Slide Deck
advertisement

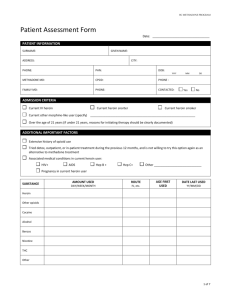
Decreasing the Use of Prescription Opiates and Benzodiazepines Among Individuals Enrolled in Methadone Programs Kim Castelnovo, RPh Pharmacy Manager, Community Care © 2014 Community Care Behavioral Health Organization About Community Care • Behavioral Health Managed Care Company • Founded in 1996 • Statewide HealthChoices presence; 39 of 67 Pennsylvania counties • 10 offices across the Commonwealth • Over 600 employees © 2014 Community Care Behavioral Health Organization 2 About Community Care • Medicaid/HealthChoices membership: 725,000 • Commercial/Medicare membership: 450,000 • Approximately 110,000 people served annually • Statewide network of approximately 1,600 providers © 2014 Community Care Behavioral Health Organization 3 Serving 39 Counties Erie Warren McKean Potter Tioga Bradford Susquehanna Crawford Wayne Forest Cameron Venango Sullivan Elk Lycoming Mercer Clinton Jefferson Clarion Lawrence Clearfield Butler Centre Armstrong Beaver Allegheny Mifflin Indiana Cambria Westmoreland Perry Dauphin Huntingdon Washington Greene Franklin Adams Bucks Lancaster Bedford Fulton Berks Lebanon Montgomery Cumberland Somerset Pike Pike Luzerne Columbia Monroe Montour Union Carbon Northumberland Snyder Northampton Schuylkill Lehigh Juniata Blair Fayette Wyoming Lackawanna York Chester Philadelphia Delaware Community Care Office © 2014 Community Care Behavioral Health Organization 4 Overview • Opiate and benzodiazepine use in individuals in methadone programs – With overdose deaths from heroin and prescription pain medications increasing in the U.S., opioid addiction is an important concern for Medicaid programs – Medicaid beneficiaries have higher rates of opioid addiction than other insured groups © 2014 Community Care Behavioral Health Organization 5 Benzodiazepine Use and Misuse • Among patients in a methadone program – BMC Psychiatry, May 2011: – Benzodiazepines (BZD) misuse and abuse is a serious public health problem in the U.S. – This problem is especially pertinent among those with opiate dependence because these individuals are more likely to experience elevated anxiety after stopping use of opiates – It has been shown that individuals who abuse BZD are at increased risk of continuing opiate abuse and failing to stay in methadone treatment © 2014 Community Care Behavioral Health Organization 6 Benzodiazepine Use and Misuse • In a Baltimore methadone program: – Survey conducted at a methadone treatment program in Baltimore – 194 questionnaires were included in the final data analysis • 47% reported using BZD with/without a prescription • 25% said that their initial use began with a prescription • 54% did not start using BZD until after entering the methadone program © 2014 Community Care Behavioral Health Organization 7 Benzodiazepine Use and Misuse • Among patients in a methadone program the main reasons given for using BZD without a prescription: – Curiosity – To relieve tension or anxiety – To feel good – To get high – To overcome depression or frustration © 2014 Community Care Behavioral Health Organization 8 Benzodiazepine Use and Misuse • When asked patients in a methadone program if they would consider reducing or stopping the use of BZD if the methadone program could provide help that would work: – 40% said “Yes, definitely” – 7% said “Maybe” – 19% said “No” – 33% had already stopped using BZD © 2014 Community Care Behavioral Health Organization 9 Benzodiazepine Use • Among Community Care Medicaid enrollees: – Analysis includes data for 39 Community Care counties – Number of unique members per year filling benzodiazepines – Benzodiazepine use very low among children and adolescents – Adult benzodiazepine Use ranges from 13-24% of Medicaid enrollment among Community Care counties © 2014 Community Care Behavioral Health Organization 10 Opiate Use • Among Community Care Medicaid enrollees: – Analysis includes data for 39 Community Care counties – Number of unique members per year filling four or more opiate scripts – Opiate use very low among children and adolescents – Adult opiate use ranges from 11-21% of Medicaid enrollment among Community Care counties © 2014 Community Care Behavioral Health Organization 11 A Quality Improvement Initiative Between Counties, Methadone Providers, and Community Care Community Care Methadone Provider Initiative © 2014 Community Care Behavioral Health Organization Objective • To identify members enrolled in methadone treatment programs who are concurrently filling benzodiazepine and /or opiate prescriptions • Collaborate with methadone providers to reduce the incidence of concurrent utilization and ultimately improve care © 2014 Community Care Behavioral Health Organization 13 Intervention • Community Care generates member reports on a monthly basis and sends to the methadone providers in Allegheny County • Member report includes medications filled and prescriber information • Methadone provider uses the information to help address any clinical issues with the member © 2014 Community Care Behavioral Health Organization 14 Frequency of Benzodiazepine Use Frequency of benzodiazepine use among members in methadone programs in Allegheny County Time period # of members with at least 10 # of members in methadone days of methadone + 1 Rx of for at least 10 days (den) Benzo (num) Percent (num/den) 2009-Q4 1462 524 35.8% 2010-Q2 1424 509 35.7% 2010-Q4 1463 536 36.6% 2011-Q2 1473 486 33.0% 2011-Q4 1512 503 33.3% 2012-Q2 1529 502 32.8% 2012-Q4 1523 469 30.8% 2013-Q2 1516 424 28.0% 2013-Q4 1479 384 26.0% © 2014 Community Care Behavioral Health Organization 15 Frequency of Opiate Use Frequency of opiate use among members in methadone programs in Allegheny County # of members in methadone Time period for at least 10 days (den) # of members with at least 10 days of methadone + 1 Rx of opiate (num) Percent (num/den) 2009-Q4 1462 436 29.8% 2010-Q2 1424 377 26.5% 2010-Q4 1463 387 26.5% 2011-Q2 1473 381 25.9% 2011-Q4 1512 348 23.0% 2012-Q2 1529 377 24.7% 2012-Q4 1523 328 21.5% 2013-Q2 1516 267 17.6% 2013-Q4 1479 262 17.7% © 2014 Community Care Behavioral Health Organization 16 Assessing Impact of Interventions Pre Intervention Metrics May-June 2012 (N = 636) • Members with at least 10 days of Methadone Claims = 636 22.00% 17.80% B only © 2014 Community Care Behavioral Health Organization 60.20% B+O O only 17 Assessing Impact of Interventions Post Intervention Metrics May-June 2013 (N = 485) • Members with at least 10 days of Methadone Claims = 485 40.60% 40.60% 7.40% 11.30% © 2014 Community Care Behavioral Health Organization B only B+O O only No B + No O 18 Comparison Pre-Period (May-June 2012) Post-Period (May-June 2013) Members on Benzodiazepines Only 60.2% 40.6% Members on Opiates Only 22.0% 7.4% Members on Both Medications 17.8% 11.3% Members on No Medications © 2014 Community Care Behavioral Health Organization 40.6% 19 Conclusions • The decrease in concurrent medication over the past four years is encouraging • Provider feedback has been very positive about this initiative • Providers have adopted new policies when caring for individuals on concurrent benzodiazepines or opiates to ensure appropriate use © 2014 Community Care Behavioral Health Organization 20 Collaboration of Care Implementation Guideline Presented by: Sara Remaley, MSPC, CAADC, Clinical Supervisor WPIC NATP Valerie Gualazzi, MS, CADC, Program Director WPIC NATP Western Psychiatric Institute and Clinic Western Psychiatric Institute and Clinic Narcotic Addiction Treatment Program (NATP) -Addiction Medicine Services • WPIC NATP is a clinic specializing in opioid dependency in addition to psychiatric comorbidity. • WPIC offers methadone maintenance treamtent, suboxone treatment, psychiatric care and medication management, mental health, and addiction therapy. • WPIC currently treats approximately 420 patients on a regular basis. 22 Rationale • NATP recognized a need to address the misuse and abuse of prescription benzodiazepines by patients enrolled in medication assisted treatment. • High rates of patients were enrolling in treatment and concurrently becoming addicted to and abusing benzodiazepines, posing health risks, adverse effects, and ultimately untimely discharge from treatment. Collaboration of Care • 2012- WPIC NATP redesigned the program’s philosophy and position regarding concurrent use and abuse of prescription benzodiazepines and opiates while taking methadone. • Contraindications and potential for adverse effects helped NATP move in the direction of ‘therapeutic no tolerance’. • The “Collaboration of Care” Procedure : indicating NATP’s willingness to work with patients currently on prescription benzodiazepines to taper off and receive evidence based interventions and seek alternative treatment options as needed. Collaboration of Care • The Collaboration of Care Procedure was developed as a way to inform patients of the new treatment philosophy indicating: use of benzodiazepines and opiates while on methadone is no longer permissible. • With the understanding that tapering from these type of medication can be a difficult and lengthy process with potential for relapse, NATP developed a procedural guideline to assist both patients and staff through this new process. 26 Barriers to addressing bzd use: • Difficult tapering process, risk related to withdrawal symptoms, and potential need for medically supervised detoxification. • High Relapse rates with benzodiazepines. • Concurrent rates of psychiatric comorbidity and the need to address/treat underlying mental health conditions. • Collaborating with providers (prescribing physicians) vs. illicit street use. • Addressing diversion…How does this fit? 27 Let the collaboration begin…. • Step 1: Staff Education – Development of Procedural Guideline highlighting philosophy, procedures and interventions, and processes for team to follow. • Step 2: Patient Education – An FAQ was developed and handed out to all patients indicating the new Collaboration of Care and Program Philosophy regarding Concurrent use of benzodiazepines while in treatment. 28 FAQ 29 • Step 3: Patient Acknowledgement and Responsibilities: – Reviewing the new philosophy and Collaboration of Care with patients, and asking them to acknowledge with their signatures that they have been informed. – A part of this process is also to explain to patients, the risks, as well as their rights. Albeit patients may reserve the right to refuse collaboration, they are also informed how this may directly impact their ability to remain in treatment. • Step 4: Interventions – Once the Collaboration of Care is initiated, the following procedures /interventions may be followed: • Urine Drug Screens and CCBHO Report reviewed. • Contact with the prescribing physician (physician to physician) to discuss recommendations and to create a tapering regimen. – Pill Counts • Illicit Street Use: Assessing need for medically supervised detoxification. Resources: Mercy Hospital Emergency Room, WPIC DEC (Diagnostic Evaluation Center). • UDS Confirmatory tests to determine if “levels” are decreasing- indicating progress/regression. • Interventions Continued: • Assessing underlying mental health and psychiatric disorders such as anxiety, depression, mood disorder, bipolar disorder, etc. Choosing a modality to effectively work with and treat these disorders in addition to addiction. – CBT, REBT, Gestalt Therapy, DBT, Motivational Interviewing, Person Centered etc. • Modifying treatment plans: Increasing therapy, regular appointments with Psychiatrist, following a medication regimen, ongoing collaboration. • Maintaining focus on individualized care through individualized recommendations. Assessing Progress: How is this done? Regular team meetings and supervision. Response to Interventions • What happened after the Collaboration of Care was initiated? – NATP experienced responses similarly associated with the Change Curve (Kubhler-Ross) • Shock, Denial, Anger, Acceptance, Integration Response to Interventions • How long did it take before a change was noticeable? – Integration took time and CONSISTENCY IS KEY • Response to change implementation included: – Compliance and Collaboration. – Increase in individual/group therapy- engagement in regular psychotherapy. – Increase in psychiatric treatment and psychopharmacology. – Exacerbation of symptoms/negative behaviors. – Increase in referrals to Higher LOC’s. – Decrease in bzd rates. – Increase in compliance/privilege status. 34 Evaluating Effectiveness • Establishing pre and post intervention baselines: – – – – – – – 35 Rates of bzd use/abuse among patients. Urine Drug Screen Results (including break-down of levels) Individualized Progress Relapse rates Decrease in attaining prescriptions. Patient Discharges Sustained abstinence Summary • Addressing concurrent use/abuse of benzodiazepines through the following steps: – – – – – – 36 Develop Program Philosophy Identify Perceived Barriers Education Staff Educate Patients Identify intervention strategies and evidenced based practices Identify pre and post intervention baseline data “Meeting Needs …..Renewing Life” Timothy H. Reese, M.D., MRO, SAP Medical Director 1425 Beaver Avenue Pittsburgh, PA 15233 Phone: 412-322-8415 Ext. 109 Fax: 412-322-9224/421-322-3352 “Decreasing the use of prescription opiates and benzodiazepines among individuals Enrolled in methadone programs” HISTORY OF TADISO ESTABLISHED IN 1968 AS NON-PROFIT 700 PATIENTS—24 FULL TIME COUNSELORS—1 MEDICAL DIRECTOR 1 PA. POPULATION: 2/3 NON-HISPANIC WHITE AND 1/3 AFRO-AMERICAN AND OTHER DEMOGRAPHICS NON-HISPANIC WHITES 20-44 YEARS…….FASTEST NON-HISPANIC WHITES 20-34 YEARS………FASTEST OF THE FAST NON-HISPANIC WHITES 20-34 YEARS………SHOOTING MORE NON-HISPANIC WHITES 20-44 YEARS……….INHALING MORE PENNSYLVANIA 2008-2012 PERSONS ENROLLED IN SUBSTANCE ABUSE TREATMENT PROGRAMS WHICH PRESCRIBED METHADONE INCREASED 18.9% MESSAGE WE ARE IN THE MIDST OF AN EPIDEMIC OF OPIOID ADDICTION AND ITS DEVASTATING TOLL ON SOCIETY! METHADONE IS AND CAN BE AN EVEN GREATER PART OF OUR ARSENAL AGAINST THIS DEADLY FOE! PATHOPHYSIOLOGY OF OPIOID ADDICTION --MEDULLA LOCUS CAERULEUS---90% OF CATECHOLAMINES IN CNS --RESPONSIBLE FOR THE VEGETATIVE FUNCTIONS OF THE ORGANISM (SUPPORT LIFE) --THERMOSTAT ANALOGY AND THE OPIOID WITHDRAWAL SYNDROME CLINICAL MANIFESTATIONS OF OPIOID WITHDRAWAL VITAL SIGNS: TACHYCARDIA HYPERTENSION FEVER CLINICAL MANIFESTATIONS OF OPIOID WITHDRAWAL CENTRAL NERVOUS SYSTEM: RESTLESSNESS IRRITABILITY INSOMNIA CRAVING YAWNING CLINICAL MANIFESTATIONS OF OPIOID WITHDRAWAL MUCOCTANEOUS: RHINORRHEA EYES: LACRIMATION PUPIL DILATION SKIN: PILOERECTION (GOOSEFLESH) CLINICAL MANIFESTATIONS OF OPIOID WITHDRAWAL GASTROINTESTINAL TRACT: NAUSEA VOMITING DIARRHEA CLINICAL MANIFESTATIONS OF OPIOID WITHDRAWAL I. PSYCHOSOMATIC WITHDRAWAL? II. PSEUDO-WITHDRAWAL? III. REAL WITHDRAWAL? CLINICAL MANIFESTATIONS OF OPIOID WITHDRAWAL *ACCIDENTAL OVERDOSE AFTER A SUCCESSFUL DETOXIFICATION* CLINCAL MANIFESTATIONS OF OPIOID WITHDRAWAL MU-AGONIST EFFECT WITH BEGINNERS! DOPAMINE ----VTA/NUCLEUS ACCUMBENS (FOREBRAIN) DRUG ABUSE DUMPS MASSIVE AMOUNTS OF DOPAMINE INTO THIS AREA. REINFORCES BEHAVIOUR THAT IS PARAMOUNT TO SURVIVAL OF THE SPECIES UP-REGULATION OF DOPANINERGIC NEURONS --AFTER REPEATED EXPOSURE (DRUG ABUSE) TO THESE MASSIVE AMOUNTS OF DOPAMINE THE TARGET NEURONS BECOME PROGRESSIVELY LESS RESPONSIVE! NET RESULT MORE STIMULATION GIVE LESS RESPONSE THUS PROPELLING THE ADDICTION PROCESS! BENZODIAZEPINES INTERNEURONS IN THE VTA APPLY INHIBITORY EFFECTS ON DOPAMINERGIC NEURONS THESE INHIBITORY INTERNEURONS EXERT THEIR EFFECT ON THE DOPAMINERGIC NEURONS BY WAY OF GABA (GAMMA AMINO BUTYRIC ACID) BENZODIAZEPINES INHIBIT THIS INHIBITORY EFFECT. THIS INHIBITION RESULTS IN A MASSIVE RELEASE OF DOPAMINE FROM THE DOPAMINERGIC NEURONS. THIS IS THE SYNERGISM WHICH OCCURS WHEN BENZODIAZEPINES ARE GIVEN WITH AN OPIOID; E.G., METHADONE. OPIOIDS IN A STABILIZED METHADONE PATIENT ANY ADDITIONAL OPIOID WILL CAUSE DESTABLIZATION ; IF THE OPIOIDS ARE TAKEN TO AN ANALGESIC LEVEL ONLY THE DESTABILIZATION WILL MAINLY AFFECT THE MEDULLA LOCUS CAERULEUS. IF THE OPIOIDS ARE TAKEN TO THE EUPHORIC LEVEL THE DESTABILIZATION WILL AFFECT THE DOPAMINERGIC NEURONS AS WELL. CLONIDINE IN SEARCH OF DOPAMINE SINCE THE OPIOID WITHDRAWAL SYNDROME IS DUE IN PART TO HYPERACTIVITY OF THE MEDULLA LOCUS CAERULEUS AND EXCESSIVE CATECHOLAMINES, A DRUG WHICH BLOCKS THIS EFFECT SHOULD TREAT THIS PART OF THE OPIOID WITHDRAWAL SYNDROME. CLONIDINE( CATAPRESS) IS A CENTRALLY ACTING ALPHA-2 BLOCKER AND DOES THIS WELL. WHAT ABOUT THE DOPAMINE DEFICIENCY? A BENZODIAZEPINE WAS NEEDED TO BE ADDED TO THE ABOVE REGIMEN TO MAKE THE TREATMENT PALABLE TO THE PATIENT. THIS BENZODIAZEPINE VIA INHIBITING GABA IN INTERNEURONS OF THE VTA SUPPLIED THE DOPAMINE. REPRESENTATIVE VIGNETTES A. DR. COMPLETELY COOPERATIVE—MOST COMMON SCENARIO B. DR. COOPERATIVE BUT DILATORY---NEEDS SOME PRODING C. DR. COOPERATIVE BUT SELECTIVE---”NOT TO YOUR PATIENT” D. DR. COOPERTIVE BUT NOT REALLY---REDUCE BUT WON’T STOP! CCBHO INITIATIVE THE EXPRESSED PURPOSE OF THIS INITIATIVE WAS TO DECREASE THE USE OF BENZODIAZEPINES AND OPIOIDS IN METHADONE CENTERS….AND IT WORKED! CCBHO GIVES THE METHADONE CLINICS A LISTING OF PATIENTS WHO ARE GETTING BENZODIAZEPINE AND/OR OPIOID SCRIPTS. THESE PRESCRIPTIONS WOULD NOT BE REGISTERED AT THE CLINIC NOR WOULD EVIDENCE OF THE DRUGS SHOW IN THE ROUTINE URINES. CCBHO INITIATIVE THIS SCENARIO WAS VIRTUALLY UNCHANGED. DOCTOR TO DOCTOR COMMUNICATION SPOILED THE ENTERPRISE. IN CONCLUSION, THE INTERVENTIONS I HAVE DESCRIBED WITH THE ASSISTANCE OF CCHBO DID AND CONTINUES TO MAKE A DIFFERENCE FOR THE BETTERMENT OF THE LIVES OF THE PATIENTS AT TADISO.