Atypical Ductal Hyperplasia - Society of Surgical Oncology
advertisement

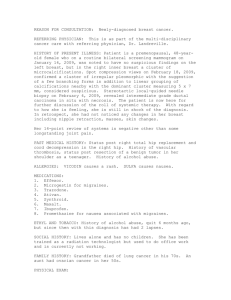
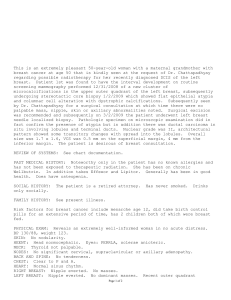
Management of High Risk and Premalignant Breast Lesions Jill R. Dietz, MD, FACS Women’s Health Institute Development of Breast Cancer Normal Duct Intraductal Hyperplasia Predict and Prevent Atypical Ductal Hyperplasia Ductal Carcinoma In Situ Invasive Ductal Carcinoma Detect and Treat Overview • Review of high risk lesions • • • • • Histology? How is the lesion identified? What is the relative risk? How is it managed? Follow up? Papilloma • Histology • If associated with dilated duct then intracystic papilloma vs non dilated sometimes called ductal adenoma • Proliferation of duct epithelium on frond-forming fibrovascular stroma • Difficult dx by cytology or frozen so excision recommended Papilloma Identified • Presents as Pathologic nipple discharge in 86% of central and 29% of peripheral lesions (where they are more commonly diagnosed as palpable mass or mammographic density) • Associated Risk • 1% of breast cancer presents as PND and less than 10 % PND is caused by cancer • Risk goes up with mammographically detected or palpable (peripheral) papillomas and with Age • Long-term RR is 2.5 to 3X Papilloma Papillomatosis • Histology • Also called epitheliosis • More consistent with micropapillary ductal hyperplasia than multiple papillomas. • A ductal hyperplastic lesion in which a fibrovascular structure supports papillary epithelial hyperplasia • May occur along side of single or multiple papillomas Papillomatosis • Identified • Pathologic nipple discharge • Mammographic density or calcifications • Associated Risk • 10% risk of cancer on excision • 3 to 4X subsequent risk Complex Sclerosing Lesions • Radial Scar (Sclerosing Lesion) • • Sclerotic center with central core of obliterated ducts, elastin deposits Corona of contracted ducts and lobules with associated proliferative lesions • Collangenous Spherulosis • Hyperplastic epithelium forms glands and acellular spherules • Less association with cancer Radial Sclerosing Lesion Identified • As a mammographically detected spiculated mass • More commonly identified in specimens of women with breast cancer • Multiple lesions in one breast not uncommon • Age over 30 and under 60 • Associated Risk • Risk is the chance of it being a cancer on excision vs RSL • Risk is the associated lesions the most common being LCIS LCIS (Lobular Carcinoma In situ) • Histology Always multiple ducts Origin from TDLU Signet-ring cells may be present Non-palpable/ no mass 50-75% of one duct involved Neoplastic cells with scant cytoplasm and small, round, bland, diploid nuclei in Type A or classical LCIS LCIS (Lobular Carcinoma In situ) Identified • Coincidentally in biopsy for proliferative lesion causing mass or mammographic abnormality • On needle biopsy of calcifications of associated sclerosing adenosis or benign calcs (LCIS rarely forms calcifications) It is not mammographically detectable • Associated Risk • 50% risk of LCIS in contralateral breast • RR 8X and absolute 17% at 15 years (ref: Page Human Pathol 1991; 22:1232-1239 Pleomorphic LCIS • Histology Type B LCIS The cells are more varied with hyperdiploid DNA with more abundant cytoplasm Difficult to differentiate b/w DCIS with intralobular spread Intracytoplasmic Mucin favors diagnosis of LCIS mucin stain may be helpful) and Signet rings are more characteristic of LCIS thann DCIS Pleomorphic LCIS Identified • Coincidentally in biopsy for proliferative lesion causing mass or mammographic abnormality • On needle biopsy of calcifications of associated sclerosing adenosis or benign calcs (LCIS rarely forms calcifications) It is not mammographically detectable • Associated Risk • Maybe difficult to differentiate from DCIS • 50% risk of LCIS in contralateral breast • RR 8X and absolute 17% at 15 years (ref: Page Human Pathol 1991; 22:1232-1239 ALH (Atypical Lobular Hyperplasia) • Histology • Same features as LCIS • Not suffieciently developed • Qualitative and quantitative factors distinguish from LCIS (< 50 to 75% of one lobule) ALH (Atypical Lobular Hyperplasia) Identified • Coincidentally in biopsy for proliferative lesion causing mass or mammographic abnormality • On needle biopsy of calcifications of associated sclerosing adenosis or benign calcs (rarely forms calcifications) • It is not mammographically detectable • Associated Risk ALH is considered a pre-malignant lesion It is associated with an increased risk of BILATERAL breast cancer 4.5-5 X more than average risk ADH (Atypical Ductal Hyperplasia) • Histology Fills some but not all criteria of DCIS About 2 mm Distinct cell borders, increased nuc/cyto ratio, nuclear enlargement, irregular chromatin or nucleoli Changes associated with proliferation. ADH (Atypical Ductal Hyperplasia) Identified • Incidentally on biopsy for benign lesion • On stereotactic biopsy of mammographic abnormality (usually indeterminant calcs) Associated Risk ADH is considered a pre-malignant lesion It is associated with an increased risk of BILATERAL breast cancer 4.5-5 X more than average risk EX: Dupont and Page: 3303 patients 2.2% NP dev Ca 4.3% with PDWA and 12.9% with atypia in 17 years American J Epidemiol 1987; 1225: 769-779 Immediate Relative Risk Risk Any Core Biopsy 2-10% 2X Subareoalar papilloma 5-10% 2-3X Distal papilloma >10% 3X Papillomatosis 10% 10-25% 13% 17% 26% 3-4X 2-5X 4-5X 8-10X 4-5X Radial Scar ALH LCIS ADH Increase in Breast Cancer Relative Risk Atypical Results Diagnosed by Cytology or Histology Confer Similar Breast Cancer Risks 25 20 FNA Cytology • Fabian, Kimler, et al 15 NAF Cytology • Wrensch, Petrakis et al 10 5.0 4.3-5.3 Histology • Dupont and Page • Dupont et al • Page et al 4.9 5 0 Atypical Hyperplasia with Atypia Hyperplasia Atypical Ductal Hyperplasia Increase in Breast Cancer Relative Risk Risks Rise in Parallel with Atypical Cells and a Family History of Breast Cancer 25 FNA Cytology • Fabian, Kimler, et al 20 18 15 10 5 5.0 4.9 4.3-5.3 11-22 NAF Cytology • Wrensch, Petrakis et al Histology • Dupont and Page • Dupont et al • Page et al 0 Atypia Atypia w/o Fam Hx Atypia + FHx Atypia with Fam Hx Cytologic Atypia is Predictive of Short-Term Outcome The percentage of women with a 10-year Gail risk > 4 developing breast cancer within 3 years: Without atypical cells: With atypical cells: 4% 15% The increase in breast cancer risk from atypical cells is independent of the Gail risk. Fabian CJ, Kimler BF, et al. J Natl Cancer Inst. 2000;92:1217-27 Management after Core Biopsy Surgical Excision • • • Borderline breast lesions: comparison of malignancy underestimation rates with 14-guage core needle biopsy versus 11-guage vacuumassisted device. Londero V, et al Eur Radiol. 2011 Jun 21(6): 1200-6. Epub 2011 Jan12 • • • All atypia diagnosed at stereotactic vacuum-assisted breast biopsy do not need surgical excision De Mascarel I, et al. Mod Pathol. 2011 May 20 (epub ahead of print) • • • Management of lobular carcinoma in-situ and atypical lobular hyperplasia of the breast – a review Hussain M, et al. Eur J Surg Oncol. 2011 Apr; 37(4): 279-89 • • • Vacuum-assisted biopsy diagnosis of atypical ductal hyperplasia and patient management Ancona A, et al. Radiol Med. 2011 Mar; 116(2): 276-91. Epub 2011 Jan 12 • • • Atypical ductal hyperplasia in directional vacuum-assisted biopsy of breast microcalcifications: considerations for surgical excision Nguyen CV, et al Ann Surg Oncol. 2011 Mar;18(3): 752-61. Epub 2010 Oct 23 • • • Identifying patients with atypical ductal hyperplasia diagnosed at core-needle biopsy who are at low risk of malignancy Albarracin CT, et al. Radiology. 2010 Dec; 257(3): 893-4; author reply 984. No abstract available. Erratum in: Radiology. 2011 Mar; 258(3): 962. Weiang, Wei (corrected to Yang, Wei). • • • Outcome of breast lesions diagnosed as lesion of uncertain malignant potential (B3) or suspicious of malignancy (B4) on needle core biopsy, including detailed review of epithelial atypia Rakha EA, et al. Histopathology. 2011 Mar;58(4): 626-32 • • • Predictors of breast cancer development in women with atypical ductal hyperplasia and atypical lobular hyperplasia Whiffen A, et al. Ann Surg Oncol. 2011 Feb; 18(2): 463-7. Epub 2010 Sep 28 • • • Flat epithelial atypia of the breast: characteristics and behaviors Sudarshan M, et al. Am J Surg. 2011 Feb; 201(2): 245-50 Epub 2010 Sep 22 • • • Incidentally detected enhancing breast lesions on chest computed tomography. Lin WC, Hsu HH, et al Korean J Radiol. 2011 Jan-Feb; 12(1): 44-51. Epub 2011 Jan 3 • • • Immediate surgical resection of residual microcalcifications after a diagnosis of pure flat epithelial atypia on core biopsy: a word of caution. Noel JC, et al. Surg Oncol. 2010 Dec; 19(4): 243-6. Epub 2009 Sep 23 • Stereotactic vacuum-assisted breast biopsy is not a therapeutic procedure even when all mammographically found calcifications are removed: analysis of 4086 procedures. Penco S, et al AJR Am J Roentgenol. 2010 Nov; 195(5): 1255-60 • • • • • • Lobular carcinoma in situ/atypical lobular hyperplasia on breast needle biopsies: does it warrant surgical excisional biopsy? A study of 27 cases O’Neil M, et al. Ann Diagn Pathol. 2010 Aug: 14(4): 251-5 • • Risk of upgrade of atypical ductal hyperplasia after stereotactic breast biopsy: effects of number of foci and complete removal of calcifications Kohr JR, et al. Radiology. 2010 Jun; 255(3): 723-30. Epub 2010 Feb 19 • • • Lobular neoplasia: morphology, biological potential and management in core biopsies O’Malley FP Mod Pathol. 2010 May; 23 Suppl 2:S14-25 • • • Clinical importance of histologic grading of lobular carcinoma in situ in breast core needle biopsy specimens: current issues and controversies Gao F, et al. Am J Clin Pathol. 2010 May; 133(5): 767-71 • • • Histology after lumpectomy in women with epithelial atypia on stereotactic vacuum-assisted breast biopsy. Graesslin O, et al. Eur J Surg Oncol. 2010 Feb; 36(2): 170-5. Epub 2009 Oct 6 • • • Flat epithelial atypia and atypical ductal hyperplasia: carcinoma underestimation rate. Ingegnoli A, et al. Breast J. 2010 Jan Feb; 16(1): 55-9. Epub 2009 Oct 13 Management: Prevention Multiple national trials have looked at chemoprevention for risk reduction Tamoxifen was found to be preventative when the contralateral breast cancer risk was halved in patients receiving Tamoxifen as treatment Breast Cancer Prevention Trial (BCPT or NSABP P-1) • 13,338 high-risk women randomized to daily tamoxifen vs. placebo for 5 years Enrollment criteria: • 60 years of age or older, or • 35-59 years old with 5-year predicted risk for breast cancer of at least 1.66%, or • a history of atypical hyperplasia or lobular carcinoma in situ Fisher B, Constantino JP, Wickerham DL, et al. J Natl Cancer Inst. 1998;90:1371-1388. Breast Cancer Prevention Trial (BCPT or NSABP P-1) Results: • Tamoxifen reduced the risk of invasive breast cancer by 49% (89 vs. 175). • Greatest risk reduction (86%) was in women with atypical ductal hyperplasia (ADH). • Tamoxifen increased the rate of endometrial cancer (36 vs. 15), stroke (38 vs. 24), pulmonary embolism (18 vs. 6), and deep-vein thrombosis (35 vs. 22). Fisher B, Constantino JP, Wickerham DL, et al. J Natl Cancer Inst. 1998;90:1371-1388. BCPT Results: Cumulative Rate of Invasive Breast Cancer Events Rate/1000 40 Placebo Tamoxifen 175 89 Rate per 1000 43.4 22.0 Placebo 30 P < 0.00001 49% reduction 20 Tamoxifen 0 1 0 0 1 2 3 4 5 Years Adapted from Fisher B, Constantion JP, Wickerham DL, et al. J Natl Cancer Inst. 1998;90:1371-1388. Breast Cancer Risk-Reduction for Tamoxifen Trials Total Breast Cancers By Group 95% CI Trial Name Placebo Tamoxifen NSABP P-11 244/6,707 124/6,681 0.51 0.39-0.66 IBIS-11 101/3,566 69/3,578 0.67 0.49-0.91 Italian2 45/2,708 34/2,700 0.75 0.48-1.18 15/702 3/702 0.18 0.05-0.62 High-risk OR 1. Chlebowski RT, Col N, Winer EP, et al. J Clin Oncol. 2002;20:3328-3343. 2. Veronesi U, Maisonneuve P, Rotmensz N. J Natl Cancer Inst. 2003:95:160-165. Why Not Just Treat All High-Risk Women With Tamoxifen? • Less than 5% of high-risk women elect to take tamoxifen when offered.1 • Tamoxifen has some serious side effects (particularly for women ≥ age 50).2 Type of event Endometrial cancer Stroke Pulmonary embolism Deep vein thrombosis 1 Port Risk Ratio (all ages) 2.53 Risk Ratio (ages ≥ 50) 4.01 1.59 3.01 1.75 3.19 1.60 1.71 ER, Montgomery LL, Heerdt AS, Borgen PI. Ann Surg Oncol. 2001;8:580-585. 2 Fisher B, Constantino JP, Wickerham DL, et al. J Natl Cancer Inst.1998;90:1371-1388. Follow up of High Risk Lesions • Is the lesion in a high risk patient? ACS definition of very high risk • Documented deleterious gene mutation in patient • Gene mutation in family/ patient untested • Therapeutic radiation to the chest (b/w age10 and 30) • Lifetime risk of 20 to 25% • Li-Fraumeni, Cowden, or Bannayan-Riley-Ruvalcaba syndromes • ADH or LCIS AND positive family history High Risk • • • • • 2 or more 1st degree relatives at young age Prior personal history of breast cancer Extremely dense breasts HRT > 10 years ADH, LCIS without family history Follow up: Surveillance • Factors to consider • • • • • • Age Breast Density Relative Risk of patient Presentation of family members Insurance Patient is part of the decision making Follow up: Surveillance • Mammography • Digital vs Analog • MRI • SBE MRI • Benefits • No ionizing radiation • Dense breasts do not interfere • High sensitivity • Limitations • Expensive • ? Lower specificity MRI • Internatioanl Breast Consortium in 2004 showed that 12% of cancers detected by mammogram or CBE were not detected by MRI (lack of neoangiogenesis) • MRI as an adjunct to mammography and BE and that a neg MRI does not overrule a palpable or mammographic finding just as a negative imaging workup does not negate the need to biopsy a palpable finding. JClin Oncol 2004; 22(suppl): 14S. American Cancer Society Guidelines for Breast Screening with MRI as an Adjunct to Mammography Debbie Saslow, PhD; Carla Boetes, MD, PhD; Wylie Burke, MD, PhD; Steven Harms, MD; Martin O. Leach, PhD; Constance D. Lehman, MD, PhD; Elizabeth Morris, MD; Etta Pisano, MD; Mitchell Schnall, MD, PhD; Stephen Sener, MD; Robert A. Smith, PhD; Ellen Warner, MD; Martin Yaffe, PhD; Kimberly S. Andrews; Christy A. Russell, MD (for the American Cancer Society Breast Cancer Advisory Group) ABSTRACT New evidence on breast Magnetic Resonance Imaging (MRI) screening has become available since the American Cancer Society (ACS) last issued guidelines for the early detection of breast cancer in 2003. A guideline panel has reviewed this evidence and developed new recommendations for women at different defined levels of risk. Screening MRI is recommended for women with an approximately 20–25% or greater lifetime risk of breast cancer, including women with a strong family history of breast or ovarian cancer and women who were treated for Hodgkin disease. There are several risk subgroups for which the available data are insufficient to recommend for or against screening, including women with a personal history of breast cancer, carcinoma in situ, atypical hyperplasia, and extremely dense breasts onmammography. Diagnostic uses of MRI were not considered to be within the scope of this review. CA Cancer J Clin 2007;57:75–89.) © American Cancer Society, Inc., 2007. American Cancer Society Guidelines for Breast Screening with MRI as an Adjunct to Mammography Literature related to breast MRI screening published between September 2002 and July 2006 was identified using MEDLINE (National Library of Medicine), bibliographies of identified articles, and unpublished manuscripts. Expert panel members reviewed and discussed data during a series of conference calls and a working meeting in August, 2006. When evidence was insufficient or lacking, the final recommendations incorporated the expert opinions of the panel members. CA Cancer J Clin 2007;57:75–89 CA Cancer J Clin 2007;57:75–89