2015 03 04 Thames Valley Clinical network event – Catherine

Oxfordshire
Clinical Commissioning Group
Using an outcomes based contracting approach to improve the care of older people
Oxfordshire CCG’s approach to contracting for outcomes
Oxfordshire
Clinical Commissioning Group
This presentation
Why an outcomes based contract?
Outcomes
Approach to procurement
Outcomes and Indicators
Service Scope
Service Model
Incentivization
Oxfordshire
Clinical Commissioning Group
The case for outcomes based contracting
Current commissioning converts money into activity, not outcomes
Incentives are not aligned to maximise benefit across the patient pathway
Current approach is financially unsustainable
If we are serious about integration we need a different approach to commissioning
Oxfordshire
Clinical Commissioning Group
How is an OBC contract different?
It aligns commercial arrangements to deliver outcomes for patients
It can deliver the optimum VFM service for patients and tax payers as commissioners will seek to pay out incentives to reward excellence
It supports integration through the inclusion of all relevant providers that jointly will need to achieve outcomes
It supports collaborative approaches through gain share arrangements to share financial savings between providers and commissioners
It provides a change mechanism for improvement and refinement
It creates stability for providers (and patients) and sets the pace of change over a longer-term contract
It remains an NHS standard contract!
Oxfordshire
Clinical Commissioning Group
Approach to procurement
Integration central to approach
Services in scope provided by two main NHS providers
Providers had begun to work more closely together
Asked the two providers to work together and provide a single response
Achieved “most capable provider” designation
Contract negotiation to commence
Oxfordshire
Clinical Commissioning Group
So-what outcomes will drive individual and system change?
Oxfordshire
Clinical Commissioning Group
Outcomes and indicators
Outcome Example Indicators
I want to be helped to be healthy and active
I want to be helped to be as independent as possible in the best place for me
When I am in need of care it is safe and effective
I want to have a good experience and be treated with respect and dignity
% with fragility fracture who recover to previous level of functioning; % with no on-going care after reablement
Proportion still at home 90 days after discharge; avoidable sight loss;
DTOC; admissions for ASC conditions
Effectiveness of community services; incidence of pressure ulcers
% who die in place of their wishes; experience of overall care
Oxfordshire
Clinical Commissioning Group
Service Scope
Non-elective admissions
Community hospitals
Community assessment and admission prevention services
Reablement services
Intermediate care beds
9
Oxfordshire
Clinical Commissioning Group
Provider Service Model proposals
1.
Unified care network
2.
Ambulatory care by default
3.
‘Specialist Generalist’ care
4.
Universal Best Practice
5.
Working with others
Transforming care for Older People in Oxfordshire
Making our health and care systems fit for an ageing population. Oliver et al. Kings Fund 2013.
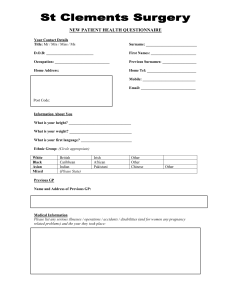
1. Unified Care Network
•
•
•
The Patient
• Frail, comorbid, vulnerable
An individual in a network
A partner in care
Therefore care must be:
• Individualised
• Comprehensive
• Coordinated
• Consistent
• Capable
• 7 day
10
Right place ‘Close to home’
We propose:
A seamless network of complex care:
•
• Community Care Hubs
– Economy of scale
– Resilience of scale
– Quality & capability of scale
• eg coprovision of physical & psychological Health
• ‘Acute site 1’
‘Community Care Hub Plus’
• Integration across multiple axes
• Virtual presence of 2
○
• Information sharing
& 3
○ capability
• Telemedicine
Evaluating integrated and community-based care. How do we know what works?
Nuffield Trust 2013
Transforming care for Older People in Oxfordshire
2. Ambulatory Care by Default
Patients Need:
• Prompt, effective, coordinated assessment and treatment
• Right place, right time
• Advanced decision-making with the patient
• Care to be safe and compassionate
11
We Propose:
The best care, closer to home.
• Infrastructure and teams adapted to outreaching care
• Re-balancing of the ‘care footprint’
• Universal ‘active interface’
– EMU, EAU, SEU, ED
• Distributed advanced care:
– diagnostics (PoCT & Radiology)
– complex treatment and monitoring: true ‘Hospital at Home’
Transforming care for Older People in Oxfordshire
Directory of Ambulatory Emergency Care for Adults,
3 rd edition. NHS Institute for Innovation. 2012
1
2
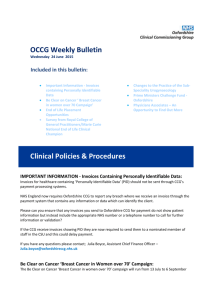
3. Specialist Generalist Care
Model of Care
Acute medicine Complex and Interface medicine
In acute hospitals
For adult patients with the most severe illness
- General Medicine
- Geriatric Medicine
- Stroke
- General Surgery
- (non-MTC) Trauma
In both
- acute hospitals
- Community Care Hubs
Longer LoS
Complex needs
Usually (very) elderly
Dementia prevalent
Risk of Harm
‘Active Interface’ capability
Embedded in all assessment units
Outreaching support to primary care delivered from Community Hubs
Advanced relationships with clinical colleagues in the acute hospitals Generalists integrated platform of holistic care.
Embedded Geriatric &
Psychological Medicine
Specialists more focused (specialised) input in some settings.
Geriatricians
Generalists
Psychological Medicine
+
‘the network’
Cohort drawn and developed from
- 1 ○ & 2 ○ care
- medical & non-medical
Future hospital: Caring for medical patients. Future Hospital Commission 2013.
Transforming care for Older People in Oxfordshire
4. Universal Best Practice to deliver the best Patient-Centred Outcomes
Patients need care that is:
• Effective
• Harm-free
• Joined-up
• Delivered in partnership
• Delivered by familiar people
We Propose:
• Promotion of self-care
• Enabling care
• Tailored multi-disciplinary care – ‘CPA’
• Zero delays
• Enhanced Recovery approach
• Capable care 24-7
• ‘Care to the patient, not patient to the care’
• Care environments that are universally frail-appropriate and dementia-appropriate
13
Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database of Systematic Reviews 2011
.
Tr ansforming care for Older People in Oxfordshire
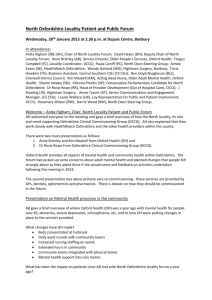
Universal Best Practice to deliver the best Patient-Centred Outcomes
An exemplar: Intermediate Care beds
Current
• Dis-integrated, isolated
• Provider-determined location
• Dated accommodation
• Weak clinical capability
• Brittle staffing
• Maximum 40 hour clinical care
• Minimal governance
• Opaque outcomes
14
Proposed:
• Integrated
• Close to home
• Purpose-built
• Scaled to optimise care
– Resilience, quality and value!
– Co-location of complementary services
• Strong clinical team
– medical, nursing, therapy, mental health
• 24-7 clinical capability
• Strong governance
• Transparent outcomes
– Benchmarked
– Quantitative and Patient-reported (PREM)
National audit of Intermediate Care 2013. NHS Benchmarking Network.
Transforming care for Older People in Oxfordshire
5. Working with Others
Primary Care needs:
• Immediate high quality advice
• Responsive outreaching home care
• Highest quality patient information
• Development of clinical capability
Social Care providers need:
• The best functional outcomes
• An accurate client prognosis
• Excellent clinical information
• Effective response to medical crises
We propose:
• Direct ‘phone access to senior clinicians
• CPA and ambulatory care
• Transformational improvement in IT
• Professional development opportunities
• CPA delivered by expert teams
• Advanced clinical network capability delivered 24-7 into the home
• Integrated Health & Social assessment
Third sector providers need:
• A meaningful role in patient care
• Support during client crisis
15
• Valuing the opportunity of their offer
• Integration into the Network of Care
• Open access to CPA and ambulatory care
Lessons from experience. Making Integrated care happen at scale and pace. Kings Fund 2013.
Transforming care for Older People in Oxfordshire
Oxfordshire
Clinical Commissioning Group
Incentivization-1
It is the commissioners intention to spend the money.
Budget c£90m
Quantum to be at risk: TBC but 15-20%
At (e.g.) 20% that equates to £18m per annum
That £18m is shared across the outcomes and specific indicators. Each point (out of
100) is worth £180,000
Oxfordshire
Clinical Commissioning Group
Incentivization-2
So-if we allocate 30% of the incentive pot to
“healthy and active”-that is worth £5.4m…
Is that enough money to drive a more proactive and preventative service model?
Phasing of incentives: what can be achieved in year 1, what needs 5+ years?
Improvements on baseline, and then for review
“bonus payment” for consistency across outcomes
Oxfordshire
Clinical Commissioning Group
Contacts
OBC Programme Lead:
Catherine Mountford catherine.mountford@oxfordshireccg.nhs.uk
Clinical Lead
Dr Barbara Batty
Barbara.batty@oxfordshireccg.nhs.uk