Algisyl
advertisement

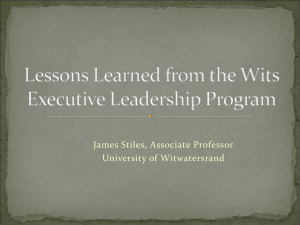
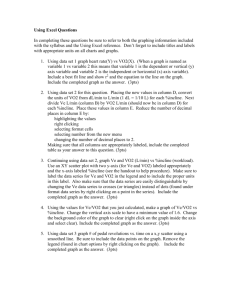
One Year Follow-Up Results from AUGMENT-HF: A Multicenter Randomized Controlled Clinical Trial of the Efficacy of Left Ventricular Augmentation with Algisyl-LVR in the Treatment of Heart Failure* Douglas L. Mann, Randall J. Lee, Andrew J.S. Coats, Gheorghe Neagoe, Dinu Dragomir, Enrico Pusineri, Massimo Piredda, Luca Bettari, Bridget-Anne Kirwan, Robert Dowling, Maurizio Volterrani, Scott D. Solomon, Hani N. Sabbah, Andy Hinson, Stefan D. Anker on behalf of the AUGMENT-HF Investigators * These data appear in European Journal of Heart Failure following this meeting Disclosures: Scientific Advisory Board - Lone Star Heart, miRagen therapeutics, Lilly Corporation Consultant – Bio Control Medical, Cardioxyl, Medtronic, Janssen Grant Support – NIH 1 Background • Therapeutic options are limited for patients with advanced heart failure who become refractory to conventional pharmacological therapies • The injection of biomaterials into diseased myocardium has been shown to reduce myofiber stress, LV wall stress, restore LV geometry and improve LV function1,2 • Algisyl® is a medical device that consists of an alginate hydrogel that is injected into the midwall of the LV, where it remains as a permanent implant that is intended to reduce LV wall stress and prevent or reverse the progression of HF • Results of the AUGMENT-HF 6-month primary endpoint analysis were presented at this meeting in 2014 and published earlier this summer3 1 Sabbah HN, et. al., JACC Heart Fail. 2013;1(3):252-8. Lee RJ, et. al, Int J Cardiol. 2015 Jul 2;199:18-24. 3 Anker, SD, et. al. Eur Heart J. 2015 Sep 7;36(34):2297-309 2 2 LV Restoration & Laplace’s Law The mechanism of the Algisyl R R h Dilated s = h Modified (LVR) PxR 2h s = PxR 2h 3 LV Restoration with Algisyl Placement of Alginate Hydrogel via a Limited Thoracotomy Mean procedure duration 80.5 (±24.9) minutes Mean number of implants 15.5 (±2.0) Mean total volume of Alginate-hydrogel 4.6 (±0.6) mL 4 AUGMENT-HF Study Design & Objectives • Multicenter prospective randomized clinical trial • 78 Patients with moderate to severe HF that had been treated with optimal medical and/or device therapy, randomized 1:1 − 40 patients randomized to Algisyl implant procedure + optimal standard medical therapy (SMT) − 38 patients randomized to optimal standard medical therapy alone • 15 centers in Australia, Italy, Romania, Netherlands & Germany • Primary Efficacy Endpoint: peak VO2 assessed by a blinded core lab at 6 months • Secondary Endpoints: peak VO2, 6MWT, Symptoms, QOL and measures of LV remodeling (echo) at 12, 18 and 24 months • Safety: clinical outcomes (MACE) adjudicated by blinded CEC 5 AUGMENT-HF Key Inclusion & Exclusion Criteria • Inclusion criteria − Written informed consent − ischemic or non-ischemic HF patients who are symptomatic despite optimal evidence-based therapies for HF − LVEF ≤ 35% − Peak VO2 of 9.0 - 14.5 mL/min/kg − LVEDDi 30 to 40mm/m2 (LVEDD/BSA) − Stable, evidence-based therapy for heart failure Previously reported high compliance: diuretics (99%) Beta Blockers (95%), ARBs/ACE-enzyme inhibitors (89%) and MRAs (69%) • Exclusion criteria − renal, hepatic, stroke and MI status − LV wall thickness < 8 mm required for implant 6 AUGMENT-HF Baseline Demographics Patients Completing 1-year follow-up All Patients (n=73)* All (n=59)** Control (n=33) Algisyl (n=26) 62.6 ± 9.6 63.2 ± 9.1 63.0 9.3 63.5 9.0 Ischaemic HF 42 (58%) 35 (59%) 20 (61%) 15 (58%) Non-ischaemic HF 31 (42%) 24 (41%) 13 (39%) 11 (42%) 81% 79% 76% 81% LVEF (%) 25.5 5.1 26.0 5.0 25.9 5.1 26.1 5.0 Peak VO2 (mL/min/kg) 12.2 1.8 12.4 1.7 12.4 1.7 12.3 1.8 6MWT distance (m) 293 84 292 88 306 81 275 95 Mitral regurgitation 3+ 37 (51%) 27 (46%) 18 (55%) 9 (35%) Hypertension 43 (59%) 37 (63%) 20 (61%) 17 (65%) Diabetes 29 (40%) 25 (42%) 15 (46%) 10 (39%) Previous PCI or CABG 20 (27%) 17 (29%) 9 (27%) 8 (31%) Age (years) NYHA Class III/IV * Modified Intention-to-Treat (mITT) population; ** 1 patient assessed by telephone only 7 Peak VO2 - Mean Change from Baseline (a) Peak VO2 (mL/min/kg) Mean change from baseline (SE) 2.5 P=0.014 P<0.001 2 1.5 1 0.5 0 -0.5 -1 -1.5 0 3 6 9 12 Time since randomisation (months) Control Algisyl # of available values Control 37 33 30 29 Algisyl 34 27 26 24 Algisyl was superior to SMT at 12 months with a mean treatment effect of 2.10 mL/kg/min (CI 0.96–3.24). Algisyl patients completed the 1 year follow-up with a mean peak VO2 of 14.0 (±3.1) mL/min/kg 8 Anaerobic Threshold – Mean Change from Baseline VO2 at AT (mL/min/kg) Mean change from baseline (SE) (b) 2.5 P=0.235 P<0.001 2 1.5 1 0.5 0 -0.5 -1 -1.5 -2 0 3 6 9 12 Time since randomisation (months) Control Algisyl # of available values Control 32 22 20 12 Algisyl 23 14 14 11 AT is independent of patient motivation or effort. Algisyl was superior to SMT with a mean treatment effect of 2.34 mL/kg/min (CI 1.35–3.32) at 12 months (p<0.001). 9 Post-hoc Analysis – Impact of Missing Peak VO2 Data • This is an advanced HF patient population with a high 1 year mortality, hence loss of patient data over this period is a concern. • Shown here is a post-hoc analysis of the repeated measures model for Peak VO2 including only paired data; those 58 patients with both a baseline and a 12 months assessment. 10 Six Minute Walk Test - Change from Baseline 6MWT Distance (m) Median change [25% - 75% range] 220 P<0.001* P<0.001* 180 140 100 60 20 -20 -60 0 3 6 9 12 Time since randomisation (months) Control Algisyl # of available values Control 38 34 34 31 Algisyl 35 29 29 26 Treatment effect (vs. SMT) of 101 meters for median 6MWT distance 11 NYHA Functional Class at 12 months 30 Control (n=32) Algisyl (n=26) Odds Ratio: 31.90 (CI 7.6–133.4); P < 0.001 25 No. of Patients 20 15 10 5 0 Control (n=32) Algisyl (n=26) Class I 0 8 Class II 8 14 Class III 24 4 Class IV 0 0 At 12 months, 85% of patients in the Algisyl group were NYHA functional class I or II compared to 25% of patients on SMT. Only 4 patients in the Algisyl group remained in NYHA class III at 12 months. These differences were highly statistically significant. The odds ratio favoring improvement by one class for Algisyl was 31.90 (CI 7.6–133.4); P < 0.001 12 AUGMENT-HF – Summary of 12 Month Outcomes Mean Difference Algisyl vs. Standard Medical Therapy P Value Algisyl vs. Standard Medical Therapy Peak VO2 (mL/kg/min) 2.10 < 0.001 Anaerobic Threshold (mL/kg/min) 2.34 < 0.001 Peak Watts 11.9 0.003 Total Exercise Time (min) 1.52 0.002 6-min walk test distance (m)a 101a < 0.001 NYHA class - 1.0 < 0.001 KCCQ Overall Summary score 13.4 0.016 KCCQ quality of life score 12.5 0.04 Outcomes a non-parametric test 13 13 All Adverse Events at 12 months SMT (N=38) Safety population Algisyl-LVR (N=40) # of patients # of patients Total # Total # with events with events of events of events (%) (%) P All adverse events 98 25 (66) 144 34 (85) <0.001# Serious adverse events 44 18 (47) 50 21 (53) 0.186# # p-value calculated by the log-rank test of the hazard ratio (hazard rate per 100 patient years at risk) 14 MACE and Mortality – Blinded CEC Adjudication SMT (N=38) Safety population Event Death Algisyl-LVR (N=40) Total # # of patients Total # # of of events (%) of events patients (%) 4 4 (10.5%) 9 9 (22.5%) Cardiovascular death 4 4 (10.5%) 8 8 (20.0%) Non-cardiovascular death 0 0 (0.0%) 1 1 (2.5%) 38 15 (39.5%) 19 10 (25.0%) Cardiovascular death 4 4 (10.5%) 6 6 (15.0%) Cardiac arrest 3 3 (7.9%) 2 2 (5.0%) Worsening heart failure 23 13 (34.2%) 11 6 (15.0%) Sustained ventricular arrhythmias 8 5 (13.2%) 1 1 (2.5%) MACE events (excludes index procedure) The study was not powered to detect differences in event rates and there were no statistically significant differences between groups for any of these event categories 15 The Future of Algisyl AUGMENT-HF II – Large US PMA Study (recent FDA cleared IDE) •Sample size of 240 patients, randomized 1:1 versus usual care •Endpoints essentially identical to the prior AUGMENT-HF study •Peak VO2 and Combined HF hospitalization and mortality Algisyl as a Percutaneous Intervention 16 Conclusions • We previously reported that Algisyl injections can be administered safely in patients with advanced HF, with an acceptable 30 day post-operative morbidity & mortality. • These one-year follow-up results from AUGMENT-HF demonstrate continued long term benefits of the Algisyl implant procedure in patients with advanced HF. • Algisyl combined with SMT provided substantial improvements in functional capacity & HF symptoms compared to patients on SMT alone at 1 year post treatment. • The 1 year MACE suggest a potential favorable reduction in HF hospitalization in patients treated with Algisyl. However there was a trend towards higher CV mortality and overall mortality at 1 year for patients receiving Algisyl. • Longer term observations for this patient cohort and larger studies will provide insights into important clinical outcomes such as HF hospitalizations and CV mortality 17