Poverty as it Relates to Child Welfare

Poverty As It Relates to
Child Welfare
Dr. Alan Dettlaff, Ph.D, Jane Addams College of Social Work (UIC)
Krista Thomas, MSW, Children’s Bureau – Region V
Womazetta Jones, IDCFS
20 th Annual African American Advisory Council Institute
April 13, 2012
Background on Racial Disparities
Racial disparity describes an unequal outcome experienced by one racial or ethnic group when compared to another racial or ethnic group.
Disparities can occur at every decision-making point, including the initial report of alleged maltreatment, indication of maltreatment, entries into substitute care, and exits from care.
Research examining decision-making points has documented disparities at each stage along the child welfare pathway.
At issue is whether race accounts for these disparities, or whether other factors may play stronger explanatory roles.
Critiques of Efforts to Reduce
Disparities
Critics of efforts to reduce racial disparities contend that the observed differences between African American and White children are due to the fact that African American children are maltreated at higher rates than children of other races.
Critics contends that higher rates of maltreatment in African
American families are to be expected because African
American children are more likely to be exposed to many of the risk factors associated with maltreatment, particularly poverty.
Critiques of Efforts to Reduce
Disparities
Prior research, most notably the federally funded National
Incidence Studies of Child Abuse and Neglect (NIS), had consistently shown no significant differences in the incidence of maltreatment across racial groups.
However, findings from the recently released NIS-4 found for the first time that rates of maltreatment for African American children were significantly higher than those for White or
Hispanic children.
In supplemental analyses of these race differences, the authors concluded that these observed differences are the result of greater precision of the NIS-4 estimates, as well as an increased disparity in income between African American and White families.
Poverty, Risk, and Maltreatment
Although poverty does not cause maltreatment, considerable evidence suggests that maltreatment occurs disproportionately among poor families.
Findings from the NIS-4 indicate that children in low SES households experience some form of maltreatment at a rate more than 5 times the rate of other children.
Research on Poverty and Racial
Disparities
Very few studies have examined the role of poverty in producing and contributing to racial disparities, and even among these, the evidence is mixed.
◦
Using national data comparing rates of child maltreatment to other child outcomes, Drake et al. (2011) conclude that poverty and associated risk factors are stronger drivers of racial disparities in reports of alleged maltreatment than racial bias.
◦
However, researchers in Texas have found that even after controlling for poverty, race remains a consistent predictor of the decision to substantiate cases of maltreatment and to place children in out-of-home care.
Despite conflicting and limited data, evidence exists that poverty, race, and maltreatment interact in important ways that need to be further understood and acknowledged.
National Data on Poverty, Race, and
Maltreatment
Wulczyn, F. (2011). Research Is Action: Disparity, Poverty, and the Need for New Knowledge. Chicago: Chapin Hall at the
University of Chicago
National Data on Poverty, Race, and
Maltreatment
Wulczyn, F. (2011). Research Is Action: Disparity, Poverty, and the Need for New Knowledge. Chicago: Chapin Hall at the
University of Chicago
National Data on Poverty, Race, and
Maltreatment
Wulczyn, F. (2011). Research Is Action: Disparity, Poverty, and the Need for New Knowledge. Chicago: Chapin Hall at the
University of Chicago
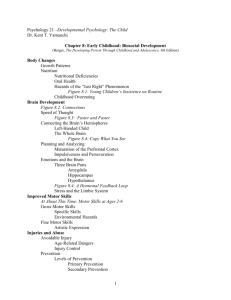
Illinois Data on Poverty, Race, &
Maltreatment
15%
10% y = 0.0389x + 0.0057
5%
0%
0% 20% 40% 60%
White Child Poverty Rate
80% 100%
Rolock, N., Dettlaff, A. D., Wilder J. R. & Jantz, I. (2011). The relationship between child victimization and child poverty rates in Illinois. Chicago, IL: University of Illinois at Chicago. Available at: www.socialwork.uic.edu/cwrc
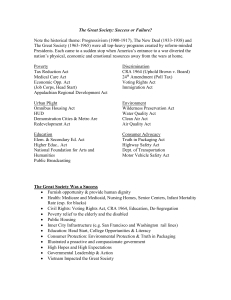
Illinois Data on Poverty, Race, &
Maltreatment
15%
10%
5% y = -0.0206x + 0.048
0%
0% 20% 40% 60%
Black Child Poverty Rate
80% 100%
Rolock, N., Dettlaff, A. D., Wilder J. R. & Jantz, I. (2011). The relationship between child victimization and child poverty rates in Illinois. Chicago, IL: University of Illinois at Chicago. Available at: www.socialwork.uic.edu/cwrc
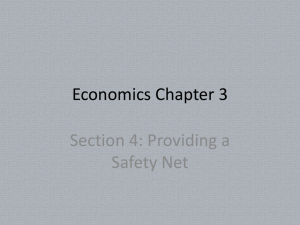
Texas Disparities Study - Removals
Rivaux, S. L., James, J., Wittenstrom, K., Baumann, D., Sheets, J., Henry, J., & Jeffries, V. (2008). The intersection of race, poverty, and risk: Understanding the decision to provide services to clients and to remove children. Child Welfare, 87,
151-168.
Supporting Low-Income Families:
Select Federal Child Welfare Initiatives
Title IV-E demonstration projects
◦ Flexible funding/title IV-E capped allocations
◦ Subsidized guardianship
Evidence-Based Home Visiting
Differential Response
Federal Child Welfare
Demonstration Projects
Titles IV-B and IV-E of the Social Security Act:
◦ Primary federal legislation related to child welfare and federal funding streams
◦ Majority of funding directed towards foster care placement and administration (Title IV-E) with the funding available for prevention and reunification services (Title IV-B) often insufficient to address depth of child and family need
1994: Passage of Public Law 103-432
◦ First introduced the idea of waiving certain title IV-B and IV-E requirements to allow states to test innovative and effective child welfare practices, often directed at services that protect children from abuse and neglect, preserve families, and facilitate permanency
◦ 1997 Passage of the Adoption and Families Act expanded the waiver authority
8 different categories of title IV-E child welfare demonstrations, including:
◦ Flexible funding/capped title IV-E allocations
◦ Subsidized guardianship
2011: The Child and Family Services Improvement and Innovation Act (Public
Law 112-34)
◦ Allows HHS to approve up to 10 new child welfare waiver demonstration projects in each of FYs 2012-2014
Title IV-E Flexible Funding Waivers
Two primary models
◦ Capped allocation: State receives an annual lump sum of federal title IV-E foster care dollars that are then distributed to local jurisdictions through state-determined allocation formulas (CA, FL, NC, OH, OR)
◦ Case-specific waiver payments/slots, distributed to counties based on demographic and other select variables (Indiana)
Flexible Funding Waivers:
What Did They Do?
Process evaluation findings showed that the availability of flexible funding did increase the amount and diversity of services available to vulnerable children and families
◦ New/expanded programs focused on family-centered case management models (e.g. Child and Family Team Meetings), supervised visitation, kinship/after care support, intensive placement prevention services, family finding and engagement programs, and respite care
Case-specific good and services provided through the use of flexible funds included: food and clothing; rental/housing assistance; utility assistance; household goods; transportation assistance/car repairs; child care and legal assistance
Flexible Funding Waivers: Have We Seen
Improved Outcomes for Children and Families?
Positive findings in placement prevention, exits to permanency, placement duration, and foster care re-entry and have been observed in some states
Maltreatment recurrence has been no higher in populations assigned to the waiver experimental groups – so children are at least as safe as those children in jurisdictions without access to flexible funding
Florida and Indiana: Positive, statistically significant findings across most major outcome areas
◦ Indiana found that families of children assigned to the waiver slots received certain goods and services at significantly higher levels than the comparison families, specifically family preservation services, household goods, homemaker services, transportation, housing assistance, money management training, life skills training, and childcare.
Most states have been able to increase their available revenue for a spectrum of child welfare services and ALL states have remained costneutral
Holistically, however, evidence of program impact remains inconclusive or mixed, with no consistent, positive patterns observed across all participating jurisdictions
Current Status of Flexible Funding
Demonstrations
STATE
California
Florida
Indiana
North Carolina
Ohio
Oregon
START DATE
7/1/2007
10/1/2006
1/1/1998
7/1/1997
10/1/1997
7/1/1997
COMPLETION
DATE
6/30/2013
7/31/2012
9/30/2011
2/28/2008
9/30/2015
6/30/2016
Subsidized Guardianship Waivers
Purpose: To test the extent to which the availability of subsidized guardianship (SG) increased exits from foster care among children for whom reunification and adoption were not viable options
Eleven states implemented SG waivers:
◦ Delaware, Illinois, Iowa, Maryland, Minnesota, Montana, New
Mexico, North Carolina, Oregon, Tennessee, and Wisconsin
◦ All have concluded as of 2011
Positive evidence from this cluster of waiver projects
(dominated largely by Illinois’ findings) resulted in the enactment of the Guardianship Assistance Program under the Fostering Connections to Success and Adoption Act of
2008;
◦ Provides states the option to amend their title IV-E foster care state plans to provide kinship guardianship assistance payments on behalf of eligible children
Subsidized Guardianship:
Some Background
Increased support among the child welfare field that some children and youth, esp. those placed with relatives, needed another permanency option
Private guardianship: Long-standing permanency option where legal custody is transferred to a private caregiver
◦ Caregiver gains authority for the care, control, and supervision and increased decision-making capability on behalf of the child
◦ Reduction in administrative oversight and intrusion by the child welfare agency, since the child exits foster care
◦ Does not require termination of birth parents’ parental rights
◦ Prior to the option of SG, guardians then lost the monetary supports and services that were made available to them as foster parents – NOT an economically viable option for many families
Subsidized guardianship – caregivers could become permanency placement resources for the children in their care without losing the financial supports and services needed to support those placements.
Subsidized Guardianship Waivers:
What Did We Learn?
Several states saw big boosts in their overall permanency rates for children assigned to the experimental group
◦ 6.6% here in Illinois
◦ 18% in Wisconsin
Findings from IL, MN, TN, and WI show that reunification rates were not significantly impacted
Evidence about impact on adoptions less definitive
◦ Indication that many children in IL and TN who exited to SG would have been adopted over time
Subsidized Guardianship Waivers:
What Did We Learn? (cont’d)
Decreased lengths of stay in almost all SG waiver projects, ranging from 269 less days in Illinois’ original waiver project to 80 less days in Tennessee
Consistent findings that children placed with guardians are at least as safe or safer from repeat maltreatment than children in other placement settings, particularly reunification
Comparable placement stability rates (IA, TN, and WI)
Comparable foster care re-entry rates
Consistent findings that children in SG placements fared as well or better than children in foster care or other permanent placements with regards to outcomes like school performance and engagement in risky behaviors.
Strengths of Subsidized Guardianship
Provides emotional and physical stability for children and youth without having to terminate parental rights
◦ Maintains existing family relationships
◦ Maintains on-going contact and/or the potential for reunification
(if appropriate) with a birth parent
◦ Provides low-income permanent relative caregivers additional financial resources to support the children in their care
Respects the values and preferences of certain cultural/ethnic groups
Youth felt the permanency provided through SG helped them shed the stigma of foster care, feel more stable, and have more freedom to engage in “normal” childhood activities
Saves States money, primarily through reduced lengths of stay and reduced administrative expenses
Home Visiting Programs
Evidence-Based Home Visiting Initiative
◦ HHS/ACF/Children’s Bureau program
◦ 17 grantees across 15 states (including Illinois)
◦ 5 year initiative, began in 2008
Affordable Care Act Maternal, Infant and
Early Childhood Home Visiting Program
◦ Health Resources and Services Administration
(HRSA) Program
◦ Formula grant distributed to states
◦ Funding available FFY 2010-2014 (~$90M for
2010 alone)
What is Home Visiting?
Method of early intervention service delivery, particularly for highrisk families with infants and young children, where services are provided from within the family’s home
Multiple home-visiting models, varying by:
Age of child
Risk status of the family
Range and intensity of services
Curriculum
Service provider (professional vs. para-professional)
Home visitors can provide social support; act as resource and referral providers; be literacy teachers, parenting coaches, role models, and parent and child health and well-being experts
Premise underlying home visiting programs is that services provided in the home will be a beneficial and cost-effective way to positively impact families and shape parenting practices in a way that will have measurable, long-term benefits for children’s development
Home Visiting: Grounded in the
Evidence
EBHV and MIECHV grantees required to select an evidence-based home visiting model
While not consistent across all models, home visiting programs have shown favorable impacts in:
◦ Child development and school readiness
◦ Family economic self-sufficiency
◦ Positive parenting practices
◦ Child health
◦ Maternal Health
◦ Reductions in child maltreatment
◦ Linkages and referrals
Differential Response
Emerged out of the growing movement for strengths-based, family-centered approaches to supporting child and family well-being
Beginning in Florida and Missouri 1993, currently active some level in ~19 states
Central tenet: Many children and families that reach the attention of the child welfare system could be better served through a collaborative and supportive model outside the constraints and stigma of an investigation
Children’s Bureau’s Support of
Differential Response
National Quality Improvement Center on
Differential Response in Child Protective Services
◦ Design and conduct evaluation, to rigorously study implementation, outcomes and cost impact of differential response in research and demonstration sites
◦ Learn if differential response is an effective approach in CPS
◦ Build cutting-edge, innovative and replicable knowledge about differential response, including guidance on best practices in differential response.
Illinois, Ohio, and Colorado selected as the research and demonstration sites
HHS/Children’s Bureau Resources
Title IV-E Waiver Demonstration Projects
◦ http://www.acf.hhs.gov/programs/cb/programs_fu nd/
Evidence Based Home Visiting
◦ http://supportingebhv.org/
National Quality Improvement Center on
Differential Response on Child Protective
Services
◦ http://differentialresponseqic.org/
Illinois Department of Children
& Family Services
Differential Response
Pathways to Strengthening & Supporting Families
Womazetta Jones, Project Director
What is Differential Response (DR)?
An alternative means of responding to allegations of child maltreatment.
Approximately 17 states are using a statewide DR system or have implemented DR within some counties
Criteria For DR In Illinois
Names and current address of the family are known;
Alleged offenders are the parents, legal guardian, or responsible relative;
No prior indicated reports of abuse and/or neglect or;
Prior indicated reports have been expunged;
No pending investigations;
Alleged victim (s) or other siblings or household members are not currently in the care or custody of DCFS or wards of the court;
Protective custody has not been taken or required in the current or any previous case;
Allegations include, individuality or combination
Inadequate Food
Inadequate Clothing
Environmental Neglect
Mental & Emotional Impairment
Neglect
Inadequate Shelter
Inadequate Supervision
Medical Neglect
Risk of Harm Due to
Staffing
Public Sector: DR Specialist (DCFS)- Assess Safety
Memorandum Of Understanding with AFSCME
30 DR Specialists
6 Supervisors
Private Sector: Strengthening and Supporting Family
(SSF) Worker- Change Agent
13 Private Agencies with DR Contracts
13 SSF Supervisors
40 SSF Workers
Caseload Ratio 12:1
Strengthening and Supporting Families (SSF) Staff:
Agents of Change
Initial Visit- Paired Team
SSF Worker is the Change Agent
Worker is the service
Evidence base practices
◦ Six Protective Factors
◦ Recovery Coach Model
◦ Home Visiting Model
Not a referral and linkage program
Short term and intensive
How are we helping to strengthen and support families
Addressing the Needs identified by the Family
• Listening
• Mentoring
• Nutrition
• Cash Assistance
• Parent Café
• Partnering With Parent (PWP)
Engagement
Counseling
Transportation
Homemaker
Advocacy
Budgeting
AND MORE
Statistical Data
November 1, 2010- March 31, 2012
2772 Case Have Been Randomized to DR
271 Families Have Declined Services
557 Cases Have Redirected to Investigation
Evaluation
Random Control Trial (RCT): Compares outcomes for families randomly assigned to the investigation or DR pathway
Process Evaluation:Looks at how DR is implemented at the agency level and at the caseworker level
Cost Evaluation: Looks at how much it costs to “treat” a case
(on average) in the Investigation versus DR pathways – factoring in both short-term and long-term (i.e., re-reports) costs
Cross Site Evaluation Questions
-Child Safety: Are children whose families receive the noninvestigation pathway as safe as or safer than children whose families receive the investigation pathway?
-Pathway Differences: How is the non-investigation pathway different from then investigation pathway in terms of family
engagement, caseworker practice, and services provided?
-Program Costs: What are the cost and funding implications to the child protection agency of the implementation and maintenance of a DR approach?
Why Continue To Do This?
• Impact
With Our Families
Within the Community