BCA GAUTENG W2 LS1 MY contribution v1
advertisement

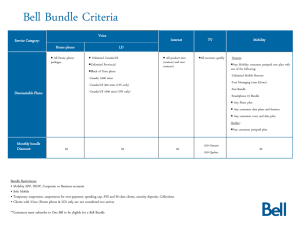
Shifting paradigms to build improvement capacity in South Africa Dr Dena van den Bergh, Chairperson BCA Dr Michele Youngleson Dr Kim Faure LAUNCH - A call to a focused and collaborative approach that leads to consistent and sustainable best practice “at the bedside” and delivers tangible, real benefits The Best Care Always Campaign.... • A unique collaborative national quality improvement campaign that involves public and private sector working together to make a bigger impact on patient care than we could each do alone. • To join the campaign, must be willing to: a) b) c) d) Implement evidence-based interventions at a faster pace; Share information, experiences and successes with others; Committed to measurement Contribute to the advancement of the campaign as a whole • Aim: to accelerate the implementation of evidence-based practice and improve patient starting with: ─ Reducing healthcare-associated infections ─ Promoting antibiotic stewardship Progress to further patient safety and improvement priorities TOTAL No. of enrolled Hospitals = now 202 in 2011 •Clinix - 6 •LHC – 48 •Medi-Clinic - 52 •Netcare - 53 •NHN – 20 •Public Sector •Gauteng- 14 •Western Cape - 9 •Free State , KZN, Limpopo Participants • Major private hospital groups ─ Clinix, Life Healthcare, Medi-Clinic, Netcare, NHN ─ Hospital Association of S Africa (HASA) • NDOH and public sector ─ Endorsement by National Dept of Health ─ Public Sector Hospitals (Gauteng, West Cape, Free State, KZN) • Professional community ─ FIDSSA, CCSSA, SASA, SpesNet, ICSSA, FPNL SATS • Partnership with Institute for Healthcare Improvement 5 Sponsors • • • • • • • • Discovery Health – Platinum Founding Janssen-Cilag - Gold Founding Media sponsor – Medical Chronicle HASA – public relations and administration Adcock Ingram Critical Care Astra-Zeneca B.Braun Fresenius Kabi 3M Aspen , J&J 6 Health sector shift •From me to we •From competition to collaboration •from secret to sharing •private –public collaboration •learning from private to public and public to private •All BCA material is open source Responsibility shift •From it doesn’t happen here to -knowing the facts •From “we already do that” to -acknowledging we may not •from passive to -active •From overwhelm to -high risk first then progressing •From can’t do - to – -if they can so can we •Accept the inevitable to -persistence •From victim of limitations to - building skills and taking on the challenge I’m sure glad the hole is not in our end! Culture shift •from punishing to •from blaming to •from who (people) to •From “spray and pray” to •From helping to -learning -curious -why (system) -support -capacitating (mentors) QA and QI •Quality assurance/audit to -QA and QI •Checklists as checking/ticklist to -checklists as aids/support •From writing more protocols -to focused interventions that improve critical elements one at a time Measurement shift •From USA data to •From numbers to •From bar graphs to •From data for centre to -SA stats -rates -run charts (over time) -frontline measures to support staff •From individual hospital to -measures across systems Methodology shift •From spray and pray to PDSA •Systems and measurement •Psychology of change •What and the how and the where •Continuous Learning system The BCA Quality Improvement approach • • • • Not just protocol Focus on the implementation gap All learn all teach Learning by doing Leadership and Doctor engagement •From “its up to clinicians/nurses” to active involvement of leadership and hospital CEOs • From ICC to EXCO •Doctors and clinical leaders •From sceptical and critical to “this might work” “it’s worth trying” to more “how can we support you” and even “I would like to initiate ...” An invitation to stretch our boundaries even further “Nobody can go back and start a new beginning, but anyone can start today and make a new ending.” Maria Robinson Everyone in healthcare really has two jobs when they come to work every day: 1. to do their work and 2. to improve it. Healthcare-associated infections are 2-3 x more common in developing countries Allegranzi B. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet Dec 2010. 18 Allegranzi B. Burden of endemic health-care-associated infection in developing countries: systematic review and metaanalysis. Lancet Dec 2010. Number of HAI studies 1995-2008 19 SA Hospitals? ─9.7% HAI point prevalence ─28.6% in ICU Private + Public Hospitals in Gauteng Prof A Duse. SA-HISC study (unpublished) 20 HAI Impact • On the patient & family • On staff • On the hospital • Financial 21 Film Partnering to Heal - computer-based, interactive learning tool about infection control practice and culture of safety. http://www.hhs.gov/ash/initiatives/hai/trainin g/ 22 CLABSI CAUTI + Antibiotic Stewardship Peripheral line infection SSI VAP 202 Hospitals enrolled at least 1 intervention 24 Closing the “Know-Do” gap 25 Accelerating change and improvement through networking and collaboration. 18 - 24 months Repeated improvement cycles: Expert Meeting and Planning Group formed Learning session 1 Repeated improvement cycles: Learning session 2 Mentoring and support © Institute for Healthcare Improvement Learning session 3 Project review exercise • Learning sessions ran May – November 2010 • Learning sessions were followed by implementation periods driven by the Plan, Do, Study, Act (PDSA) method. • No external on-site mentoring was possible • Implementation at each hospital was the responsibility of the respective teams • No formal reports or centralized data collection were undertaken. • Unexpected interruption six months into the project with no further external support available from BCA Hospital presentations Teatime What Is a Bundle? • A group of 4-5 evidence-based best practices that each individually improve care, and when done together result in much better outcomes. The science behind the bundle is so well established that it should be considered standard of care. Compliance can be measured: yes/no answers. Measuring rare events and time-between measures. I James Benneyan IHI BCA focus areas for improvement 6 infection prevention bundles • VAP (ventilator associated pneumonia) • CLABSI (central line associated bloodstream infection) • PVC • SSI (surgical site infections) • CAUTI (catheter associated urinary tract infections) (Peripheral vascular catheter associated infection) • Hand Hygiene Getting started • • • One infection prevention bundle One unit Follow the sequence from piloting to spread The Sequence for Improvement and Spread Spread Scale up Sustain Implement Pilot Robert Lloyd Mapping the Challenge Exercise On the table provided: 1. Identify the high risk units 2. Identify which bundles would apply to each unit 3. Select a priority unit and bundle to start with Mapping the Challenge ICU, High care or ward Unit 1 Unit 2 Unit 3 Unit 4 Ventilators Central lines Peripheral lines Surgical Sites Urinary Catheters Hand hygiene The challenge at your facility ICU Ventilato rs Central lines Periph eral lines Surgica l Sites Urinary Catheter s Hand Hygiene X X X X X X X X X X X X X X X X X X X X X X Theatre High Care Medical Ward Surgical Ward X X X Emergency X X X X Unit Exercise: i) Mark the procedures relevant to each of your ICU, high care units and/or wards with an ‘X’. ii) Prioritise the area of most concern in each unit and circle the appropriate ‘X’ in that unit The challenge at your facility ICU Ventilato rs Central lines Periph eral lines Surgica l Sites Urinary Catheter s Hand Hygiene X X X X X X X X X X X X X X X X X X X X X X X X Theatre High Care Medical Ward X Surgical Ward Emergency Unit X X X X Exercise: i) Mark the procedures relevant to each of your ICU, high care units and/or wards with an ‘X’. ii) Prioritise the area of most concern in each unit and circle the appropriate ‘X’ in that unit Choosing your bundle and unit Importance - impact • size of the problem • size of the impact • leadership preference Start where you’ll get the best results • the most support Start small, scale up or spread when ready ICU Ventilat ors Centr al lines Periph Surgic eral al lines Sites Urinary Cathete rs X X X X X X X X X X X X X X X Theatre High Care Medical Ward X Surgical Ward Emergency Unit X X X X X X X Mapping exercise ICU Ventilat ors Centr al lines Periph Surgic eral al lines Sites Urinary Cathete rs X X X X X X X X X X X X X X X Theatre High Care Medical Ward X Surgical Ward Emergency Unit X X X X X X X Breakout sessions 1. Bundle Content • HAI Definitions • Elements of the bundle 2. CEOs - Leading BCA Bundle Content Session • SSI – Sarie van der Westhuizen / Rita Pretorius (Mediclinic Gynaecological Hospital) • CAUTI – Annamarie Crumplin and Patricia January (Mediclinic Highveld) • CLABSI – Margaret Lidhovo (Mediclinic Morningside) • HAND HYGIENE – Karen Swart (Netcare infection control) • VAP – Amanda Jansen van Vuuren (Mediclinic Vereeniging) • Surveillance control) definitions – Lesley Devenish (Netcare infection Setting an Aim What do we want to achieve? Aim • • • • • Helps leaders think through all aspects of the project Helps select the correct processes for improvement Select the right team Keeps activities focused Empowers individuals to make changes What reduction in HAIs is possible? 1. Adult Ventilator Associated Pneumonia Average 45% reduction. With every bundle element every time – Zero cases for over long periods of time (pg 7 Getting Stared Kit) 2. Central Line Associated Blood Stream Infections Nearly eliminate CLABSI (pg 7&8 Getting Started Kit) 3. Peripheral Line Associated Infections 4. Surgical Site Infections (incidence in clean cases 2-3% USA) 40 – 60 % infections are preventable (pg 6 Getting Started Kit) 5. Catheter Associated Urinary Tract Infection Reductions of 46% - 81% have been achieved (pg 6 Getting Started Kit) Define an Aim for your HAI Statement of where you want to go you don’t need to know how to get there yet • must have a number • must have a time frame • must stretch you - not achievable in the current system - requires change • benchmark against what has been achieved elsewhere Aim To reduce ………… (VAP, CLA-BSI, PLI, SSI, CAUTI) By ……………. amount By implementing the whole ………bundle to every patient every time By May 2013 (in 18 months) Traditional approach to improvement PROBLEM EVIDENCE BASED SOLUTION PLAN “traditional” attempts to change I IMPLEMENT FAIL Closing the “Know-Do” gap 54 Overcoming the Implementation Gap SYSTEM ANALYSIS to identify barriers to care PROBLEM GREAT IDEAS PLAN IMPLEMENT I SUCCEED/ SUSTAIN ACT DO STUDY Rapid Cycle Change What are we trying to accomplish? PLAN DO ACT What can we change that will result in an improvement? STUDY PLAN DO ACT DO ACT PLAN STUDY PLAN STUDY DO ACT How will we know that a change is an improvement? STUDY Film – Maru • What is he trying to achieve? • How will he know if he has succeeded? • How many changes did he try? Model for Improvement What are we trying to accomplish? What can we change that will result in an improvement? Aim How will we know that a change is an improvement? Change Measurement PLAN DO ACT STUDY The Plan, Do, Study, Act Cycle A scientific approach to improvement PDSA starts with a theory and tests the theory Act Plan Study Do Improvement Guide, Chapter 1, p. 24, 25 Film – Making a garden • What problem did the women experience? • What was their theory about the cause of the problem? • How could a small test of change have helped? Where small tests of change would have been helpful • Endotrachael tubes in the ICU • Peripheral line insertion trays for anaethetists The theatre sisters had decided to try this ……. Chlorhexidine skin prep for peripheral IV lines….. a great idea! 62 The problems identified: The pack: • No trolley space, has to be balanced on the patient The gloves: • Aneasthetist are mostly Male - gloves are far to small for their hands • numerous complaints - “I cannot put them on without them ripping to shreds” – gloves discarded into a box for the nurses to use in non sterile procedures. • results - using non sterile gloves, or surgical gloves which triples the cost The bag: • The red bag is also saved for other waste disposal. 63 PDSA: team work and small tests of change How many doctors would have needed to test the packs to discover these problems? What could have been saved with small tests of change? - money - frustration - enthusiasm for change - time to create something effective and efficient 64 The Plan-Do-Study-Act Cycle A small bite of the elephant in 4 steps Improvement Guide, Chapter 5, p. 97 The Plan-Do-Study-Act Cycle A: Clippers ordered. Another PDSA with 6 other surgeons planned S: Was some resistance as predicted. Lack of supplies unexpected barrier. Improvement Guide, Chapter 5, p. 97 P: Ask one doctor to use clippers instead of razor with 1 patient D: Dr. M used clippers on 2 patients. Was pleased. Told staff not to put razor on his cart again! Improving many parts of the bundle/system simultaneously PLA N PLA N STU DY PLA N STU DY PLA N DO ACT STU DY Element 1 STU DY Element 2 STU DY PLA N DO ACT DO ACT STU DY PLA N STU DY PLA N DO ACT DO ACT STU DY Element 3 PLA N DO ACT STU DY PLA N DO ACT DO ACT DO ACT PLA N DO STU DY DO ACT STU DY Element 4 STU DY PLA N ACT PLA N DO ACT Progress Snapshot – PDSA Cycles Special Needs Notice TRST Research Research Cycles Blaylock Develop Blaylock Feb 18-21 2008 Bed Avail. Tool Dec 12-16 2007 Bed Avail. Tool Dec 3-4 2007 Nov 26-30 2007 Nov 19-23 2007 Patient Pamphlet PCC Tool Allied Referral Poster Feb 2008 Discharge Package Checklist Feb 2008 Discharge Package Checklist Nov 12-16 2007 Implement Risk Screening Feb 10 to Mar 5 2008 Jan 28 to Feb 10 2008 Jan. 28 to Feb 26 2008 Feb 19 -26 2008 Feb 1519 2008 Test Blaylock Jan 28 to Mar 4 2008 Bed Avail Question Jan 10 2008 Communication Source: Paula Raggiunti, Wave 6 IHI IA Program CCC Rehab Decision Tree Referral Feb 26 to Mar 4 2008 Discharge Package Checklist Jan 28 to Feb 15 2008 Discharge Lunchtime Closing the “Know-Do” gap 70 Traditional approach to improvement PROBLEM EVIDENCE BASED SOLUTION PLAN “traditional” attempts to change I IMPLEMENT FAIL Model for Improvement What are we trying to accomplish? What can we change that will result in an improvement? Aim How will we know that a change is an improvement? Change Measurement PLAN DO ACT STUDY Overcoming the Implementation Gap SYSTEM ANALYSIS to identify barriers to care PROBLEM GREAT IDEAS PLAN IMPLEMENT I SUCCEED/ SUSTAIN ACT DO STUDY Rapid Cycle Change What are we trying to accomplish? PLAN DO ACT What can we change that will result in an improvement? STUDY PLAN DO ACT DO ACT PLAN STUDY PLAN STUDY DO ACT How will we know that a change is an improvement? STUDY Model for Improvement What are we trying to accomplish? What can we change that will result in an improvement? AIM How will we know that a change is an improvement? CHANGE MEASUREMENT PLAN DO ACT STUDY Different aims and different data Research data - new knowledge DATA FOR IMPROVEMENT Data for routine monitoring 76 Measurement Outcome measure Are we getting closer to our target? Measurement Process measure (Bundle compliance) Did we use the whole bundle in every patient every time? Measurement Measuring the impact of a change Was the change an improvement? Ventilator Associated Pneumonias- Bundle Compliance and Infection Rate Mar 09 - Aug 10 14.00 100% 12.66 12.00 11.97 12.00 82% 12.35 91% 12.96 91% 91% 88% 86% 11.83 11.82 93% 92% 89% 89% 93% 92% 93% 88% 90% 80%80% 77% 10.00 71% 69% 9.78 10.01 9.94 9.17 9.06 8.61 60% 8.58 8.28 8.00 70% 7.16 50% 6.70 6.00 5.63 VAP 40% 30% 4.00 20% 2.00 10% Aug-10 Jul-10 Jun-10 May-10 Apr-10 Mar-10 Feb-10 Jan-10 Dec-09 Nov-09 Oct-09 Sep-09 Aug-09 Jul-09 Jun-09 May-09 Apr-09 0% Mar-09 - Infection Rate 80 Outcome measures How many infections did we have? – the numerator Is this better than before? I # infections – the numerator When is it a hospital acquired infection? - definitions Is it our infection? - transferred in I Overcoming Numerator Issues – diagnosing the HAI Checklists for Diagnosing the HA Infection used by the team User-friendly outcome measures Outcome measures that only need a numerator I Safety Calendar Welsh 1000 lives campaign I Developed by Annette Bartley Welsh Patient Safety Project Fill in the Welsh Calendar to show the infections September Dates of infection (CAUTI) 1/9/11 4/9/11 6/9/11 8/9/11 12/9/11 13/9/11 13/9/11 28/9/11 28/9/11 29/9/11 Welsh safety Calendar Christian Barnard Hospital Measuring HAI The concept of ‘days between’ infections Month 1 Month 2 KEY No incident New incident More than 1 incident Month 3 Numerator only 91 Days between infection September Dates of infection (CAUTI) Days between infection 1/9/11 4/9/11 3 6/9/11 2 8/9/11 2 12/9/11 4 13/9/11 1 13/9/11 0 28/9/11 15 28/9/11 0 29/9/11 1 Plot ‘Days between infection’ on the graph September Days Dates of infection (CAUTI) between infection 1/9/11 ? 4/9/11 3 6/9/11 2 8/9/11 2 12/9/11 4 13/9/11 1 13/9/11 0 28/9/11 15 28/9/11 0 29/9/11 1 Days Between Infection Sequence of Infections # Days since last infection Date of infection Measuring rare events and time-between measures. I James Benneyan IHI Outcome measures with a numerator and denominator Ratios Percentage: SSI / number of cases (Caesarian Sections) Rate: CLABSI / 1000 central line-days 97 Overcoming Denominator Issues At the same time every day the Unit manager counts devices in use in the ward Process measures Bundle compliance 99 Process measures • Overall compliance with the whole bundle – reliability – how any patients got the whole bundle every time? • Compliance with individual bundle elements 100 Measuring bundle compliance Adapted from a tool created by Dominical Hospital (Santa Cruz, CA) (IHI VAP HowtoGuide V6) 101 Measuring bundle compliance Adapted from a tool created by Dominical Hospital (Santa Cruz, CA) (IHI VAP HowtoGuide V6) 102 Individual bundle elements Know where your problem areas are 103 District Hospital VAP bundle compliance August 2011 120% 120 100 97.2 88.89 60 40 100% 72.6 80 53.6 38.9 20 0 % Compliance Percentage compliance VAP Compliance July 2011 80% 60% 40% 20% 0% HOB 30 degrees Bundle elements Sedation Vacation DVT PUD prophylaxis prophylaxis Bundle items 104 Oral hygiene Run chart for individual bundle elements Compliance with VAP bundle elements 100 80 60 40 20 0 2011 JUL AUG SEP HOB 30 degrees OCT NOV Sedation vacation DEC 2012 JAN FEB DVT prophylaxis MAR APR MAY PUD prophylaxis JUN JUL Oral Hygiene 105 Measuring bundle compliance No. receiving ALL 5 components of vent bundle = reliability of bundle compliance No. on ventilators for the day of the sample 106 Total bundle compliance Need to reach and sustain 95% compliance Knowing if you are becoming more reliable 107 The data cycle Collect Collate Display Activity Analyse interpret Act on data Share Report Outcome measure (e.g. number of infections per unit, days between infection, infection rate per 1000 device days, etc.). Select Outcome Measures: 1. Welsh Safety Cross Collate Collect 2. Days between infections 3. Infection Rate/1000 device days Display Activity 4. Other: Numerator: Denominator: Analyse interpret Act Share Report Process measures UNIT: Collate Collect BUNDLE: Process Measures: Display Activity 1. Compliance with individual bundle elements 2. Overall Compliance with Bundle Analyse interpret Act Share Report PDSA • Planning measurement systems using the model for improvement and PDSA Problem: Aim of this change: The Change: ACT: Abandon Adapt PLAN: (Who, what, where,when, how) Adopt STUDY: Prediction: DO: Measurement for this change Accelerating change and improvement through networking and collaboration. 18 - 24 months Repeated improvement cycles: Expert Meeting and Planning Group formed Learning session 1 Repeated improvement cycles: Learning session 2 Mentoring and support © Institute for Healthcare Improvement Learning session 3 Feedback forms please