Radicular Syndrome
advertisement

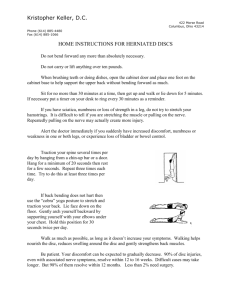
Darwin Amir Bgn Ilmu Penyakit Saraf Fakultas Kedokteran Universitas Andalas Cervical plexus Brachial plexus C1 C2 C3 C4 C4 C4 C4 C4 T1 T2 T3 T4 T5 T6 T7 T8 T9 Phrenic nerve Axillary nerve Musculocutaneous nerve Thoracic nerves T10 T11 T12 Lumbar plexus L2 L3 Sacral plexus Radial nerve L1 L4 L5 S1 S2 S3 S4 S5 Co1 Ulnar nerve Median nerve Lateral femoral cutaneous nerve Genitofemoral nerve Femoral nerve Pudendal nerve Sciatic nerve See ANS lecture Definition: a combination of changes usually seen with compromise of a spinal root within the intraspinal canal; these include neck or back pain and, in the affected root distribution dermatomal pain, parasthesia or both decreased deep tendon reflex, occasionally myotomal weakness Radicular Syndrome Arises due to compression or herniation of the nerve roots are branching of the spinal cord that transmits signals throughout the body at every level along the spine Radicular Syndrome Symptome Leads to pain and other signs like lack of sensation, tingling and a sense of weakness felt in the upper or lower regions of the body like the arms or legs Radicular Syndrome Symptomes Sensory-related symptomes are more prevalens as compared to motor-related symptomes, and muscular weakness is generally as indicator of the increased severity of nerve compression The nature and kind of pain could differ ranging from dulling, throbbing pain and complex to localize , and even sharpshooting and burning sensation could be felt Less common than somatic pain The hallmark of radiculopathy, any pathologic condition affecting the nerve roots Arises from the nerve roots or dorsal root ganglia Herniated disk is by far the most common cause Lancinating or electric quality Moves in bands and usually radiates down the limbs Associated symptoms of paresthesias are very helpful determining the identity of the involved nerve root better than site of pain Symptoms of weakness and objective findings of sensory loss, weakness and reflex loss may occur Inflammation is important as a pain mechanism: ◦ Phospholipase A and E, NO, TNF, other proinflammatory mediators are released by a herniated disk ◦ The dura surrounding the ventral and dorsal nerve root is bathed in this exudate ◦ Inflammation or prior injury to nerve root is necessary to cause compression to generate continued pain Neurapraxia: Segmental loss of myelin coating on nerve root/nerve ◦ Weakness, but no atrophy Axonotmesis: Loss of axons and myelin but at least some supporting structures are preserved ◦ Weakness and muscle atrophy if severe Neurotmesis: Loss of axons, myelin, and complete disruption of supporting structures (transection) weakness and atrophy Dermatome • Each nerve root supplies cutaneous sensation to a specific area of skin, known as a dermatome Overlaps somewhat, so won’t lose All sensation, but will feel paresthesia Myotome • If radicular pain sever could affect myotome • Each nerve root supplies motor innervation to certain muscles, known as a myotome In the cervical spine: In the lumbar spine: ◦ Nerve roots exit above their named vertebral body ◦ I.e., C7 exits below C6 and above C7-so lateral disk herniation here gets C7 ◦ Spinal cord ends at L1 or L2 ◦ Nerve roots travel long distances then exit below their named vertebral body ◦ The lumbosacral nerve roots are susceptible to injury at multiple locations ◦ T11-L1—anterior horn C7 most common Root C5 C6 C7 C8 T1 Pain (*less reliable for localization) Neck, shoulder Paresthesias/Numbness Weakness (*more reliable for localization) Lateral arm Shoulder abduction and external rotation, elbow flexion and forearm supination Neck, shoulder, Lateral forearm, thumb Shoulder abduction and external lateral arm and and index finger rotation, elbow flexion and forearm forearm, lateral supination and pronation hand Neck, shoulder, Index and middle Elbow and wrist extension, forearm middle finger, fingers, palm pronation, wrist flexion hand Shoulder, Medial forearm and Finger extension, some wrist medial forearm, hand, fourth and fifth extension, distal finger and thumb fourth and fifth digits flexion, finger abduction and digits adduction Medial arm and Medial forearm; also Thumb abduction most affected; forearm, sometimes fourth and finger abduction and adduction axillary chest fifth digits wall Reflex loss Biceps, brachioradialis Biceps, brachioradialis Triceps None None Classic presentation is to “wake up with it.” Usually no identifiable factor. ◦ Causes painful limitation of neck motion and symptoms corresponding to the affected nerve root(s) The majority of cervical herniated discs will catch the nerve root corresponding to the lower vertebral level. ◦ Ex: A C6/7 disc herniation will impinge upon the C7 root. Just as is the case with Lumbar HNP, conservative therapy is the mainstay of treatment. Surgery indicated for those that don’t improve with conservative management, or with new/progressive neurologic deficit. Stenosis – a constriction or narrowing of a duct or passage. ◦ Cervical spinal stenosis, thus, is narrowing of the spinal canal (within which lies the cervical spinal cord). This narrowing can be from any of a multitude of causes. Usually, though, this is referring to more chronic types of processes, rather than acute or sudden ones. More than half of adults older than 50 yrs. Will show significant degenerative cervical spine disease on radiography (CT/MRI)… ◦ (i.e., “Everybody has degenerative disc disease. And probably their dogs and cats too.” …however, only a fraction of these patients will actually experience any type of significant neurological symptoms. Radiculopathy – from nerve root compression. ◦ The term “radiculopathy” refers to disease of the nerve roots; LMN signs, pain/parasethesias. Myelopathy – from spinal cord compression. ◦ The term “myelopathy” refers to pathological changes of the spinal cord itself. Pain and sensory changes in the back of the head, neck, and shoulders. The goal here is to avoid missing patients who are myelopathic, because once stenosis has evolved to the point that it is compressing (and causing damage to) the spinal cord, the progression of symptoms may be variable…but it is going to progress. Clinical: Low back pain wit associated leg symptoms Positions can induce radicular symptoms Posterolateral disc pathology most common: Area where anular fibers least protected by PLL Greatest shear forces occur with forward or lateral bend Central disc pathology: Usually with LBP only without radicular symptoms, unless a large defect is present 21 low back pain world wide • Common complaint among adults • Lifetime prevalence in working population up to 80% • 60% experience functional limitation or disability • Second most common reason for work disability • Despite advances in imaging and surgical techniques LBP prevalence and its cost are relatively unchanged intervertebral disc vascular supply to the disc space from the cartilaginous endplate 1. segmental radicular artery 2. interosseous artery 3. capillary tuft 4. disc anulus Internal disruption Back Pain Causes • • • • • • de-conditioning sprain/strain spondylolithesis spondylosis facet syndrome disc herniation • • • • • • disc bulge spinal stenosis biomechanical inflammatory infection cancer ◦ Historically Bilateral sciatica Expanded to include unilateral sciatica Sudden, partial or complete loss of voluntary bladder function due to massive disc impingement on spinal nerves The frequency of daily urination is much greater than bowel evacuation, so… ◦ Presently Bladder dysfunction with a decrease in perianal sensation Symptoms ◦ Back pain ◦ Radicular pain Bilateral Unilateral ◦ Motor loss ◦ Sensory loss ◦ Urinary dysfunction Overflow incontinence Inability to void Inability to evacuate the bladder completely ◦ Decrease in perianal sensation Treatment: Urgent decompression is mandatory for prevention of irreparable / irreversible bladder damage 12 hours is the maximum time prior to irreversible changes 30 Cauda Equina Syndrome Caude equina: Begins at L2 disc space distal to conus medullare Cauda equina syndrome occur due to - Acute disc herniation - Epidural hematoma - Tumor Cauda Equina Syndrome Motor - Flaccid lower extremities - Knee and ankle jerk absent Sensory - Asymmetrical sensory loss - Saddle anasthesia - Loss of sensation arround perineum, anus & genital Cauda Equina Syndrome Autonomic - Loss of bladder and bowel funsction - Urinary retention Clinical: Up to 75 % of involvement of the spine occurs at 2 levels: L5-S1 and L4-L5 Possible factors that contribute to development: Changes with maturation in: Nutrition Disc chemistry Hormones Occupational forces Progression of disc narrowing leads to degenerative changes of bony structures, especially posterior components, leading to spondylosis 34 Clinical: Progression of spondylolysis with separation Grades assigned I-IV for level of translation Most common levels are L5-S1 (70 %) and L4-L5 (25 %) May be asymptomatic, but can result in Spondylosis DDD Radiculopathy Treatment: Medication Physical Therapy Injections Surgery 35 Clinical: Results from narrowing of spinal canal and / or neural foramina (CONGENITAL OR DEGENERATIVE) Most common complaint is leg pain limiting walking Neurogenic / Pseudoclaudication = pain in lower extremities with gait Relief can occur with: stopping activity sitting, stooping or bending forward Common are complaints of weakness and numbness of extremities Usually becomes symptomatic in 6th decade 36 Somatic back and neck pain: ◦ Often not helpful and not indicated unless the patient has risk factors for a serious underlying cause of back pain Incidence of spine abnormalities such as disk bulges/minor herniations is about 25-50% in asymptomatic people! Current techniques are not helpful in identifying the source of the somatic pain Root lesion (radiculopathy) vs entrapment neuropathy ◦ ◦ ◦ ◦ C6/7 vs carpal tunnel syndrome (med. n. at wrist) C8 vs ulnar neuropathy at the elbow L3/4 vs femoral neuropathy L5 vs peroneal n. at the fibular neck Bilateral L5-S1 radiculopathy vs early peripheral polyneuropathy Could be appropriate by EMG/NSV Please be familiar with the concepts Radiculopathy always must be distinguished from other peripheral nerve or plexus problems Root lesion (radiculopathy) vs plexus lesion ◦ ◦ ◦ ◦ C5/6 vs Upper trunk C8 vs Lower trunk L3/4 vs Lumbar plexus L5/S1 vs Sacral plexus The End TERIMA KASIH