Chapter 17 Chapter 17 PowerPoint
advertisement

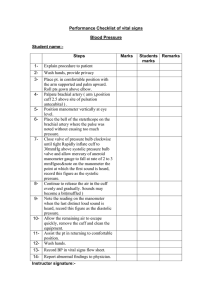
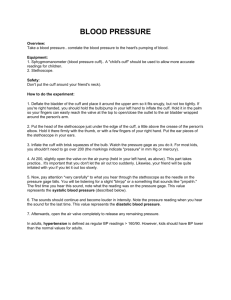
Chapter 17 BLOOD PRESSURE MEASUREMENT Sharon Jones Introduction This presentation is concerned with taking patients’ blood pressures and outlines the procedure as well as potential causes for error. Part 1 – Blood Pressure Overview Part 2 – Blood Pressure Measurement Part 3 – Blood Pressure Measurement Procedure Part 4 –Factors that Influence Blood Pressure PART 1: Blood Pressure Overview Definition Blood Pressure (BP) is the pressure exerted by the blood against the walls of the blood vessels (Tortora, 2006). Blood Pressure is dependent on: • strength of the heartbeat • elasticity of arterial walls • volume and viscosity of the blood • person’s health, age and physical condition Systolic and Diastolic Pressures Systolic Pressure • The peak pressure of the blood in the arteries caused by ventricular contraction. • Indication of the integrity of the heart, arteries and arterioles. Diastolic Pressure • The minimum pressure of the blood against the vessel wall following closure of the aortic valve. • Direct indication of blood vessel resistance. Korotkoff’s Sounds 1. Phase I The pressure level at which the first faint, clear tapping sounds are heard, which increase as the cuff is deflated (reference point for systolic BP). 2. Phase II During cuff deflation when a murmur or swishing sounds are heard. 3. Phase III The period during which sounds are crisper and increase in intensity. 4. Phase IV When a distinct, abrupt muffling of sound is heard. 5. Phase V The pressure level when the last sound is heard (reference point for diastolic BP). PART 2: Blood Pressure Measurement Measurement BP is recorded in millimetres of mercury: • mm Hg The systolic reading is written first, followed by the diastolic, for example: • 140/80 mm Hg Hypertension in adults is defined as a systolic pressure of more than 140 mm Hg Hypotension in adults is defined as a diastolic pressure of less than 100mm Hg Methods of Measurement Direct: intra-arterial recording. Invasive technique usually performed in areas where patients continually monitored, such as high dependency units and theatres. Indirect: more commonly performed. Measure the BP in the brachial artery of the arm. Indirect BP Measurement • Sphygmomanometer with stethoscope • Sphygmomanometer with Doppler • Sphygmomanometer with palpation • Dinamap or automated device PART 3: Blood Pressure Measurement Procedure Sphygmomanometer with stethoscope You will need: • Sphygmomanometer • Stethoscope • Observation chart Q. As you read through the action points in the next slide, work together in your learning groups to identify the rationale behind each step. You might want to refer back to the printed book for help. • Wash hands. • Explain procedure to the patient and assess level of understanding. • Ensure the patient is positioned comfortably, and has been rested for approximately 3 minutes if supine or seated and 1 minute if standing. • Remove tight clothing, support arm horizontally at heart level. • Avoid talking throughout the procedure. • Apply a sphygmomanometer cuff that covers approximately 80% of the circumference of the upper arm, with the centre of the bladder positioned over the line of the brachial artery approximately 2cm above the elbow. • Position the manometer at eye level, ensuring it can be easily observed by the practitioner. • Estimate the systolic pressure through palpation Estimation of the systolic pressure: • Palpate the brachial artery pulse • Inflate the cuff until the pulsation disappears. • Deflate cuff • Estimate systolic pressure • Inflate the cuff 30mm Hg higher than the estimated systolic pressure. • Position the stethoscope over the brachial artery, ensuring it does not come into contact with the tubing of the cuff. • Lower mercury column slowly (2mm per second), observe the needle of the dial as it is lowered and listen for Korotkoff sounds. • Read blood pressure to the nearest 2mm Hg. • Record the systolic and diastolic pressures, noting which arm was used, and compare to previous readings. Report irregularities to senior practitioner. • Remove the cuff and ensure patient’s comfort. • Clear away equipment and clean according to local policy. Cuff Size If a cuff is too large or too small, underestimation or overestimation of the BP occurs. • 12 x 26 cm standard adult size. • 12 x 40 cm obese adult size. • 10 x 18 cm small adult size. Monitors Two main types: • Auscultatory: use sound for measurement. • Oscillometric (automated): rely on variations of pressure in the cuff, caused by the pulse in the artery. Equipment Checks • Manometer: Visibility of meniscus; calibration • Cuff: Condition; length and width of inflatable bladder • Inflation/deflation device: Any malfunctions; control valve • Stethoscope: Condition & cleanliness PART 4: Factors that Influence Blood Pressure Factors that Influence the BP of Adults These include: • Age, anxiety, smoking, meals, time of day, temperature and sleep. • ‘White coat’ hypertension – blood pressure notably higher when recorded by doctors and nurses. (O’Brien et al, 1997) To minimise ‘white coat’ hypertension, try to relax your patient through familiarising them with their surroundings and using good communication skills. The healthcare practitioner responsible for undertaking BP measurement must ensure their practice is up-dated and their competence with this skill maintained to deliver safe, evidence based care at all times.