Size of the Economy - CUTS International

Competition Policy for the
Pharmaceuticals Sector in India
Nitya Nanda
CUTS, Jaipur
&
Amirullah Khan
IDF, Gurgaon
The Industry – A View
Almost non-existent before 1970, a prominent producer of healthcare products, meeting 95% of the country’s needs now
Indian production constitutes about 1.3% of the world market in value terms and 8% in volume terms
Likely to grow from about US$5.5bn in 2000 to US$25bn in 2020
Global attention during TRIPs and Public
Health debate – great promise
Doubts if the industry can provide affordable medicines even to the people in India
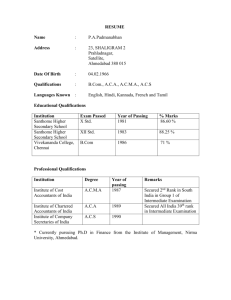
The global Scenario
Stage of development
Sophisticated pharmaceutical industry with a significant research base
Innovative capabilities
Industrial
10
12
6
Number of countries
Developing
Nil
6
(Argentina, Brazil,
China, India, Korea and
Mexico)
7 Those producing both therapeutic ingredients and finished products
Those producing finished products only
No pharmaceutical industry
Total
2
1
31
87
59
159
Total
10
18
13
89
60
190
Nature of the Industry
Four primary medical sciences: Allopathy,
Ayurveda, Unani and Homeopathy
Allopathic medicines - most important and are subject to price regulation
Market is broadly divided into bulk drugs
(20%) and formulations (80%)
The organized sector - 70% in terms of value.
The top ten companies - 30% of total sales
The individual market shares of companies are small – several products and several “relevant markets” within the industry
Roughly, different therapeutic segments and some of them are highly concentrated
Different Therapeutic Segments
Product category
Analgesics & Antipyretics
Antacids and Antiulcerants
Antibiotics
Patent Coverage
Most are off-patent.
High
Old generation - off-patent.
Newer generation - High
Low
DPCO Coverage Players
High Major players are Burroughs Wellcome, SmithKline Beecham,
Hoechst and Wockhardt.
A large number of local players
High
The latest generation drugs
Antacids: Knoll and Parke Davis.
Anti-ulcerants: Glaxo, Cadila, Ranbaxy, Dr Reddy’s Labs etc.
Glaxo, Ranbaxy, Cipla, Hoechst, Alembic, Burroughs
Wellcome, Ambalal Sarabhai etc.
Only Rifampicin Lupin (dominant), Hind. Ciba., Cadila, Glaxo and Hoechst Anti-tuberculosis products
Anti-parasitic &
Anti-fungal products
Cardiac Therapy
Low Relatively low
Low
Anti-protozoal: Nicholas Piramal, SmithKline Beecham
Pharma, Ranbaxy, and Cipla.
Anti-fungal: Bayer, Fulford, Glaxo etc.
Sun Pharma, Torrent, Cadila, ICI etc.
Corticosteroids
New drugs are many.
Popularly used in India:
Low.
All popularly used are offpatent.
NSAIDs, Antirheumatic products
Respiratory System ailments
Vitamins
Low
Very low.
Off-patent
Key drugs
Betamethasone and
Dexamethasone
High
Very low.
Very high
Glaxo, Crosslands, Wyeth, Fulford, Merind. etc.
Knoll, Roussel, Hind Ciba, Pfizer etc.
Anti-cough: Pfizer, Parke Davis, Nicholas Piramal.
Anti-cold: Burroughs, Alembic etc.
Anti-asthmatics: Cipla (dominant)
E-Merck, Pfizer, Glaxo, Abbott etc.
Pharmaceuticals Regulation
Consumption patterns are not affected by prices - a unique example of market failure
In many countries, government bears most or all of the costs of medicines - As a monopsonist, the government may be able to control drug prices
In developing countries, people are covered neither by public nor private insurance
The doctors and the pharmacists companies influence them
Bypassing doctors - fall prey to company advertisements or to local pharmacists, even in the US
Pharmaceuticals Regulation (Contd.)
Practically all countries in the world have mechanisms to regulate also a significant move to insist on generic prescription
Regulating Prescribing Doctors
Regulating Pharmacists
Regulating Prices
International benchmarking
Control on the evolution of prices over time
Control of prices relative to cost
Pharmaceuticals Regulation in India
In the early fifties, introduction of compulsory manufacturing of finished products and later, of raw materials of new drugs
In the 60s, two public sector companies,
Hindustan Antibiotics Ltd (HAL) and
Indian Drugs and Pharmaceuticals Ltd
(IDPL)
Till 1962, no price control
In 1962, control imposed under the
Defence of India Act, 1915 - The Drugs
(Display of Prices) Order, 1962 and the
Drugs (Control of Prices) Order, 1963
Pharmaceuticals Regulation in India
During 1970, the Indian Patents Act (IPA) and the Drug Prices Control Order (DPCO) issued under the Essential Commodities Act, 1955
DPCO revised in 1979, 1987 and 1995
DPCO 1970 was a direct control on the profitability and an indirect control on the prices
DPCO, 1979 stipulated ceiling prices and put 370 drugs under price control
Retail Price = (MC+CC+PM+PC) x (1+MAPE/100)
+ excise duty
(MC = material cost including cost of bulk drugs/excipients: CC = conversion cost; PM = cost of packing material; PC = packaging charge; MAPE =
Maximum Allowable Post-manufacturing Expenses)
Pharmaceuticals Regulation in India
DPCO, 1987, dugs under price control reduced from 370 to 142 and higher
MAPE provided
The New Drug Policy 1994 liberalised the criteria for selecting drugs for price control
DPCO 1995 - a uniform MAPE of 100% was granted
DPCO 1995 drugs under price control from 142 to just 76
The New Pharmaceutical Policy, 2002, number of drugs under price control to just 38
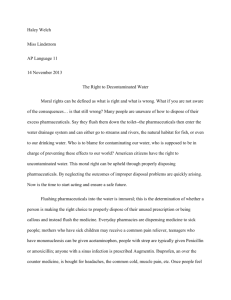
Market Shares of Drugs under DPCO
Year
Number of drugs
1979 347
1987 142
1995 74
2004 38
Approximate market share (%)
80
60
40
20
Decontrol and Prices
Price control and patent regime – prices among the lowest in the world
Prices started rising as soon as controls were removed - brand leader is usually one of the most expensive
Drugs under patent much cheaper in India but off-patent drugs (80-85% of current sales) are not necessarily cheaper
Prices of some top selling drugs are higher than those in Canada and the UK
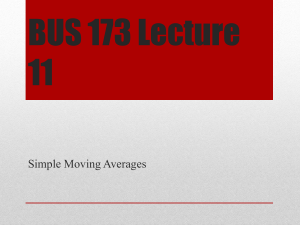
Decontrol and Prices - International
Cost Comparison of Select Drugs
Drug Dose Canada UK
Amoxycillin 250 mg 1.75 2.59
India
2.89
Ampicillin 250 mg 1.75
Erythromycin 250 mg 1.25
Cephalexin 250 mg 3.00
2.42
2.87
7.74
3.18
3.28 - 4.17
4.46
Propanolol
Atenolol
40 mg
50 mg
1.25
--
0.25
2.65
1.39
1.29
Prednisolone 10 mg 1.50 1.09 1.32
Paracetamol 500 mg 1.25 0.32 0.49
Haloperidol 0.25 mg 0.13 1.60 0.55
Phenobarbitone 30 mg 0.25 0.28 0.50
Decontrol and Prices
The price difference - no direct interaction between the consumer and the drug market
Pharmacists in developed countries - little influence over the volume of prescriptiondrug sales - marketing push usually targets doctors
Pharmacy owners banded together to form a huge cartel - All India Organization of
Chemists and Druggists (AIOCD)
AIOCD forced some drug companies to sign
"memorandums of understanding" to increase profit margins to pharmacies
Competition Issues: Collusions
No knowledge of domestic cartel.
Vitamins cartel alone cost India about
$25mn in the 1990s
Collusive behaviour of the pharmacies in
India is a matter of grave concern
Market becomes smaller due to high margin - harmful for the long run growth of the industry
December, 2004 the Ministry of Fertilisers
& Chemicals tried to bring in curbs on trade margins by amending the DPCO
Competition Act 2002 - only trade unions are allowed collective bargaining
Competition Issues: M&As
Industry is highly fragmented, intense consolidation activities expected
Top global pharmaceutical companies are consolidating – impacting in India
Large Indian companies are also expanding their reach overseas through acquisitions
The deals will require complex analysis - the impact on different therapeutic segments
For example, Glaxo-Wellcome-SmithKline
Beecham was allowed to merge conditionally in EU, divested product categories with competition concerns
Competition Issues: Abuse of Dominance
Patents Act, 1970 has significant implications for abuse of dominance
Absence of product patent - difficult to sustain monopoly
WTO TRIPS - product patent from 2005
The art of dealing with abuse of dominance (no experience)
Canada Patented Medicine Prices
Review Board (PMPRB)
Competition Act 2002 – provisions not strong enough
In Lieu of Conclusion
Manufacturers demanding more decontrol – arguing, competition will improve availability and affordability of essential drugs
UPA government's NCMP has promised to "take all steps to ensure the availability of life-saving drugs at reasonable prices"
Supreme Court order in the K.S. Gopinath case,
March 10, 2003, directing the government to ensure that “… essential and life-saving drugs do not fall out of price control"
In Lieu of Conclusion
Regulatory regime - hard on the manufacturers but soft on the doctors and the pharmacists
Indian Medical Council (Professional Conduct,
Etiquette and Ethics) Regulations 2002 – not effective
Bangladesh example?
Bulk drugs buyers are informed producers – different approach?
Import competition - Few specified life saving products at zero duty but for most others, the effective duty rate more than 56 percent
For scheduled (regulated) drugs, the MAPE is 100 percent for domestic and 50 percent for imported drugs