Pulse and Blood Pressure
advertisement

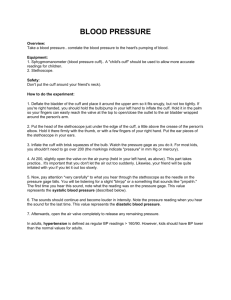
Readings taken from a patient Blood Pressure Respiratory Rate Arterial Pulse Body temperature Results from the alternating expansion and recoil of an artery Occurs with each beat of the Left ventricle creating a pressure wave Pulse rate normally equals the heart rate Average of about 70 – 76 BPM Felt in an artery that is close to the surface Pressure points- used to stop blood flow into distal tissues Compress the artery – do not apply too much pressure Radial arterial pulse Located distal forearm at wrist on radial side Routinely used to take a pulse Superficial temporal pulse – head Facial Artery – by the TMJ Common carotid artery – neck Brachial artery - at the antebrachial fossa Femoral Artery – groin Popliteal Artery – behind the knee (popliteal region) Posterior Tibial Artery – at the medial malleolus Dorsalis Pedis Superficial temporal artery Facial artery Common carotid artery Brachial artery Radial artery Femoral artery Popliteal artery Posterior tibial artery Dorsalis pedis artery Use your first 2 or 3 fingers Do not use the thumb (has own pulse) Press firmly then ease compression Feel for the pulse If no pulse, then you are pressing too hard or you are not in the right location The pressure the blood exerts on the walls of blood vessels allows for circulation Created from an increase in arterial pressure from a ventricle that is contracting Pressure is highest closer to the heart and in larger arteries (aorta, brachial) Pressure is greater on the left (closer to the heart) Pressure drops continuously until virtually zero in the Vena Cava Most distal, before return to the heart Venous return to the heart does not rely solely on blood pressure Veins – valves to prevent backflow Compression of the skeletal muscle Differences in flow A cut vein – see even flow of blood Arterial – pulsating blood flow Arteries provide elasticity - compression of arteries will aid the blood flow −10 Venae cavae Veins Venules Capillaries Arterioles Arteries 60 Aorta Pressure (mm Hg) 120 Systolic pressure 100 80 Diastolic pressure 40 20 0 Measure 2 pressures Systolic pressure – arterial pressure is high due to ventricular contraction Diastolic pressure – results from the relaxation of ventricles Units of measurement (mmHg) 120/80 Systolic/ Diastolic Pressure is greater on the left (closer to the heart) Pressure drops continuously until virtually zero in the Vena Cava Pressure is low pressure Most distal, before return to the heart Venous return to the heart does not rely solely on blood pressure Veins – valves to prevent backflow Compression of the skeletal muscle Blood pressure 120 systolic 70 diastolic (to be measured) Brachial artery (a) The course of the brachial artery of the arm. Assume a blood pressure of 120/70 in a young, healthy person. Pressure in cuff above 120; no sounds audible 120 mm Hg Rubber cuff inflated with air Brachial artery closed (b) The blood pressure cuff is wrapped snugly around the arm just above the elbow and inflated until the cuff pressure exceeds the systolic blood pressure. At this point, blood flow into the arm is stopped, and a brachial pulse cannot be felt or heard. Pressure in cuff below 120, but above 70 120 mm Hg 70 mm Hg Sounds audible in stethoscope (c) The pressure in the cuff is gradually reduced while the examiner listens (auscultates) for sounds in the brachial artery with a stethoscope. The pressure read as the first soft tapping sounds are heard (the first point at which a small amount of blood is spurting through the constricted artery) is recorded as the systolic pressure. Pressure in cuff below 70; no sounds audible 70 mm Hg (d) As the pressure is reduced still further, the sounds become louder and more distinct; when the artery is no longer constricted and blood flows freely, the sounds can no longer be heard. The pressure at which the sounds disappear is recorded as the diastolic pressure. Blood pressure 120 systolic 70 diastolic (to be measured) Rubber cuff inflated with air Brachial artery (a) The course of the brachial artery of the arm. Assume a blood pressure of 120/70 in a young, healthy person. Pressure in cuff above 120; no sounds audible Pressure in cuff below 120, but above 70 120 mm Hg 120 mm Hg 70 mm Hg Brachial artery closed Pressure in cuff below 70; no sounds audible 70 mm Hg Sounds audible in stethoscope (c) The pressure in the (b) The blood pressure cuff is gradually cuff is wrapped reduced while the snugly around the examiner listens arm just above the (auscultates) for elbow and inflated sounds in the until the cuff brachial artery with pressure exceeds a stethoscope. The the systolic blood pressure read as the pressure. At this first soft tapping point, blood flow into sounds are heard the arm is stopped, (the first point at and a brachial pulse which a small cannot be felt or amount of blood is heard. spurting through the constricted artery) is recorded as the systolic pressure. (d) As the pressure is reduced still further, the sounds become louder and more distinct; when the artery is no longer constricted and blood flows freely, the sounds can no longer be heard. The pressure at which the sounds disappear is recorded as the diastolic pressure. Arterial Blood Pressure (BP) is directly related to: Cardiac Output (CO) The amount of blood pumped out of the left ventricle / min. Peripheral Resistance (PR) The amount of friction the blood encounters as it flows through the arteries The amount of friction the blood encounters as it flows through the arteries Arterial constriction- narrowing of the blood vessels due to a Sympathetic N.S. response or atherosclerosis Increased blood volume Increased blood viscosity – thickness Other factors Age, weight, time of day, exercise, body position, emotions, drugs I. Neural Factors 1. Autonomic Nervous System a. 2 divisions – Sympathetic and Parasympathetic 1. Sympathetic – to stimulate 2. Parasympathetic – calm down (has no effect) b. Sympathetic stimulation 1. causes vasoconstriction (narrowing of the BV) 2. center located in the Medulla of the brain (Involuntary) 3. if active, causes vasoconstriction c. Activated by: 1. Standing suddenly after lying down 2. This causes blood pooling in legs and feet 3. Activates special receptors (Baroreceptors) in large arteries of the neck and chest 4. This in turn will signal a reflexive vasoconstriction and an increase in blood pressure back to normal (homeostatic) levels 2. Hemorrhage – results in a decreased blood volume a. B.P. drops b. Increased heart rate trying to compensate c. decreased blood results in decreased venous return d. sympathetic system turns on and results in vasocontriction 3. Vigorous exercise or being frightened a. this results in the “Fight or Flight” response b. results in generalized vasoconstriction except in the skeletal muscles 1. dilate to increase the blood flow to working muscles c. Sympathetic system will never cause vasoconstriction of the Blood Vessels of the heart and Brain II. Renal Factors - Kidneys 1. help to regulate B.P. by Regulating water a. when the BP and or blood volume inc., the kidneys will allow more water to leave the body in the urine b. this will decrease the blood volume and will in turn decrease the BP c. If dec. arterial BP, the kidneys will retain water to try to inc. BP. 2. Renin – an enzyme released by the kidney cells when Arterial BP is low. a. Renin stimulates a series of reaction to form Angiotensin II 1. a potent vasoconstrictor 2. stimulates the Adrenal cortex to release Aldosterone 3. this will inc. Na+ ion re-absorption by kidneys, then inc. water re-absorption and then blood volume III. Temperature 1. cold results in vasoconstriction a. Reduces blood flow and swelling 2. Heat causes vasodilating effect a. used to speed circulation into inflamed areas IV. Chemicals - drugs a. Epinephrine – inc. both heart rate and BP b. Nicotine – Inc. BP by causing Vasoconstriction c. Alcohol and Histamines – cause vasodilation and decreased BP. “Drunken face” V. Diet 1. diet low in slat, saturated fats and Cholesterol help to prevent Normal Adult Range a. Systolic between 110-140 mmHg b. Diastolic between 70-80 c. Varies during the day, usually peak in the A.M. d. varies by weight, age, race, mood, exertion and posture 1. Hypotension (low blood pressure) a. Systolic below 1090 mmHg b. usually the result of physical conditioning c. associated with long life and an old age free of illness 2. Orthostatic Hypotension a. Seen in the elderly b. a temporary low BP and dizziness when they rise suddenly c. usually results from an aging sympathetic NS responding slowly to change 3. Chronic Hypotension a. May result from poor nutrition and inadequate levels of blood proteins b. low blood viscosity will result in low blood pressure c. Acute Hypotension – warning of circulatory shock 1. inadequate circulation 2. Blood loss being the most common cause 4. Hypertension a. May temporarily rise with exercise, fever, emotion b. Persistent Hypertension – High Blood Pressure 1. Pathological – when BP is elevated over 140/90 c. Chronic condition 1. usually will progress 10-20 yrs without symptoms 2. strains the heart and damages arteries 3. called the Silent Killer 4. Heart pumps against resistance a. enlarges the heart (Enlarged Myocardium) 5. the walls of the heart become flabby 6. blood vessels become enlarged, tear the endotheilium which increases Atherosclerosis d. associated with long life and an old age free of illness 4. Primary (Essential) Hypertension a. no specific cause b. usually due to diet, obesity, heredity, race and stress 1. Women > Men Black > White c. child of HTN parent is 2X greater risk d. Obesity – the length of Blood Vessels increases 1. each pound of fat requires miles of additional blood vessels 2. the heart needs to work harder 1. Results in the narrowing of the arteries a. causes damming up process of the interior lumen (wall) b. The vessel walls thicken and protrude into the lumen c. the vessels can close easily from a roaming clot d. Usually effects the aorta and coronary vessels Onset and Stages According to the Response to injury hypothesis: 1. initial event is damage to the Tunica Intima caused by a. chemicals Carbon Monoxide (Cigarettes and car exhaust) b. bacteria or viruses c. physical factors (trauma or persistent HTN) 2. once the lumen breaks, platelets cling to the site of injury 3. clotting begins to prevent blood loss and the inflammatory process to repair begins. a. if a one time injury, then it is over 4. If persistent, the plaque will continue to grow Onset and Stages (Continued) According to the Response to injury hypothesis: 5. plaques grow through series of injuries and healing, and rupture again 6. endothelial cells release Chemotactic agents that increase the permeability of the endothelium to fats and Cholesterol to deposit in the tunica inima 7. Monocytes arrive to act as a Macrophage and engorge on the fat which turns them into lipid filled “foam cells” a. they now lose the ability to act as a scaenger 8. these cells join with smooth muscle cells from the T.I. and deposit collagen and fat (more “Foam Cells”) a. results in the “Fatty Streak stage” 1. thickening of t.i. by greasy gray yellow lesions called fibrous or atherosclerotic plaques 9. protrusion of these lesions into the lumen is called atherosclerosis 1. The end stage of Atherosclerosis a. enlarged plaques hinder nutrient diffusion to deep tissue of the artery b. results in the death of smooth muscle cells in the tunica media, fills with scar tissue and loses elasticity c. calcium salts deposit to form complicated plaques d. results in the fraying and ulceration of the arterial wall that encourages thrombus formation e. increased rigidity will lead to Hyppertension f. see an increase risk of stroke, Myocardial infarctions and aneurysims