizures are classified as Partial arising from a localized area of the brain Generalized marked by widespread electrical abnormality in the brain e.g. complex, Jacksonian e.g. tonic – clonic, absence Status epilepticus refers to continued seizure activity a medical emergency treated with medications Clinical Manifestations Tonic – clonic seizures (grand mal) Tonic Clonic Involuntary contraction and relaxation of opposing muscle groups producing a jerky convulsive movements A generalized seizure activity, with no focal onset and lasting about 2 minutes Possible prodrome of a vaguely uneasy feeling (aura) Loss of consciousness, with falling if upright at onset Tonic phase Persistent contraction of a muscle or sets of muscles due to muscular shrinkage muscle contraction (including jaw clenching) possibly periods of apnea Clonic phase rhythmic, forceful movement of extremities excessive salivation rapid pulse Possible incontinence Stupor for 5 to 10 minutes after the clonic phase Absence seizures (petit mal) Generalized seizure activity no focal onset occurring primarily in children Momentary loss of consciousness (10 to 30 second) marked by a glassy stare usually no falling Complex seizures the client exhibits altered behavior e.g. automatisms, unusual sensations, delusions Not aware of what is happening Jacksonian seizures begin in one part of the body e.g. twitching of one side of the face or abnormal movements of the hand may progress to a generalized tonic – clonic seizures Status epilepticus Usually refers to generalized grand mal seizures Seizures is prolonged (or there are repeated seizures without regaining consciousness) Unresponsive to treatment Can result in decreased oxygen supply and possible cardiac arrest Medical management: Drug therapy Phenytoin (Dilantin) Often used with Phenobarbital for its potentiating effect Inhibits spread of electrical discharge Side effects: Phenobarbital gum hyperplasia hirsutism ataxia gastric distress Nystagmus anemia sedation Elevates the seizure threshold Inhibits the spread of electrical discharges Surgery: To remove the tumor, hematoma or epileptic focus Nursing management During seizure activity Protect from injury Keep airway open Prevent falling, gently support the head Decrease external stimuli do not restrain do not use tongue blades do not add additional stimuli loosen tight clothing Place in side – lying position Suction excess mucus Observe and record seizure Note pre-ictal aura affective signs: Fear anxiety Psychosensory signs: Hallucinations Cognitive signs: “deja – vu symptoms” note nature of ictal phase symmetry of movement response to stimuli; LOC respiratory pattern note post-ictal response amount of time it takes child to orient to time and place Provide client teaching and discharge planning concerning Care during a seizure Need to continue drug therapy Safety precautions/activity limitations Need to wear Medic – Alert identification bracelet or carry identification card Potential behavior changes and school problems Availability of support groups/community agencies How to assist child in explaining the disorders to peers CEREBROVASCULAR DISORDERS Cerebrovascular Accident TIA Cerebral Aneurysm Cerebrovascular Disorders • Destruction/infarction of brain cells caused by a reduction in cerebral blood flow and oxygen • Group of disorders that involves disruption of blood supply to the brain Cerebrovascular Accident (CVA, Stroke) Sudden loss of brain function Most common site is middle cerebral artery Most leading cause of death in the US which strikes 50,000 persons each year One half of survivors sustain permanent neurologic deficits Transient Ischemic Attacks (TIA) Transient or temporary episode of neurologic dysfunction Considered a warning sign of CVA Common site is bifurcation of common carotid artery Cerebral Aneurysm Dilation of the walls of the cerebral artery resulting from a weakness in the arterial wall Most common type of berry aneurysm Most common site is the circle of Willis Usually at a vessel at a junction Cerebrovascular Disorders Affects men more than women Caused by: Incidence increases with age Thrombosis Embolism Hemorrhage Risk Factors: Hypertension Diabetes mellitus Arteriosclerosis/atherosclerosis Cardiac disease Valvular disease/replacement Chronic atrial fibrillation Myocardial infarction Life – style: Obesity Smoking Inactivity Stress Use of oral contraceptives Etiology CVA TIA Results from Thrombosis Most common Embolism Vessel rapture Spasm Result from occlusion of an intracranial or extracranial artery Commonly associated with atherosclerosis CEREBRAL ANEURSYM Results from a weakness in a vessel wall because of a congenital defect or a degenerative process such as Hypertension Atherosclerosis Pathophysiology: Interruption of cerebral blood flow for 5 minutes or more causes death of neurons in affected area with irreversible loss of function Modifying Factors: Cerebral edema: Vasospasm: Develops around affected area causing further impairment Constriction of cerebral blood vessel may occur, causing further decrease in blood flow Collateral circulation: May help to maintain cerebral blood flow when there is compromise of main blood supply Stages of Development: TIA: Warning sign of impending CVA Brief period of neurologic deficit: May last less than 30 seconds, but not more than 24 hours with complete resolution symptoms Stroke in evolution: Visual loss Hemiparesis Slurred speech Aphasia Vertigo Progressive development of stroke symptoms over a period of hours or days Completed stroke: Neurologic deficit remains unchanged for a 2 to 3 day period Clinical Manifestations: Headache Generalized symptoms: Vomiting Seizures Confusion Disorientation Decreased LOC Nuchal rigidity Fever Hypertension Slow bounding pulse strong and forceful pulse Cheyne – stokes respiration Inability to flex the head forward due to rigidity of the neck muscles deepening breaths, followed by shallower and shallower breaths and stops breathing for a short period of time before starting to breathe again Focal signs: (related to site of infarction) Hemiplegia Sensory loss Aphasia Homonymous hemianopsia blindness or reduction in vision in one half of the visual field Laboratory and Diagnostic Study findings: CT and brain scan EEG: Reveal the lesion Abnormal changes Cerebral arteriography: May show occlusion or malformations of blood vessels Nursing Management: Acute Stage: Maintain patent airway and adequate ventilation Monitor vital signs and neuro checks Provide complete bed rest as ordered Maintain fluid and electrolyte balance and ensure adequate nutrition Maintain proper positioning and body alignment (elevate HOB) Promote optimum skin integrity Maintain adequate elimination Provide quiet, restful environment Establish means of communicating with client Administer medications as ordered: Hyperosmotic agents, corticosteroids to decrease cerebral edema Anticonvulsants to prevent or treat seizures Thromboembolytics given to dissolve clot Anticoagulants for stroke in evolution or embolic stroke Rule out the possibility of hemorrhage Tissue Plasminogen Activator (tPA, Alteplase) Streptokinase, urokinase Must be given within 2 hours of episode Rule out the possibility of hemorrhage Heparin Warfarin (Coumadin) For long term therapy Aspirin and Dipyridamole (Persantine) To inhibit platelet aggregation in treating TIA’s Anti-hypertensive if indicated for elevated blood pressure Nursing Management Rehabilitation: Hemiplegia Results from injury to cells in the cerebral motor cortex or to corticospinal tracts Causes contra-lateral hemiplegia since tracts cross in medulla Turn every 2 hours 20 minutes on affected side Use proper positioning and repositioning to prevent deformities Foot drop External rotation of hip Flexion of fingers Wrist drop Abduction of shoulder and arm Support paralyzed arm on pillow or use sling while out of bed to prevent sub-luxation of shoulder Elevate extremities to prevent dependent edema Provide active and passive ROM exercise every 4 hours Susceptibility to hazards Keep side rails up at all times Institute safety measures Inspect body parts frequently for signs of injury Dysphagia Check gag reflex before feeding client Maintain a calm, unhurried approach Place client in an upright position Place food in unaffected side of mouth Offer soft foods Give mouth care before and after meals Homonymous Hemianopsia Loss of half of each visual field Approach client on unaffected side Place personal belongings on unaffected side Gradually teach client to compensate by scanning Turning the head to see things on the affected side Emotional lability Mood swings, frustrations Create a quite restful environment with a reduction in excessive sensory stimuli Maintain a calm non-threatening manner Explain to family that the clients behavior is not purposeful Aphasia Most common in right hemiplegics Maybe receptive or expressive Receptive Aphasia Give simple slow directions Give one command at a time Gradually shift topics Use non-verbal communications Pantomime, demonstration Expressive Aphasia Listen and watch very carefully when the client attempts to speak Anticipate client’s needs to decrease frustration and feelings of helplessness Allow sufficient time for client to answer Sensory/Perceptual Deficits More common in left hemiplegics Characterized by: Assist with self – care Provide safety measures Initially arrange objects in environment on unaffected side Gradually teach client to take care of the affected side and to turn frequently and look at affected side Apraxia Loss of ability to perform purposeful, skilled acts Impulsiveness Unawareness of disabilities Visual neglect Neglect of affected side and visual space on affected side Guide client through intended movement Take object such as washcloth and guide client through movement of washing Keep repeating the movement Generalizations about the clients with left hemiplegia versus right hemiplegia and nursing care Left Hemiplegia Perceptual, sensory deficits, quick and impulsive behavior Use safety measures, verbal cues, simplicity in all areas of care Right Hemiplegia Speech – language deficits, slow and cautious behavior Use of pantomime and demonstration TIC DOULOUREUX (Trigeminal Neuralgia) Description: Disorder of cranial nerve V causing disabling and recurring attacks of severe pain along the sensory distribution of one or more branches of the trigeminal nerve Trigeminal neuralgia (TN), also known as tic douloureux pain syndrome recognizable by patient history alone. The condition is characterized by pain often accompanied by a brief facial spasm or tic. Pain distribution is unilateral and follows the sensory distribution of cranial nerve V, typically radiating to the maxillary (V2) or mandibular (V3) area. At times, both distributions are affected. Physical examination eliminates alternative diagnoses. Signs of cranial nerve dysfunction or other neurologic abnormality exclude the diagnosis of idiopathic TN and suggest that pain may be secondary to a structural lesion. Incidence increase in elderly women Cause unknown Etiology: The condition has no clear – cut cause Some experts argue that the syndrome is caused by traumatic damage to the nerve as it passes from the openings in the skull to the muscles and tissue of the face. The damage compresses the nerve, causing the nerve cell to shed the protective and conductive coating (demyelination) Others believe the cause stems from biochemical change in the nerve tissue itself A more recent notion is that an abnormal blood vessel compresses the nerve as it exits the brain In all cases, though, an excessive burst of nervous activity from a damaged nerve causes the painful attacks. Pathophysiology: The mechanism of pain production remains controversial. One theory suggests that peripheral injury or disease of the trigeminal nerve increases afferent firing in the nerve; failure of central inhibitory mechanisms may be involved as well. Pain is perceived when nociceptive neurons in a trigeminal nucleus involve thalamic relay neurons. Aneurysms, tumors, chronic meningeal inflammation, or other lesions may irritate trigeminal nerve roots along the pons. An abnormal vascular course of the superior cerebellar artery is often cited as the cause. In most cases, no lesion is identified, and the etiology is labeled idiopathic by default. Uncommonly, an area of demyelination from multiple sclerosis may be the precipitant. Lesions of the entry zone of the trigeminal roots within the pons may cause a similar pain syndrome. Thus, although TN typically is caused by a dysfunction in the peripheral nervous system (the roots or trigeminal nerve itself), a lesion within the central nervous system may rarely cause similar problems. Infrequently, adjacent dental fillings composed of dissimilar metals may trigger attacks. Clinical Manifestations: Sudden paroxysms of extremely severe shooting pain in one side of the face Attacks may be triggered by: During attack: cold breeze foods/fluids of extreme temperature Tooth brushing Chewing Talking Touching the face Twitching Grimacing Frequent blinking Tearing of the eye Poor eating and hygiene habits Withdrawal from interactions with others Laboratory and Diagnostic Study findings: Diagnostic X-rays Test: of the Skull Teeth Sinuses May identify dental or sinus infection which may aggravate the condition Medical management: Anticonvulsant drugs: Carbamazipine (tegretol) Phenytoin (dilantin) Nerve block: Injection of alcohol or phenol into one or more branches of the trigeminal nerve Temporary effect Last for 6 – 18 months Surgery: Peripheral Avulsion of peripheral branches of trigeminal nerve Intracranial Retrogasserian rhizotomy: Total severance of the sensory root of the trigeminal nerve intracranially Results in Permanent anesthesia Numbness Heaviness Stiffness in affected part Loss of corneal reflex Microsurgery: Uses more precise cutting and may preserve facial sensation and corneal reflex Percutaneous radio – frequency trigeminal gangliolysis: Current surgical procedure of choice Thermally destroys the trigeminal nerve in the area of the ganglion Provides permanent pain relief with preservation of: Sense of touch Proprioception a sensory nerve ending in muscles, tendons, and joints that provides a sense of the body’s position by responding to stimuli from within the body Corneal reflex Done under local anesthesia Microvascular decompression of trigeminal nerve: Decompresses the trigeminal nerve Craniotomy is necessary Provides permanent pain relief Preserves facial sensation Nursing management: Assess the characteristics o pain including triggering factors, trigger points and pain management techniques Administer medications as ordered, monitor response Maintain room at an even, moderate temperature, free from drafts Provide small, frequent feedings of lukewarm water and perform hygiene during periods when pain is decreased Prepare the client for surgery if indicated Provide client teaching and discharge planning concerning: Need to avoid outdoor activities during cold, windy or rainy weather Importance of good nutrition and hygiene Use of medications, side effects and signs of toxicity Specific instructions following surgery for residual effects of anesthesia and loss of corneal reflex Protective eye wear Chew on unaffected side only Avoid hot fluids or foods Mouth care after meals to remove particles Good oral hygiene; visit dentists every 6 months Protect the face during extremes of temperature BRAIN TUMORS Brain Tumors Primary tumors Secondary tumors Signs and symptoms Cerebral edema Increased ICP Focal neurologic deficits Obstruction of flow of CSF Brain Tumors: Complications Cerebral (vasogenic) edema/ ↑ ICP Herniation of brain tissue/ischemia of affected area Rupture/hemorrhage into brain tissue Seizure activity/hydrocephalus Pituitary dysfunctions/SIADH/diabetes insipidus Fluid and electrolyte imbalances Brain Tumor: Classification Malignant/benign Location Gliomas Meningiomas Pituitary gland Acoustic neuromas Brain Tumors: Symptoms Headaches (severe on awakening in am) Nausea and vomiting Visual symptoms Seizures Changes in mentation or personality Papilledema (swelling of the optic disk) Brain Tumors: Interventions Nonsurgical Radiation/chemotherapy Blood brain barrier disruption Recombinant DNA Monoclonal antibodies Antineoplastic drugs Immunotherapy/hyperthermia Surgical Biopsy Craniotomy Brain Tumors: Post-op Complications Increased ICP Hematomas Hydrocephalus Respiratory problems Neurogenic pulmonary edema Wound infection Meningitis Fluid/electrolyte imbalance