File
advertisement

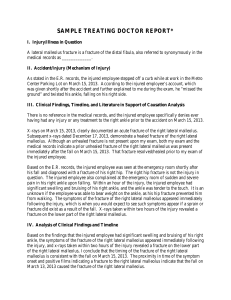
Potts Fracture By: Micah Shore 7/14/13 AT 4810 Dr. Jordan Utley Potts Fracture Section 1: Introduction to the Pathology Incidence of the Pathology A Pott’s fracture happens most frequently to athletes and those who have to land on one leg, such as a football player landing after making a catch or a dancer landing a jump. They are most commonly found along with severe ankle sprains and usually happen together. A shear force directly hitting the malleolus can also cause a fracture. You are more likely to fracture the lateral head due to the better stability and durability of the medial bone and ligaments. Of all the ankle injuries evaluated, only 15% are ankle fractures. The frequency of ankle fractures has been increasing for the past 20 years, and the rate is approximately 187 in 100,000 person-years (Iskyan, Kara, 2012). Etiology During certain activities such as landing from a jump, or when rolling an ankle, stress is placed on the tibia and fibula causing either of the malleolus to crack or break (Pott's Fracture, 2013). Because of the large forces required to break the tibia or fibula, a Pott's fracture often occurs in combination with other injuries such as a sprained ankle or other fractures of the foot, ankle or lower leg. Along with any other kind of fracture there are different degrees of severity and areas on the bone that can be fractured. <Photo #1> Section 2: Anatomy and Physiology Anatomy The lateral malleolus of the fibula and medial malleolus of the tibia are the main bones that can be fractured in this pathology. The distal heads of the fibula and tibia form the mortise for the ankle, which are called the malleolus’s. The talus, which sits in between the two heads can also be bruised or damaged in the process. The ligaments involved can be either the anterior talofibular, posterior talofibular, and calcanofibular on the lateral side or any one of the deltoid ligaments on the medial side. Physiology When a severe ankle sprain happens the ligaments tear and may bring a piece of the bone with them causing an avulsion fracture. The bone hitting the ground from spraining the ankle so bad will crack the head of the fibula or tibia as well. Any crushing blow to the lower leg also has the ability to fracture the distal heads of either bone (Jenn F, 2012). All of these instances happen very quickly causing tremendous stress on the bone at once. <Photo #2> Section 3: Evaluation of the Injury Signs and Symptoms Patients with a Pott's fracture typically experience a sudden onset of sharp, intense ankle or lower leg pain at the time of injury. An audible sound, such as a "crack" or "snap", may also be heard. The patient will limp to avoid pain created from weight being placed on the foot. In cases of the medial malleolus being fractured the patient may not be able to put an kind of pressure on the foot since the tibia is the main weight bearing bone. Initially it is extremely painful but subsides to a dull pain after some time of resting. Pain can be expected on the lateral, medial, or posterior sides of the ankle along with bruising and swelling. An obvious deformity may be present in severe cases and certain movements will elicit pain as well. Special Tests: Defining Practice Evaluation A special test for a Pott’s fracture will be pain during talar tilt, where the ankle is inverted and everted causing the talus to knock against the medial or lateral malleolus (Starkey, Chad, 2010) . <Photo #3> Along with the special test, the malleolus with be tender to the touch and the ankle will have limited movement. A bump test can also be administered, which is simply lightly hitting the bottom of the heel with the palm of your hand and will elicit some pain if it is a positive test (Starkey, Chad, 2010). Section 4: Associated differential diagnoses A lateral or medial ankle sprain can be mistaken instead of a fracture since they go hand in hand. When there is a fracture there is also a sprained or torn ligament. You can rule out a sprain by performing the special tests for a fracture as well as palpating the malleolus for tenderness and pain (Jenn F, 2012). A sprain will elicit dull pain unless walked on but even then the pain is not as strong as if it were broken. In fact for some fractures no pressure can be placed on that foot at all. Section 5: Prognosis & Recent Evidence Informing Best Clinical Care Prognosis Depending on how bad the fracture is surgery may be needed to put the bone back together. After surgery a boot or cast needs to be worn as well as the use of crutches. There is a slow transition from the cast or boot to a brace and taped ankle for a number of weeks. Follow up x-rays are taken until the bone is fully healed. After that, Physical therapy is needed throughout the recovery process where stretching and progressive strengthening exercises are performed weekly until the patient can return to play (Iskyan, Kara, 2012). Recent Research There is really no new research on the diagnosis and treatment of a Pott’s fracture that I haven’t already listed above.