Antiarrhythmic Therapy
advertisement

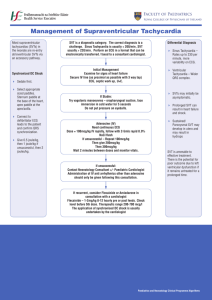
UTHSCSA Pediatric Resident Curriculum for the PICU Antiarrhythmic Therapy Antiarrhythmic Therapy Empiric Pathophysiologic Arrhythmia Diagnosis Arrhythmia Diagnosis Known or suspected mechanisms BLACK BOX Critical components Vulnerable parameters Targeted subcellular units Interventions Clinical Outcomes Interventions Clinical Outcomes Antiarrhythmic Therapy Pathophysiologic Arrhythmia Diagnosis Known or suspected mechanisms Critical components Vulnerable parameters Targeted subcellular units Interventions Clinical Outcomes AV node reentrant tachycardia AV node reentry Anatomical fast/slow pathway AV node (slow conduction) AV nodal action potential L-type Ca++ channel Ca++ channel blocker -blocker Sinus rhythm Vaughn-Williams Classification • Based on cellular properties of normal His-Purkinje cells • Classified on drug’s ability to block specific ionic currents (i.e. Na+, K+, Ca++) and beta-adrenergic receptors • Advantages: – Physiologically based – Highlights beneficial/deleterious effects of specific drugs Antiarrhythmic Therapy Empiric Arrhythmia Diagnosis BLACK BOX Interventions Clinical Outcomes Goals •Identify the type of dysrhythmia •Be familiar with more common antiarrhythmics and their Vaughn-Williams Classification Arrhythmia Types • Slow • Fast Fast wide Fast narrow Too fast Arrhythmia-focused Therapy • Fast Narrow • Supraventricular tachycardias – Re-entry type • Orthodromic SVT – Automatic • A.E.T. , Atrial Flutter • J.E.T. Arrhythmia-focused Therapy • Fast Wide – (rare) Antidromic SVT or SVT with abberancy – Ventricular tachycardia • Inappropriate automaticity of ventricular or His-Purkinje tissue Arrhythmia-focused Therapy • Select one antiarrhythmic or a limited group of antiarrhythmics to treat the disorder. Antiarrhythmic Agents Vaughn-Williams Classification • Class I - Na+ - channel blockers (direct membrane action) • Class II - Sympatholytic agents • Class III - Prolong repolarization • Class IV- Ca++ - channel blockers • Purinergic agonists • Digitalis glycosides The Action Potential 30 mV Phase 1 Phase 2 0 mV Phase 3 Phase 0 Phase 4 - 90 mV Class I Na+ Channel Blockers • IA - Quinidine/Procainamide/Disopyramide • IB - Lidocaine/Mexiletine/Phenytoin • IC - Flecainide/Propafenone/Ethmozine 1 2 Affects Phase 0 3 0 4 ERP RRP Class IA - Na+ Channel Blockers Procainamide/Quinidine/Disopyramide • Mode of action – Depress conduction and prolong refractoriness • – – – Atrial, His-Purkinje, ventricular tissue Peripheral alpha block Vagolytic Negative inotrope • ECG changes – – – Increase PR, QRS (Diso: PR > QRS ) Toxicity: QTc increases by 30% or QT > 0.5 sec Ca++ channel blockade / potent anticholinergic (Diso) Class IA - Na+ Channel Blockers Procainamide • Uses SVT (reentry) or VT – Afib/flutter (on digoxin) • Drug interactions-Decrease metabolism of Amiodarone – • Dose – – – IV: load 15 mg/kg over 1 hour, then 30-80 g/kg/min (level 5-10 ng/ml) PO: 30-70 mg/kg/day • Side effects: Lupus- in slow acetylators – ANA + : 50-90% Symptoms: 20-30 % Arrhythmia-focused Therapy • Procainamide has been a long-used intravenous • infusion for a wide range of dysrhythmias: – Narrow complex tachycardia: • Atrial tachycardia, resistant re-entrant tachycardia – Wide-complex tachycardia: • Ventricular tachycardia • Downside: • Side effects, negative inotrope, proarrhythmic Class IB Lidocaine/Mexiletine/Phenytoin • Mode of action – – – – – Little effect on normal tissues Decreases Purkinje ERP/ automaticity Increases Ventricular fibrillation threshold Depresses conduction, esp. at high rates (Mexiletine) Suppresses dig-induced delayed afterdepolarizations (Phenytoin) • ECG changes – Slight QTc (Lidocaine/Phenytoin) Class IB Lidocaine • Use: VT (acute) – Acts rapidly; no depression of contractility/AV conduction • Kinetics – t1/2 : 5-10 min (1st phase); 80-110 min (2nd phase) • Drug interactions – – Decreased metabolism w/ CHF/hepatic failure, propranolol, cimetidine Increased metabolism w/ isuprel, phenobarbital, phenytoin Class IB Lidocaine • Dose – 1 mg/kg, then 20-50 g/kg/min (level: 2-5 g/ml) • Side effects – CNS toxicity w/ levels > 5 g/ml Class IB Mexiletine • • • • Use: VT (post-op CHD) Kinetics: t1/2 = 8 - 12 hrs Drug interactions- rare Dose – 3-5 mg/kg/dose (adult 200-300mg/dose) po q 8 hrs • Side effects – – Nausea (40%) CNS - dizziness/tremor (25%) Class IB Phenytoin • Uses – VT (post-op CHD), digoxin-induced arrhythmias • Drug interactions – Coumadin- PT; Verapamil- effect (displaces from protein) • Dose – PO: 4 mg/kg q 6 hrs x 1 day, then 5-6 mg/kg/day ÷ q 12hr – IV: bolus 15 mg/kg over 1 hr; level 15-20 g/ml • Side effects – Hypotension, gingival hyperplasia, rash Arrhythmia-focused Therapy • Class IB antiarrhythmics are very effective and very safe. • Little or no effect on “normal” tissues • First line for ischemic, automatic arrhythmia's (Ventricular tachycardia) • Not a lot of effect on normal conduction tissue – not a good medicine for reentry and atrial tachycardias. Class IC Flecainide/Propafenone/Ethmozine • Mode of action – – – – – Depresses abnormal automaticity (Flec/Ethmozine) Slows conduction in AV node, AP, ventricle (Flec/Prop) Shortens repolarization (Ethmozine) Negative inotrope (Propafenone) Prolongs atrial/ventricular refractoriness (Propafenone) • ECG changes PR, QRS QTc (Propafenone) Class IC Flecainide • Uses: PJRT, AET, CAT, SVT, VT, Afib • Kinetics – t1/2 = 13 hrs (shorter if between 1-15 mos old) • Drug interactions – – Increases digoxin levels (slight) Amiodarone: increases flecainide levels Class IC Flecainide • Dose – 70-225 mg/m2/day ÷ q 8-12 hr – Level: 0.2-1.0 g/ml • Side effects – – Negative inotrope- use in normal hearts only • (NO POST-OPs) PROARRHYTHMIA - 5-12% (CAST) Arrhythmia –focused Therapy • IC’s have a lot of side effects that make them appropriate for use only by experienced providers. Class II Agents Beta-blockers • • • • • • Propranolol Atenolol Metoprolol Nadolol Esmolol d,l-Sotalol Class II Propranolol • Uses – SVT (reentry, ectopic) – Sinus tachycardia (thyrotoxicosis) – VT (exercise-induced) • Kinetics – t1/2 = 3 hrs (increased if cyanotic) • Drug interactions – Verapamil • • Hypotension Decreased LV function Class II Propranolol • Dose – PO: 2-4 mg/kg/day q 6 hrs – IV: 0.05-0.15 mg/kg • Side effects – Avoid in asthma/diabetes – CNS effects • – Nonpolar - crosses BBB BP • Suppresses renin-aldo-angiotensin axis Arrhythmia-focused Therapy • Beta-blockers are good for reentry circuits and automatic dysrhythmias. • Their effect of decreasing contractility may be limiting. Class III K+ - channel blockers • Properties – – – Prolong repolarization Prolong action potential duration Contractility is unchanged or increased • Agents – – – – Amiodarone Sotalol Bretylium N-acetyl Procainamide (NAPA) Arrhythmia-focused Therapy Can be very powerful antiarrhythmics but limited indications for first-line use – beyond the spectrum of primary care providers Amiodarone: may become a first-line medicine for a broad spectrum of arrhythmias, currently still high-risk Purinergic Agonists Adenosine • Mode of action – – – – Vagotonic Anti-adrenergic Depresses slow inward Ca++ current Increases K+ conductance (hyperpolarizes) • ECG/EP changes – Slows AV node conduction Purinergic Agonists Adenosine • Uses – – SVT- termination of reentry Aflutter- AV block for diagnosis • Kinetics – – t1/2 = < 10 secs Metabolized by RBCs and vascular endothelial cells • Dose – IV: 100-300 g/kg IV bolus Purinergic Agonists Adenosine • Drug interactions – Methylxanthines (caffeine/theophylline) • Side effects – – – – AFib/ sinus arrest/ sinus bradycardia Bronchospasm Flushing/headache Nausea • Great medicine: quick onset, quick degradation. Digoxin • Mode of action – – – Na-K ATPase inhibition Positive inotrope Vagotonic • ECG changes – – – Increases PR interval Depresses ST segment Decreases QT interval Digoxin • Use: SVT (not WPW) • Kinetics – t1/2 = preemie (61hrs), neonate (35hrs), infant (18hrs), child (37hrs), adult (35-48hrs ) • Interactions Coumadin- PT Digoxin level Quinidine, amiodarone, verapamil renal function/renal tubular excretion (Spironolactone) Worse with K+, Ca++ Digoxin Toxicity • Nausea/vomiting, lethargy, visual changes • Metabolic – – – – Hyper K+, Ca++ Hypo K+, Mg++ Hypoxemia Hypothyroidism • Proarrhythmia – – – AV block- decreased conduction SVT- increased automaticity VT- delayed afterdepolarizations Digoxin Toxicity Treatment • GI decontamination – Ipecac/lavage/charcoal w/ cathartic • Arrhythmias – – – SA node /AV node depression- Atropine; if dig > 6, may need pacing SVT- Phenytoin or -blocker VT- Lidocaine (1 mg/kg) or Phenytoin • DC Cardioversion may cause refractory VT/VF!! Proarrhythmia Torsades de Pointes • Class IA – – – Quinidine Procainamide Disopyramide 2-8% 2-3% 2-3% • Class III – – – – d,l-Sotalol d-Sotalol NAPA Amiodarone 1-5% 1-2% 3-4% < 1% Summary • SVT: Initial – – – Adenosine ?Propranolol Procainamide • SVT: Long Term – – – Nothing Propranolol Digoxin Summary • VT : Initial – Lidocaine – Procainamide • VT: Long Term – Lidocaine/Procainamide – Beta-blockers – Cardiologist 60 Cycle Interference Atrial Flutter SVT Ventricular Tachycardia Ventricular Fibrillation