RUNNING HEAD: Fite Comprehensive Clinical Case Study Fite
advertisement

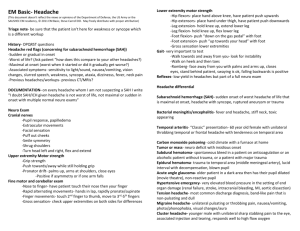
RUNNING HEAD: Fite Comprehensive Clinical Case Study Comprehensive Clinical Case Study Leah Fite Wright State University-Miami Valley College of Nursing and Health 1 Fite Comprehensive Clinical Case Study Comprehensive Clinical Case Study History and Physical Patient Information Name: S.S.; Age: 39; Race: African American; Gender: female Source Patient and electronic medical record, both reliable sources Chief Complaint “After getting home from work, I had an intense headache and became nauseous. I took some Advil and had to go lie down in my room with the lights off. Nothing seemed to make the pain get better so I called 911.” History of Present Illness S.S. is a 39 year old well developed African American female with a history of diabetes and hypertension who presented to the emergency department via life squad due to persistent, severe headache. The patient reports she came home from work and developed an intense occipital headache which radiated to her forehead. She stated it was unlike any headache she had ever had, rating it 10/10, with associated photophobia, nuchal rigidity, and nausea. The headache was unrelieved by ibuprofen or rest. She denies fever, chills, chest pain, palpitations, abdominal pain, edema, or shortness of breath. She is currently alert and oriented to person, place, time, and situation. Glascow Coma Scale (GCS) 15. Vital signs show BP 210/102 mmHg, HR 106 bpm, RR 20, O2 saturation 98% on room air, and temp 98.8 F. 2 Fite Comprehensive Clinical Case Study 3 Medical History Diabetes mellitus type II, hypertension, tension headache Surgical History Cholecystectomy Family History Father with history of diabetes and hypertension; mother with history of cerebral aneurysm at age 42 Social History The patient lives alone in an apartment on the second floor. No children. 20 pack year smoking history. She drinks alcohol socially three to four times weekly, with the last episode of drinking being two nights ago. No known history of illicit drug use. She is a server at the local restaurant, and doesn’t follow a strict diet. She does not exercise regularly. She reports that she gets the flu shot annually. Allergies No known allergies Home Medications Norvasc 10mg PO daily Metformin 500mg PO BID Multivitamin 1 tablet daily Fite Comprehensive Clinical Case Study Current Medications 0.9% NS continuous IV at 75ml/hr Labetolol continuous IV infusion (titrate to keep systolic blood pressure (SBP) 140-160 mmHg) Keppra 500mg IVPB Q12h Nimodipine 60mg PO Q4h (hold for SBP less than 120 mmHg) Heparin 5000 units subcutaneous TID Pepcid 20mg IV daily Colace 100mg PO BID Senna 1 tablet PO BID Regular insulin Q6h with low dose sliding scale Acetominophen 650mg PO Q6h prn pain or temperature above 101.5 F Dilaudid 0.5mg-1mg IV Q3h prn severe pain Odansetron 4mg-8mg IV Q6h prn nausea/vomiting Review of Systems General: Denies fever, weight gain/loss. Admits to intermittent tension headaches which she attributes to stress. Skin: Denies dermatitis, rash/itching, non-healing wounds, sores, or abscess. 4 Fite Comprehensive Clinical Case Study HEENT: 5 Denies loss of hearing, tinnitus/vertigo, earaches, sinus problems, nose bleeds, blurred vision, double vision, glaucoma, or cataracts. Admits to light sensitivity with this episode of headache Neck: Denies swollen glands or difficulty swallowing. Admits to neck pain with flexion Chest: Denies shortness of breath, cough, asthma, COPD, wheezing, tuberculosis CV: Denies chest pain, palpitations, syncope, or feet swelling GI: Admits to occasional heartburn. Admits to intense nausea associated with this headache, otherwise has no problems with nausea or vomiting. Denies abdominal pain, vomiting, diarrhea, blood in stool, or difficulty swallowing GU: Denies urinary incontinence, urinary frequency or hesitancy, denies kidney stones, blood in urine, or bladder infections M/S: Denies joint pain or swelling, gait problems Neuro: Admits to episodes of occasional mild headaches which she attributes to stress. Denies associated photophobia up until this headache episode. Denies confusion, weakness, numbness, lightheadedness, seizure, falling, or previous stroke Psych: Denies anxiety, panic attacks, depression Physical Exam General: Mild distress. Holding head in hands, requesting for lights to be turned off. Alert and oriented to person, place, and time. Cooperative with exam. Fite Comprehensive Clinical Case Study Vital Signs: 6 Temperature 98.8 F orally, HR. 106 bpm, BP. 210/102 mmHg, RR. 20 bpm, SPO2 98 % on room air. Height 5’5”, admission weight 98 kg, BMI 36 Neurological: Alert and oriented to person, place and time. Follows commands. Richmond agitation sedation score (RASS) 0. Glasgow coma score (GCS): 4/5/6. Cranial nerves II-XII intact. No focal deficits. HEENT: Normocephalic, atraumatic with no masses or lesions palpated. EOMI; No nystagmus. Pupils 3mm, equally round and reactive to light. No exudates or hemorrhage noted. Sclera white, conjunctiva pink. No papilledema on fundoscopic exam. Tympanic membranes pearly grey bilaterally without bulging or fluid, good cone of light. Nasal mucosa pink and moist, no exudates. Throat without lesions. Oral mucosa pink and moist. No pharyngeal errythema. Good dentition. Neck: Trachea midline. Neck supple. No lymphadenopathy, thyromegaly. Brisk carotid upstrokes without bruits. + menigismus. CV: Normal S1, S2. No murmurs, rubs, or gallops. No thrills, heaves, or lifts palpated. The PMI is located in the 5th intercostalspace. No jugular vein distention (JVD) or peripheral edema noted. Respiratory: Normal A/P diameter. Respirations equal and unlabored. No accessory muscle use. Lungs clear to auscultation throughout; no wheezes, rhonchi, or crackles. No dullness to percussion. No tactile fremitus. Breasts: Symmetric with no palpable masses. No nipple discharge noted. Fite Comprehensive Clinical Case Study Abdomen: 7 Soft, non-tender, non-distended, without mass and organomegaly. No guarding or rebound tenderness. Positive bowel sounds in all four quadrants. Tympanic percussion over epigastrum. No hepatosplenomegaly. G/U: Normal female. M/S: Full range of motion in all extremities, 2 + reflexes and symmetric. Extremities: No clubbing, peripheral edema or cyanosis. Brisk capillary refill. Peripheral pulses: + 2 bilateral radial, +2 bilateral femoral, +2 bilateral dorsalis pedis, and +2 posterior tibial. No femoral bruits auscultated. Skin: Normal coloration for ethnicity, warm and dry. Normal turgor. No ecchymosis, rashes or lesions noted. Mid abdominal scar noted from cholecystectomy. Nails smooth without clubbing or cyanosis. Psych: Memory, judgment, and insight intact. Mood and affect consistent with current situation. Laboratory Findings Table 1. Complete Blood Count and Renal Panel Complete Blood Count (CBC) WBC Results Normal Values Renal Panel Results Normal Values 8.7K cells/mL Sodium 137 mEq/L RBC 4.5 M cells/mL Potassium 3.6 mEq/L Hemoglobin 13.8 g/dL 3.6-10.5K cells/mL 4.4-5.8M cells/mL 13.5-16.5 g/dL Chloride 109 mEq/L Hematocrit 43% 40-50% Carbon Dioxide 29 mEq/L 135-145 mEq/L 3.6-5.1 mEq/L 101-111 mEq/L 24-36 mEq/L Fite Comprehensive Clinical Case Study MCV MCH MCHC RDW Platelet 82 fL 29 pg 36 14.5% 189 K/uL 8 82-97 fL 27-33 pg 32-36 g/dL <15.3% 140-375 K/uL BUN Creatinine Glucose 25 mg/dL 1.2 mg/dL 135 mg/dL 8-26 mg/dL 0.5-1.2 mg/dL 74-99 mg/dL Cardiac Enzymes CPK Results 128 IU/L Normal Values 0-200 IU/L CK-MB Troponin 3.2 ng/mL 0.01 ng/mL <6.1 ng/mL <0.05 ng/mL Table 2. PT/INR and Cardiac Enzymes PT/INR Results PT 11.1 seconds INR PTT 1.0 23.2 seconds Normal Values 9.0-11.4 seconds 0.8-1.2 23-32.5 seconds Other laboratory tests include drug toxicology screen, ethanol level, and urinalysis. No illicit drugs or ethanol were detected. Urinalysis revealed clear, amber urine, with a specific gravity of 1.020, with no other abnormal findings. Diagnostic Findings 12 lead electrocardiogram (ECG) shows sinus tachycardia with multiform premature ventricular complexes. Inverted T waves present in V1-V5, with large U waves and prolonged QTc interval. Chest radiography (CXR) is insignificant for acute cardiopulmonary findings, and no evidence of cardiomegaly. Noncontrast computed tomography (CT) of the head is significant for subarachnoid hemorrhage (SAH), likely from the anterior communicating artery. Differential Diagnosis Ms. S presents with severe headache with associated nuchal rigidity, photophobia, and nausea. Headache is a common complaint that can occur due to many underlying causes, Fite Comprehensive Clinical Case Study 9 therefore extensive history inquiring about onset, intensity, quality, timing, and associated symptoms is important for prompt identification and initiation of treatment. Due to the patient history and presenting symptoms, the differential diagnoses for this patient include migraine, intracranial mass, meningitis, and subarachnoid hemorrhage. Since this patient has a history of headaches, the first diagnosis to rule out is migraine. Onset of migraines typically occurs in adolescence or early adult life, and can be described as dull, pulsating or throbbing, generally lasting for several hours or longer. Family history of migraines may be significant to assist with this diagnosis; however, episodes may be triggered by alcohol, stress, sleep disturbances, menstruation, specific foods, or lights and loud noises (Aminoff & Kerchner, 2012). Associated symptoms with migraine include photophobia, nausea, vomiting, cognitive impairment, and visual disturbances including blurred vision and visual hallucinations such as sparks, flashes, or stars (Aminoff & Kerchner, 2012). Many patients learn that resting in a dark, quiet room and the use of over the counter analgesics help with acute attacks, but prescription therapy with triptans or central nervous stimulants, such as cafergot, may be needed in extreme cases (Aminoff & Kerchner, 2012). The presenting symptoms and history of headaches in this patient can point to this diagnosis, but due to the severity of the headache, CT is warranted, and migraine can be ruled out due to the presence of blood on scan. The presence of intracranial mass can produce symptoms of headaches and nausea, as well as personality changes, emotional lability, malaise, and seizures, suggestive of increased intracranial pressure (Aminoff & Kerchner, 2012). Intracranial tumors can occur at any age. Most often, the presence of intracranial mass leads to focal neurologic deficits such as progressive intellectual decline, aphasia, auditory or olfactory hallucinations, visual field loss, or sensory loss, depending on the location of the mass (Aminoff & Kerchner, 2012). The preferred Fite Comprehensive Clinical Case Study 10 method for detection of intracranial mass is MRI, however, head CT with contrast can be used (Aminoff & Kerchner, 2012). The presence of severe headache warrants immediate diagnostic testing such as CT. The lack of focal neurologic deficits and the presence of blood in the subarachnoid space with no evidence of mass found on CT can rule out this diagnosis. The presence of severe headache with associated neck stiffness and photophobia should also alert the clinician to the possibility of meningitis. The lack of fever and absence of leukocytosis can essentially rule out this diagnosis. However, since the patient presents with two of the four symptoms suggestive of meningitis, the diagnosis cannot be ruled out completely until further testing is performed. Lumbar puncture should be performed with suspected meningitis to assess fluid clarity, cell count, glucose, protein, and opening pressure (Aminoff & Kerchner, 2012). Since this patient presented with severe headache suggestive of SAH, CT was performed prior to the invasive procedure of lumbar puncture. The absence of leukocytosis or fever, in addition to the presence of blood on the CT scan can rule out the diagnosis of meningitis. The clinical presentation of subarachnoid hemorrhage is distinctive in that the onset of headache is sudden, and the quality of headache is unlike anything the patient has experienced. Associated nausea, vomiting, nuchal rigidity, and photophobia may also be present, as well as confusion or decreased level of consciousness. Risk factors for subarachnoid hemorrhage include “nonwhite” females, with a history of hypertension, diabetes, smoking, illegal drug use, family history, and high alcohol consumption (Aminoff & Kerchner, 2012; Lemonick, 2010). With these presenting symptoms, immediate CT scan should be performed to investigate the cause, since failure to obtain CT in suspected SAH can result in poor outcomes and death (Connelly et al., 2012). Urgent evaluation and treatment of suspected SAH is a class Ia Fite Comprehensive Clinical Case Study 11 recommendation due to the risk of early re-bleed and associated poor outcomes with re-bleed (Connelly et al., 2012). While trauma accounts for the most common cause of SAH, the majority of spontaneous SAH are secondary to the rupture of cerebral aneurysm originating from the anterior portion of the Circle of Willis (Lemonick, 2010). Aside from radiologic confirmation of SAH and size of aneurysm, grading of severity of bleeding is useful to assess the treatment and outcome of the patient. The Hunt and Hess scale and World Federation of Neurological Surgeons scale are both useful tools that include assessment of current patient condition and location of the aneurysm, which should be used for the management of the patient with SAH (Connelly et al., 2012; Lemonick, 2010). Once SAH is radiologically confirmed, the patient should be transferred to the neurosurgical intensive care unit for close observation and monitoring of neurologic status until intervention is able to be performed. Diagnostic tests/Rationale Electrocardiogram (EKG) While 12 lead EKG is not indicated for the diagnosis of SAH, most patients have an EKG performed upon admission to the emergency department. Many times patients with SAH also have EKG abnormalities such as arrhythmias and morphologic changes present, in addition to the classic presenting symptoms (Sommargren, 2002). Repolarization abnormalities of the ST segment, T wave, U wave, and QT segment are often associated with SAH, and are often noted as neurogenic or cerebral EKG changes, insignificant for myocardial ischemia or infarction (Sommargren, 2002). Many times these changes are resolved within five days of the Fite Comprehensive Clinical Case Study 12 hemorrhage, with the exception of the T wave inversion, which can persist for months after the diagnosis and repair. Computed Tomography (CT) In the patient with suspected SAH, the initial diagnostic test is a noncontrast head CT. In patients who present with a normal neurological assessment, but acute onset of severe headache suspicious of SAH, prompt diagnosis is important to improve survival and decrease the incidence of complications. Patients who have a noncontrast head CT performed within six hours of onset of headache, the sensitivity and specificity for detecting SAH is 100% (Perry et al., 2011). As time passes, small volumes of blood diffuse away from the bleeding source and hemolyse, thus rendering CT less able to distinguish cerebrospinal fluid (CSF) from blood, and sensitivity will decrease (Perry et al., 2011). Even within the first three days of onset of headache, noncontrast head CT remains the cornerstone of diagnosing SAH, with the sensitivity remaining above 90% for diagnosis (Connolly et al., 2012). However, at five days post aneurysm rupture, sensitivity and specificity decrease to 76% and 58%, respectively (Lemonick, 2010). Due to the increased sensitivity and ability to rapidly perform a CT, it is preferred over magnetic resonance imaging (MRI) for the diagnosis of SAH (Aminoff & Kerchner, 2012). The presence of anemia and patients with hematocrit less than 30% can decrease the sensitivity of CT, as well as technical drawbacks such as bone artifact, patient motion, or inexpert interpretation, which are limitations to CT (Lemonick, 2010). Lumbar Puncture (LP) The absence of blood on head CT cannot exclude the diagnosis of SAH, and if high suspicion remains, LP should be performed. CSF evaluation with LP is examined for the Fite Comprehensive Clinical Case Study 13 presence of xanthochromia. Traumatic tap is evident by the progressive clearing of blood in each progressive tube collected, while the presence of higher red blood cell count in the final tube is likely diagnostic of SAH (Lemonick, 2010). A yellow discoloration of the CSF, referred to as xanthochromia, may also be present and suggestive of SAH. Presence of xanthochromia usually doesn’t develop until six to twelve hours after the development of SAH, and is due to the breakdown of red blood cells in the CSF into methemoglobin, oxyhemoglobin, and bilirubin (Lemonick, 2010). The sensitivity for visual inspection of xanthochromia in the CSF is only 47%, and should not be the sole diagnostic test for ruling out SAH in suspected patients (Arora, Swadron, & Dissanayake, 2010). However, if xanthochromia is present, further testing with cerebral angiography, CT angiography (CTA), or magnetic resonance angiography (MRA) should be performed. Computed Tomographic Angiography (CTA) CTA is a noninvasive test that can be used to visualize the size and location of cerebral aneurysm that can be used for the diagnosis of SAH. This test can also be useful for preparing for interventional procedures such as surgery or coiling, as it allows better visualization of the aneurysm. However, aneurysms less than three millimeters in size may not be apparent with this test (Connelly et al., 2012). The sensitivity for detection of aneurysm by CTA is 98% with a specificity of 100% (McCormack & Hutson, 2010). Magnetic Resonance Imaging (MRI)/Magnetic Resonance Angiography (MRA) MRI is another noninvasive test that can be helpful in diagnosing SAH. The use of MRI for this purpose is limited due to the increased cost, length of time for testing, and decreased sensitivity compared to that of CT. When angiography results are negative for SAH, but high Fite Comprehensive Clinical Case Study 14 suspicion remains, MRI can be helpful in detecting small infarcts, bleeds that are several days old, or areas of multiple aneurysms, and can also be useful for detecting the lesion responsible for the bleed (Connelly et al., 2012). Although less sensitive than cerebral angiography, MRA can be useful to determine the etiology of aneurysm when angiography was inconclusive, such as arteriovenous malformation or dissection, or in patients who are unable to undergo conventional angiography (Connelly et al., 2012). MRA also carries a lower risk of stroke when compared to that of cerebral angiogram. Cerebral Angiogram Cerebral angiogram is considered the gold standard for diagnosing SAH, and for detecting arteriovenous malformations and cerebral aneurysms. Due to the invasiveness and risk of ischemic stroke associated with the procedure, cerebral angiogram is not routinely used for confirmation of SAH if diagnosed on CT, but is needed for identification of the underlying cerebral aneurysm and assessment of vasospasm (Connelly et al., 2012). Cerebral angiography has great sensitivity and specificity for detecting lethal aneurysms, can be used to reveal the bleeding source, and generally includes vertebral and bilateral carotid visualization due to the frequency of multiple aneurysms and multitude of sources that can supply arteriovenous malformations (Aminoff & Kerchner, 2012). Prioritized Plan The prioritized plan in the patient with aneurysmal SAH is focused on early recognition and diagnosis, securing the aneurysm and preventing further bleeding. The patient is admitted to the intensive care unit (ICU) for airway and cardiac monitoring, and close monitoring of blood Fite Comprehensive Clinical Case Study 15 pressure after placement of arterial line. Frequent neurologic exams every one to two hours are performed to ensure no decline in the patient condition until intervention. To prevent re-bleeding, extreme hypertension must be avoided, with a goal systolic blood pressure (SBP) of 140-160 mmHg, using a titratable agent such as labetolol (Connelly et al., 2012). Oral nimodipine should be administered to any patient with SAH to improve neurological outcomes, and decrease the incidence of cerebral vasospasm, and is a class I recommendation (Connelly et al., 2012). An anticonvulsant agent, such as keppra, is a class IIb recommendation for the immediate posthemorrhage period to decrease the incidence of seizure, which can contribute to further injury and re-bleeding (Connelly et al., 2012). Monitoring of volume status with central venous pressure (CVP) or pulmonary wedge pressure to avoid large volume of crystalloid administration to maintain the patient in a euvolemic status, as well as avoidance of fever in maintaining normothermia in the acute phase of SAH are all class IIa recommendations (Connelly et al., 2012). Tight glycemic control with goal blood glucose of 110-180 should be maintained to prevent increased risk of infection or cerebral edema. Surgical clipping or endovascular coiling as soon as possible, or at least within two days of hemorrhage, is the definitive treatment of SAH (Aminoff & Kerchner, 2012). A multidisciplinary approach to determine the best treatment option for the patient based on patient and aneurysm characteristics should be done, and include input from both neurosurgery and interventional radiology (Connelly et al., 2012). The surgical approach requires craniotomy and maneuvering of lobes to reach the aneurysm, which is sometimes difficult, in order to apply the clip at the base of the aneurysm, and carries the many risks associated with neurosurgery including infection, stroke, cerebral edema, and the risks associated with general anesthesia (Connelly et al., 2012). Endovascular coiling is the preferred method to secure the aneurysm and Fite Comprehensive Clinical Case Study 16 is associated with better long-term outcomes and less risk when compared to surgical clipping (Lemonick, 2010). Cerebral stents are used to assist in the filling of the aneurysm with coils, leading to thrombosis of the aneurysm (Aminoff & Kerchner, 2012). Due to the location of the bleed, and lack of neurologic deficits, this patient underwent endovascular coiling for the rupture of a small saccular aneurysm located in the anterior communicating artery. She was kept in the neurosurgical ICU for seven days for frequent neurologic assessments to monitor for signs of cerebral vasospasm and re-bleed. Cognitive and physical therapy was started to assist in returning the patient to pre-admission functionality. Prior to discharge, MRA was performed to assess for re-bleed, and was negative. Follow-up Patients who have experienced SAH are at an increased risk for aneurysm recurrence and re-bleeding. Once the intervention has been performed, either clipping or coiling, the patient should stay in the ICU for frequent neurologic assessments. Patients are at risk for vasospasm four to fourteen days after bleed due to the response of breakdown of products such as hemoglobin and thrombin, and can be assessed by frequent assessment of transcranial dopplers, and if clinical suspicion is high while dopplers are negative, cerebral angiogram should be repeated to document and treat the vasospasm (Aminoff & Kerchner, 2012). Management for prevention of vasospasm includes the use of nimodipine 60 PO every four hours for two to three weeks after repair (Aminoff & Kerchner, 2012). Maintaining a euvolemic status while inducing hypertension to SBP of greater than 160 mmHg with the use of vasopressors may also be needed if vasospasm occurs (Connelly et al., 20120. Once discharged, patients who undergo coiling for aneurysm rupture should follow up at three and six months after treatment with MRA, then every Fite Comprehensive Clinical Case Study 17 other year to assess for recanalization (Willinsky et al., 2009). Patients with a strong family history of cerebral aneurysm or SAH should be recommended for noninvasive outpatient screening to prevent future complications (Connelly et al., 2012). Due to the psychological consequences of SAH, such as increased fatigue, depression, anxiety, and mood and sleep disorders, a comprehensive evaluation including cognitive, behavioral, and psychosocial should be encouraged to improve quality of life (Connelly et al., 2012). Health Promotion Activities Health promotion activities in the patient with subarachnoid hemorrhage should focus on lifestyle modifications and treatment of blood pressure. To reduce the risk of repeat subarachnoid hemorrhage, treatment of hypertension is a class Ib recommendation (Connelly et al., 2012). The patient should be advised to check blood pressure readings frequently at home, and to report to her primary care physician with sustained elevated blood pressure readings. To reduce future risk, smoking and alcohol cessation is encouraged, and is also a class Ib recommendation (Connelly et al., 2012). To ensure adequate hydration, the patient should be encouraged to increase her intake of water and nonalcoholic beverages. A diet rich in vegetables may also have benefit in lowering the risk of SAH, and is a class IIb recommendation (Connelly et al., 2012). Other than restrictions on driving, activity should not be restricted after discharge, but the patient should be encouraged to monitor for increased tiredness and exhaustion. Outpatient physical therapy may be warranted to ensure maximal recovery. The patient and family should also be educated on the common symptoms of stroke. Fite Comprehensive Clinical Case Study 18 References Aminoff, M. & Kerchner, G. (2012). Nervous system disorders. In M. Papadakis & S. McPhee (Eds.), Current Medical Diagnosis and Treatment, 52nd edition (pp. 962-1037). New York: McGraw Hill. Arora, S., Swadron, S., & Dissanayake, V. (2010). Evaluating the sensitivity of visual xanthochromia in patients with subarachnoid hemorrhage. The Journal of Emergency Medicine, 39(1), 13-16. doi: 10.1016/j.jemermed.2007.09.052 Connolly, E., Rabinstein, A., Carhuapoma, J., Derdeyn, C., Dion, J., Higashida, R., &…Vespa, P. (2012). Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke, 1-39. doi: 10.1161/STR.0b013e3182587839 Lemonick, D. (2010). Subarachnoid hemorrhage: State of the art(ery). American Journal of Clinical Medicine, 7(2), 62-73. McCormack, R. & Hutson, A. (2010). Can computed tomography angiography of the brain replace lumbar puncture in the evaluation of acute-onset headache after a negative noncontrast cranial computed tomography scan? Academic Emergency Medicine, 17(4), 444-451. doi: 10.1111/j.1553-2712.2010.00694.x Perry, J., Stiell, I., Sivilotti, M., Bullard, M., Emond, M., Symington, C., &…Wells, G. (2011). Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study. British Medical Journal, 343, 1-10. doi: 10.1136/bmj.d4277 Fite Comprehensive Clinical Case Study Sommargren, C. (2002). Electrocardiographic findings in patients with subarachnoid hemorrhage. American Journal of Critical Care, 11(1), 48-56. Willinsky, R., Peltz, J., da Costa, L., Agid, R., Farb, R., & terBrugge, K. (2009). Clinical and angiographic follow-up of ruptured intracranial aneurysms treated with endovascular embolization. American Journal of Neuroradiology, 30, 1035-1040. 19