Marin McDonald, MD PhD Julie Bykowski, MD RSNA
advertisement

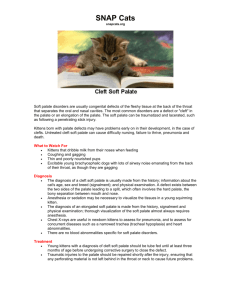
Imaging of Palate Masses Marin McDonald, MD PhD Julie Bykowski, MD ASNR Annual Meeting – Chicago 2015 Disclosures • The authors have nothing to disclose. Educational goals and summary of cases • Key cases will be used to define anatomy, regional vascular supply, drainage and innervation, as well as indications and implications for surgical resection. • Benign: pleomorphic adenoma, papilloma, benign osseous lesions. hemangioma, necrotizing metaplasia, osteomyelitis • Malignant: adenoid cystic carcinoma, mucoepidermoid carcinoma, squamous cell, lymphoma and sarcoma • Common imaging findings suggesting perineural and lymphangitic spread of palate-based malignancies • NCCN guidelines for diagnosis, evaluation and treatment. Anatomy of the hard and soft palate Soft palate Nasal cavity Nasopharynx Hard palate Oropharynx tongue Hypopharynx epiglottis trachea trachea esophagus Adapted from instantanatomy.net Anatomy of the hard and soft palate incisive fossa Soft palate Nasal cavity Nasopharynx Hard palate Oropharynx Palatine plate Horizontal plate tongue Hypopharynx epiglottis trachea trachea esophagus Greater and lesser palatine foramen Soft palate Tensor and Levator veli palatini Adapted from instantanatomy.net Anatomy of the hard and soft palate • Hard palate: anterior 2/3 • Thick mucosa covered by ketanized stratified squamous epithelium • Minor salivary glands predominant along posterior margin • Soft palate: posterior 1/3 • Formed by connective tissue, the glosspalatine and pharyngopalatine muscles • Covered by nonkeratinized squamous mucosa • Mobility via tensor and levator veli palatini incisive fossa Palatine plate Horizontal plate Greater and lesser palatine foramen Soft palate Tensor and Levator veli palatini Tumors of the palate • Benign and malignant palatal tumors are usually asymptomatic masses that are occasionally associated with a low level of discomfort. • Up to 50% of hard palate tumors are locally spread at time of presentaton • Standard evaluation includes: • Full head and neck exam • Trismus oropharyngeal involvement • Masseter wasting -> maxilary PNI • Palatal hyperesthesia -> maxillary PNI • CT – extent of tumor burden, osseous invasion • MR – soft tissue evaluation, PNI • FNA/excision Benign palate masses • Represent ~ 50% of all palate based tumors • Most common salivary type – pleomorphic adenoma • Most common epithelial type – papilloma • Others including • • • • Benign osseous lesions Mucopideroid Hemangioma Necrotizing metaplasia Palate masses: pleomorphic adenoma • Most common type of salivary gland tumor of the palate •Commonly located lateral to the midline of the posterior hard palate. • Painless, firm or rubbery, slow-growing, well-delineated masses that are covered with normal mucous membranes • Fibrous capsules appearing as hypointense on T2-weighted images with characteristic delayed enhancement Palate masses : benign osseous lesions Torus palatini • Developmental exostosis that arises from the midline of the hard palate. • Classified as flat, nodular, lobular or spindle types • Replacement of normal bone with fibrous connective tissue • Expansile lesions with groundglass opacity Fibrous dysplasia Palate masses: papilloma • Benign epithelial tumor composed of squamous epithelium • HPV subtypes 6 and 11 identified in up to 50% of oral papillomas 39 y/o M presenting with an intranasal mass Palate masses: papilloma (natural history of …) CT noncontrast 2007 CT noncontrast 2011 (concerning for malignant degeneration, but pathology consistent with inverted papilloma w/o dysplasia) Palate masses: hemangioma • Vascular anomalies are classified as infantile hemangiomas and vascular malformations (capillary, venous, lymphatic, and arteriovenous types) • On T2-weighted images, generally appear as multiple hyperintense lobules (“bunch of grapes”) Anatomy of the hard and soft palate • Blood supply: from the maxillary artery via the descending palatine artery • Hard palate: greater palatine artery • Soft palate: lesser palatine artery •Venous drainage: pterygoid plexus Greater palatine foramen Incisive fossa lesser palatine foramen Nasopalatine nerve Greater palatine artery Greater palatine nerve Lesser palatine arteries Lesser palatine nerves Adapted from instantanatomy.net Necrotizing sialometaplasia 24 y/o otherwise healthy female with new lesion on roof of mouth • Nonneoplastic inflammatory condition of the salivary glands, with over 75% occurring on the palate • Underlying etiology thought to be related to ischemia, typically present as a crateriform ulcer of the palate that spontaneously resolves • Often not seen on imaging Palate masses - malignant • Represent about half of all palate based tumors • Different spectrum of tumor pathology based on location • Hard palate – minor salivary gland malignances (e.g. mucoepidermoid) • Soft palate – majority squamous cell carcinoma • Varied patterns of spread require multidisciplinary approach to diagnosis • Full H/N exam (mastoid effusion? Nasosinal disease? Absent masseteric reflex?) • CT to evaluate for osseous invasion, lymphatic involvement • MR to improve resolution of PNI • Local excision/punch biopsy for pathology Tumors of the palate: size matters •Staging of primary tumor (T) •T0 - carcinoma in situ •T1 - Tumor <2 cm •T2 - Tumor larger > 2 cm but < 4 cm •T3 - Tumor > 4cm •T4 – local invasion Tumors of the palate: size matters •Staging of primary tumor (T) •T0 - carcinoma in situ •T1 - Tumor <2 cm •T2 - Tumor larger > 2 cm but < 4 cm •T3 - Tumor > 4cm •T4 – local invasion •Diagnosis: Mucoepidermoid •1.5% of all salivary gland tumors •Presents as a well-circumscribed mass with smooth or lobulated margins • Various degrees of enhancement Tumors of the palate: size matters •Staging of primary tumor (T) •T0 - carcinoma in situ •T1 - Tumor <2 cm •T2 - Tumor larger > 2 cm but < 4 cm •T3 - Tumor > 4cm •T4 – local invasion • Diagnosis: Adenoid cystic carcinoma, T3 • Most common salivary gland malignancy in the palate • Can appear either as a benign or malignant lesion • High-grade tumors have a proclivity for bone invasion Tumors of the palate: size matters •Staging of primary tumor (T) •T0 - carcinoma in situ •T1 - Tumor <2 cm •T2 - Tumor larger > 2 cm but < 4 cm •T3 - Tumor > 4cm •T4 – local invasion • Diagnosis: Invasive squamous cell carcinoma, T4 • Approximately half of all palatal malignancies are SCCs •up to 50% hard palate malignancies, 80% soft palate lesions • Extension beyond the hard palate occurs in up to 70% of lesions at presentation Tumors of the palate: size matters •Staging of primary tumor (T) •T0 - carcinoma in situ •T1 - Tumor <2 cm •T2 - Tumor larger > 2 cm but < 4 cm •T3 - Tumor > 4cm •T4 – local invasion • Diagnosis: adenoid cystic carcinoma with perineural invasion, T4 •High-grade tumors have a proclivity for perineural spread along the greater and lesser palatine nerves, followed by extension to the pterygopalatine fossa and cavernous sinus Tumors of the palate: perineural spread intracranial PGP fossa Infraorbital canal Infraorbital nerve Superior alveolar nerves CNV ganglion Lesser palatine nerve Nasopalatine nerve Greater palatine nerve Adapted from teachmeanatomy.net face Tumors of the palate: perineural spread Subtle widening of the right greater palatine foramen (left) is the only indicated on CT of perineural invasion, later confirmed on MRI with gadolinium. Thickening and enhancement of the right greater palatine nerve (center) confirms perineural spread of the patient’s adenoid cystic carcinoma, which extends cephalad towards the pteropalatine gangion (right). Special cases: Polymorphous low-grade adenocarcinoma • Rare type of salivary gland malignancy, most common site is the hard or soft palate • Asymptomatic, slow-growing masses that are covered by nonulcerated mucosa • Imaging features of PLGA are nonspecific. •potentially cause bone resorption, medullary infiltration, and invasion of nearby nerves and blood vessels •Metastasis to a lymph node are extraordinarily rare Special cases: lymphoma 44 M with ALL and new onset trismus • Approximately 20% of oral non-Hodgkin lymphomas occur in the palate • Commonly arise at the junction of the hard and soft palate. • B-cell non-Hodgkin lymphomas • Can present either an expansile or destructive growth pattern , often with associated lymphadenopathy Tumors of the palate: lymphatic spread and staging I •Lymphatic involvement can be assessed by either CT or MR III •Most commonly seen in SCCs and high grade mucoepidermoid tumors, soft palate >>hard palate •Up to 30% soft palate with lymphatic spread on presentation II V IV •Predilection for: •Retropharyngeal (particularly with posterior extension of soft palate SCCs) •Level I •Level II Special cases: lymphoma 12/27/2013 4/3/2014 (s/p chemoradiation) Special cases: osteomyelitis CT 12/3/2012 CT 4/6/2012 56 M diabetic with invasive fundal sinusitis, status post left orbital exteneration and sphenoidectomy. CT 4/6/4012 demonstrates extensive interval erosion of the hard palate with ill-defined heterogenously enhancing phlegmon, compatible with osteomyelitis of the hard palate. Special cases: recurrence 43 F status post resection of prior left palatal SCC with resection of left mandibular body, left maxilla and flap reconstruction. New soft tissue thickening and enhancement along the left posterior nasopharynx and oropharynx extending to the left parapharyngeal space, later biopsy proven recurrent veruccous SCC Special cases: sarcoma 30 month old female with left sided facial swelling and proptosis On CT, ill-defined mass centered within the left maxilla and hard palate with extension into the left maxillary sinus and orbital floor (top left). Significant widening and soft tissue extension of the left infraorbital foramen concerning for perineural spread (top right), confirmed on subsequent MRI by enhacenement nad thickeing of the left infraorbital nerve (bottom right). Diagnosis: melanotic neuroectodermal tumor of infancy (MNTI) Conclusion • Think beyond squamous cell carcinoma when approaching palatal masses • Over 50% of malignant lesions present with local spread at presentation, making clinical history and adjunctive imaging of critical importance • Soft palate SCCs have a much higher predilection for lymph node spread than salivary gland malignancies/hard palate tumors • Subtle changes such as palatine foramina widening may be the first indicated of PNI • A multidisciplinary approach is crucial for the staging and treatment of palate malignancies Self-assessment #1 A. The yellow arrow in the figure #1 is indicating which anatomic structure? 1. The incisive foramen 2. The greater palatine foramen 3. The lesser palatine foramen Fig. 1 Self-assessment #1 A. The yellow arrow in the figure #1 is indicating which anatomic structure? Fig. 1 1. The incisive foramen 2. The greater palatine foramen 3. The lesser palatine foramen The yellow arrow highlights the greater palatine foramen, the entry point of greater palatine nerve, which supplies sensory innervation to the hard palate Self-assessment #2 Fig. 1 In comparison to the above case, what does the appearance of the greater palatine foramen in figure 2 suggest? 1. 2. 3. Perineural spread Osseous invasion Lymphatic spread Fig. 2 Self-assessment #2 Fig. 1 In comparison to the above case, what does the appearance of the greater palatine foramen in figure 2 suggest? 1. 2. 3. Perineural spread Osseous invasion Lymphatic spread The yellow arrow highlights the greater palatine foramen, the entry point of greater palatine nerve, which supplies sensory innervation to the hard palate Fig. 2 Self-assessment #3 What stage is this hard palate tumor? 1. 2. 3. 4. T1 T2 T3 T4 5.2 cm Self-assessment #3 What stage is this hard palate tumor? 1. 2. 3. 4. T1 T2 T3 T4 Staging of primary tumor (T) T0 - carcinoma in situ T1 - Tumor <2 cm T2 - Tumor larger > 2 cm but < 4 cm T3 - Tumor > 4cm T4 – local invasion In the absence of osseous invasion, the 5.2 cm tumor is a stage T3. 5.2 cm References • • • • CT and MR imaging findings of hard palate tumrs. Kato H, Kanematsu M, Makita H, Kato K, Hatakeyama D, Shibata T, Mizuta K, Aoki M. Imaging of Perineural Tumor Spread from Palatal Carcinoma Lawrence E. Ginsberg and Franco DeMonte AJNR Am J Neuroradiol 19:1417–1422, September 1998 Cervical metastases from squamous cell carcinoma of hard palate and maxillary alveolus: A retrospective study of 10 years. Yang Z, Deng R, Sun G, Huang X, Tang E. Head Neck. Jun 4 2013 Malignant neoplasms of the hard palate and upper alveolar ridge. Petruzzelli GJ, Myers EN. Oncology (Huntingt). Apr 1994;8(4):43-8