Pain - MBBS Students Club
advertisement

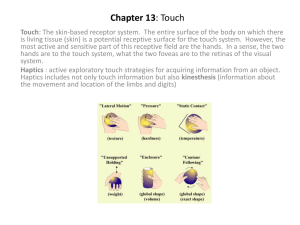
Pain is an unpleasant sensation which is a primarily protective mechanism that is meant to bring to conscious awareness that tissue damage is occurring or is about to occur. PAIN • The sensation of pain is accompanied by motivated behavioral responses (such as withdrawal or defense) as well as emotional reactions (such as crying or fear). • Also, unlike other sensations, the subjective perception of pain can be influenced by other past or present experiences (for example, heightened pain perception accompanying fear of the dentist or lowered pain perception in an injured athlete during a competitive event). • Pain is detected by pain receptors also called “Nociceptors”. • Pain is said to be a sensation and an emotion. • Adaptation to pain is poor. • Pain receptors are specific for Pain but not for the stimulus. COMPONENTS OF PAIN: 1. Nociception: the body’s detection and signaling of noxious events. 2. Pain: the conscious perception or recognition of the nociceptive stimulus, and 3. Suffering: the individual’s reaction to pain with emotional, somatic and autonomic effects along with efforts to avoid or escape pain. (This reaction differs from person to person & is influenced by age, sex, culture and personality; the reaction is also affected by the intensity & duration of pain.) TYPES OF PAIN SHARP PAIN • Also called Physiologic pain. • Quick in onset. • Felt within 0.1 sec if a pain stimulus is applied. • Sharp & pricking. Also categorized as acute pain & electric pain. • Well localized. It is not felt in many deeper tissues of the body. • E.g. needle puncturing the skin, knife cutting a skin, burn. • Conducted by A-delta fibers. DULL PAIN • • • • • • • • Also called Pathologic pain or chronic pain. It includes inflammatory and neuropathic pain. Slower in onset. Starts after 1 second of application and increases slowly over many seconds & sometimes minutes. Greater duration and less localized. It can lead to almost prolonged and unbearable suffering. It is associated with tissue destruction. Dull, aching pain, slow pain, throbbing pain, nauseous pain. It can occur in skin and deeper tissues. Conducted by C type fibers. Pain Receptors & their Stimulation • The pain receptors in the skin and other tissues are all free nerve endings. • They are widespread in: - superficial layers of the skin. - certain internal tissues, such as the periosteum, the arterial walls, the joint surfaces, and the falx and tentorium in the cranial vault. - Deeper tissues are only sparsely supplied with pain endings. • Pain can be elicited by multiple types of stimuli. They are classified as: 1. Mechanical, 2. Thermal, and 3. Chemical pain stimuli. In general, fast pain is elicited by the mechanical and thermal types of stimuli, whereas slow pain can be elicited by all three types. Pain receptors DO NOT ADAPT AT ALL or if they do, very little. 1. 2. 3. 4. Tissue Damage Tissue Ischemia Chemical substances Muscle spasm MECHANISM OF PAIN PRODUCTION 1. Tissue Damage 2. Tissue Ischemia • When a tissue does not receive the required amount of blood supply, it becomes painful in a very short time, it becomes painful in a vey short time. • Thus, if the blood supply is stopped to the upper limb by applying a tourniquet, pain appears within 3-5 minutes. If the forearm of the same limb is forced to exercise, the pain appears within 15-20 seconds. • Myocardial ischemia, Angina Pectoris and intermittent claudication are examples of pain due to tissue ischemia. Mechanism of Pain production (cont.) 3. Chemical Substances Some chemicals that excite the chemical type of pain: 1. Bradykinin 2. Histamine 3. Serotonin 4. Acetylcholine 5. Potassium ions 6. Proteolytic enzymes. Some chemicals like Substance P and Prostaglandins enhance the sensitivity of pain endings but do not excite them directly. Other chemicals may get deposited in different tissues of the body and cause pain, such as urates depositing in the synovial membranes of joints leading to gouty arthritis which is a very painful condition. 4. Muscle Spasm • When muscle spasm, the blood supply is decreased leading to decrease in oxygen supply, increased metabolites collecting at the site leading to pain. • The contracted muscle compresses its own blood vessels leading to more ischemia and more pain. • This sets up a vicious cycle or a positive feedback cycle. ASCENDING PATHWAYS ASCENDING PATHWAYS Three-neuron pathways: • Primary sensory neurons: - From external receptors - Travel through dorsal roots of spinal cord • Secondary neurons: - Make up tracts in spinal cord and brainstem • Tertiary neurons: - From thalamus to primary sensory cortex - Travel through internal capsule • For conscious perception: Spinothalamic system Medial Lemniscal system • For unconscious perception: Spinocerebellar Spino-olivary Spinotectal Spinoreticular 1. 2. Anterior Spinothalamic Pathway: Crude touch, itch, tickle & pressure Lateral Spinothalamic Pathway: Pain & temperature ANTEROLATERAL SYSTEM • • The Anterolateral system is made up of: Anterior Spinothalamic Pathway Lateral Spinothalamic Pathway The anterior spinothalamic tract carries fibers for crude touch, tickle, itch and pressure while lateral spinothalamic carries fibers for pain and temperature. • There is a double system of pain innervation in the Lateral Spinothalamic tract: 1. NEOSPINOTHALAMIC PATHWAY: For FAST pain carried by A-delta fibers 2. PALEOSPINOTHALAMIC PATHWAY: For Slow pain carried by C fibers. Because of this double system of pain innervation, a sudden painful stimulus often gives a "double" pain sensation: a fast-sharp (also called First pain) that is transmitted to the brain by the Aδ fibers, followed a second or so later by a slow (Second pain) that is transmitted by the C fibers. • The A-delta and C fibers carrying pain & temperature information from the body terminates in the dorsal horn of the spinal cord. - A-delta fibers terminate in lamina I, V and X (Lamina marginalis of the gray matter) - C fibers terminate in lamina I and II (substantia gelatinosa of the gray matter) • The distinct termination patterns of A-delta and C fibers in the spinal cord suggest that the messages are kept separate so that feel two distinct types of pain. • The primary afferent fibers for pain in the head enter the brainstem through the trigeminal nerve. The trigeminal distribution includes fibers for both the head and toothache pain. • Glutamate is the NT for the pathway for Fast pain while Substance P is the NT for the pathway for Slow pain. Even though all pain receptors are free nerve endings, these endings use two separate pathways for transmitting pain signals into the central nervous system. The two pathways mainly correspond to the two types of pain-a fast-sharp pain pathway and a slow-chronic pain pathway. ANTERIOR & LATERAL SPINOTHALAMIC TRACT Receptors (Mechanoreceptors, Thermal & Pain receptors) ↓ • Fast Pain carried by A-delta fibers (6-30 m/sec) • Slow Pain carried by Type C fibers (0.5-2 m/sec) ↓ First Order Neuron ↓ Posterior root ganglion (Cell bodies) ↓ Fibers ascend or descend 1-2 spinal cord segments where they are called the Tracts of Lissaeur ↓ On entering the spinal cord, the pain signals take one of the two pathways: Neospinothalamic pathway --Paleospinothalamic pathway Lamina I of dorsal horn Lamina II & III of dorsal horn (Lamina marginalis) (Substantia Gelatinosa) ↓ ↓ Second order neurons Second order neurons ↓ ↓ Decussate immediately through the anterior commissure & then ascend in the anterior & lateral columns of the opposite side of the spinal cord. Ascend through the brainstem (medulla, pons & midbrain) as the Spinal Lemniscus (where fibers of Anterior & Lateral Spinothalamic tract ascend together in the lower part of medulla) ↓ Thalamus (VPL nucleus) Some fibers carrying the slow pain also relay to the Reticular area, Tectal area and Periacquiductal gray region giving rise to SPINOTECTAL and SPINORETICULAR tract ↓ Third Order neurons ↓ Somatosensory Cortex (Some fibers carrying the fibers for slow pain also terminate in the hypothalamus) THE ANTEROLATERAL PATHWAY Why you CANNOT sleep when you are in pain? • Electrical stimulation in the reticular areas of the brain stem and in the intralaminar nuclei of the thalamus, the areas where the slowsuffering type of pain terminates, has a strong arousal effect on nervous activity throughout the entire brain. In fact, these two areas constitute part of the brain's principal "arousal system." This explains why it is almost impossible for a person to sleep when he or she is in severe pain. What can be done when a person is suffering from intractable and severe pain? Effect of Lesion Anterior Spinothalamic Tract: • The destruction of this tract produces little if any tactile disturbances as touch is also carried in DCML. • Bilateral lesion of this tract leads to loss of sensations of crude touch, itch and tickle below the lesion. • The unilateral lesion of the tract causes loss of sensation below the level of the lesion. Lateral Spinothalamic Tract: • The bilateral section of the tract leads to total loss of pain and temperature sensations on both sides below the lesion. • The unilateral lesion causes loss of pain (analgesia) and temperature (thermoanesthesia) below the level of the lesion on the opposite side. The contralateral sensory loss extends to a level one segment below that of the lesion owing to the oblique crossing of fibers. DIFFERENCES BETWEEN DCML & ANTEROLATERAL SYSTEM DCML 1. 2. 3. 4. Large, myelinated fibers Mechanoreceptors. High velocity: upto 70 meters/ sec. Spatial orientation is highly developed. High degree of localization. 5. Transmits the sensations: • Tactile localization • Two-point discrimination • Pressure • Stereognosis • Propriception • Vibration ANTEROLATERAL SYSTEM 1. 2. 3. 4. 5. • • • • • • Small diameter, myelinated as well as unmyelinated fibers. Multiple types of receptors. Low velocity: 1-15 m/sec Poor spatial orientation. Low degree of localization. Transmits the sensations: Pain Thermal Itch Tickle Crude touch Crude pressure The fibers of this pathway convey proprioceptive impulses to the cerebellum. It has 2 divisions: 1. Anterior Spinocerebellar Tract 2. Posterior Spinocerebellar Tract THE SPINOCEREBELLAR TRACT SPINOCEREBELLAR TRACTS Anterior Spinocerebellar Tract • Proprioceptive information. • Also contains fibers from the motor pathways so that the cerebellum is kept informed about the state of the motor neuron activity. • Fibers cross over but then cross back again the cerebellar peduncles. • Terminate in the cerebellum. Posterior Spinocerebellar Tract • Uncrossed. • Carries information mainly from the muscle spindle and the tendon organs of the trunk and lower limb, regarding position and movement of individual limb muscles. • Axons enter the posterior gray column and terminate in the nucleus dorsalis (Clark’s column). • Ascend on the same side to terminate in the cerebellar cortex. • Fast conducting. PAIN SUPPRESSION “ANALGESIA” SYSTEM OF THE BRAIN • The degree to which a person reacts to pain varies tremendously. This results partly from a capability of the brain itself to suppress input of pain signals to the nervous system by activating a pain control system, called an analgesia system. • Thus, the analgesia system can block pain signals at the initial entry point to the spinal cord. ANALGESIA SYSTEM of the Brain It consists of three major components: (1) The periaqueductal gray and periventricular areas of the mesencephalon and upper pons surround the aqueduct of Sylvius and portions of the third and fourth ventricles. Neurons from these areas send signals to (2) the raphe magnus nucleus, a thin midline nucleus located in the lower pons and upper medulla, and the nucleus reticularis paragigantocellularis, located laterally in the medulla. From these nuclei, second-order signals are transmitted down the dorsolateral columns in the spinal cord to (3) a pain inhibitory complex located in the dorsal horns of the spinal cord. At this point, the analgesia signals can block the pain before it is relayed to the brain. Gate control Theory of Pain • • • • Transmission in nociceptive pathways can be interrupted by actions within the dorsal horn of the spinal cord at the site of sensory afferent transmission. This gate mechanism is operated by a balance between excitation in large and small peripheral nerve fibers. An excess of impulses in large nerve fibers results in the closure of the gate and non-production of pain; on the other hand, relative excess of impulses in small nerve fibers opens the gate and produces pain sensation. Deep and visceral pain can be decreased by applying irritating substances to the skin overlying deep structures. This is the basis of the use of the Counterirritation for the relief of deep and visceral pain. OPIOIDS • Opioids are commonly used analgesics (chemicals that relieve the pain) that can exert their effects at various places in the CNS, including the spinal cord and dorsal root ganglion. • The different opioids are: 1. Endorphins: split products of POMC, made in the Pituitary gland as well as CNS. In the CNS, they decrease perception of pain (analgesic). They are up to 30 times more analgesic than morphine. 2. Enkephalins: are synthesized in the chromaffin cells of the adrenal medulla & released with catecholamines when sympathetic nervous system is stimulated,e.g in stress. 3. Dynorphin: has been detected in the duodenum, posterior pituitary and hypothalamus. There are interneurons in the superficial region of the dorsal root ganglion where nociceptive afferents terminate. Opioid receptors (OR) are located on the terminals of nociceptive fibers and on dendrites of dorsal root horn neurons . Activation of OR results in a decrease in release of glutamate and substance P leading to reduced transmission of from nociceptive afferents. Irritation of a visceral organ frequently produces pain that is felt not at that site but in a somatic structure that may be some distance away. Such pain that is referred to a somatic structure is called Referred Pain. REFERRED PAIN REFERRED PAIN • E.g: Cardiac pain may be referred to the right arm, the abdominal region, or even the back, neck or jaw. When pain is referred, it is usually to a structure that developed from the same embryonic segment or dermatome as the structure in which the pain originates. E.g, the arm and heart have the same segmental origin. CONVERGENCE –PROJECTION THEORY: The basis for referred pain may be convergence of somatic and visceral pain fibers on the same second-order neurons in the dorsal horn that project to the thalamus & then to somatosensory cortex. HYPERALGESIA • It is an exaggerated response to a noxious stimulus. • Chemicals released at the site of injury further directly activates receptors on sensory nerve endings leading to inflammatory pain. Nociceptors become more SENSITIVE….. • There is also release of substance P and bradykinin, which can further sensitize nociceptive terminals. ALLODYNIA • • • It is a sensation of pain in response to a normal, painless stimulus. E.g. painful sensation from a warm shower when the skin is damaged by sunburn. Damaged nerve fibers undergo sprouting, so fibers from touch receptors synapse on spinal dorsal horn neurons that normally receive only nociceptive input. This explains why painless stimuli can induce pain after injury. The release of substance P and glutamate leads to excessive stimulation of NMDA receptors on spinal neurons, a term called “wind up” that leads to excessive activity of pain transmitting pathway. It is the area of the cerebral cortex that receives primary sensory impulses directly from the relay centers in thalamus. It has 3 parts: 1. Somatosensory Area –I 2. Somatosensory Area- II 3. Association Cortex The term somesthetic cortex is reserved for Somatosensory Area-I only. SOMATOSENSORY CORTEX Somatosensory cortex- I • It is also called the Primary Somesthetic area. • It comprises of area 3,1,2. • The sequence of distribution of body areas is represented by a sensory homunculus which is a small figure of a man showing the size of the various parts of the body in proportion to distribution. • Lips occupy the greatest area followed by the face and the thumb. This is because many more receptors lie in the lips than in any other part of the body. Somatosensory cortex- II • • Its function is not well known. It seems to be concerned more with the spinothalamic tract and pain sensibility. • It further elaborates the sensory input received by Somatosensory Area I. Somatosensory Association Area: • These are Brodmann’s area 5 & 7. • It receives information from area I & II and also from the visual cortex and the auditory cortex and thalamus. • This area is responsible for decoding the sensory information. • Removal of this area causes amorphosynthesis (loss of appreciation of form of objects). THE SENSORY HOMUNCULUS What happens when Area-I is damaged? • The sense of fine touch, position, stereognosis are most affected. Higher functions are lost. Crude touch is intact which shows that this is done in the thalamus. • Two-point discrimination is decreased. • Subject cannot judge the weight of an object. • Astereognosis occurs. • Fine grade changes in temperature are not appreciated. • Orientation of different body parts relative to each other is lost. (Proprioception) • Pain is least affected but is poorly localized and poorly graded. PHANTOM LIMB PAIN It is defined as pain felt by an amputee that seems to be located in the missing limb. The theory explaining it is that brain can recognize if sensory input is cut off. The area of the brain that once received input from the leg and foot now responds to stimulation of the stump, in exactly the same way it did when the limb was attached. Mirror box therapy is used for treatment of Phantom limb pain.