Multicultural EvidenceBased Practice
By: Oralia Gonzalez
What is Evidence-Based Therapy
http://www.youtube.com/watch?v=nVF-IofaV9k
Evidence-Based Practice and
Multiculturalism
Acceptance is increasing
Originally focused on research-supported therapies for
specific disorders
Now broadened to include clinical expertise
Multiculturalism without strong research = empty
political value
EBT without cultural sensitivity = irrelevancy
There is still resistance and distrust
Research is limited but all mental health professions
support that treatment should be research based.
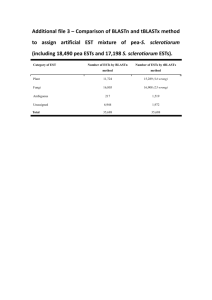
Empirically Supported Treatment (EST)
“Validated” treatments confirmed as effective for specific
disorders
Addressed issue of unintended harm from ineffective or
hazardous treatments
Specific treatment protocol for specific disorders using
manuals
Guidelines can be consulted and modified when working
with different clients
Treatment approaches should be research-based rather
than idiosyncratic, personal beliefs or sketchy theories
Guidelines to Define and Identify ESTs
1. Superiority to a control in 2 or more
methodologically rigorous, controlled studies
2. Equivalence to a well-established treatment in
several rigorous and independent controlled
studies, usually randomized controlled trials
3. Efficacy in a large series of single-case controlled designs
(e.i., within-subjects designs that systematically compare
the effects of a treatment with those of a controlled
condition)
Identified ESTs
Anxiety
Depressive and stress-related disorders
Obesity and eating disorders
Severe mental conditions such as schizophrenia and
bipolar disorders
Substance abuse and dependence
Childhood disorders
Borderline personality disorders
Examples of Empirically Supported Treatments
“Well-Established” Treatments
“Probably Efficacious” Treatments
Cognitive-behavioral therapy for panic
disorder
Cognitive therapy for obsessivecompulsive disorder (OCD)
Exposure/guided mastery for specific
phobias
Exposure treatment for posttraumatic
stress disorder (PTSD)
Cognitive therapy for depression
Brief dynamic therapy for depression
Cognitive-behavioral therapy for bulimia Brief dynamic therapy for opiate
dependence
Cognitive-behavioral relapse prevention
for cocaine dependence
Interpersonal therapy for bulimia
Behavior therapy for headache
Reminiscence therapy for geriatrics
patients
Behavior marital therapy
Emotionally focused couples therapy
American Psychological Association New
ESTs Additions
Ethnic Minorities, 1993
Women and girls, 2007
Older adults,2009
Lesbian, gay, and bisexual clients, 2012
Shortcomings of ESTs
Due to focus on choosing a treatment for a specific disorder,
contextual, cultural, and other environmental influences are not
adequately considered.
The validity for minority groups is often questionable because
they are not included in clinical trials.
Importance of therapist-client relationship is not adequately
acknowledged.
Too much emphasis is placed randomized controlled trials versus
other forms of research, such as qualitative research designs.
When treating clients with specific disorders, multicultural
therapist have had the choice to ignoring ESTs or adapting to
them.
Cultural Adaptations
Matching language, racial or ethnic
Incorporating cultural values in the specific
treatment strategies
Utilizing cultural sayings or metaphors in treatment
Considering the impact of environmental variables
Acculturation conflicts
Discrimination
Income status
Adapted ESTs Outcomes
Been successful with several minority groups
Latino/a and Haitian adolescents
Asian Americans experiencing depression
American Indians suffering from trauma
African Americans recovering from substance abuse
Most effective had the most cultural adaptations
Most effective because therapist explore the “illness
myth” of the client and the process of listening
enhances outcome
Implications
ESTs for ethnic minorities has been insufficiently researched
Challenge to select effective interventions for each individual
client
Standard ESTs
Adapted ESTs
Develop and research a culture-specific EBT
Culture-specific treatments may not be effective with a more
acculturated ethnic minority
Best approach is a research-based intervention and adapt it
to the client’s individual characteristics, values, and
preferences
Empirically Supported Relationships
American Psychological Association Division29 Psychotherapy
Task Force’s conclusions:
Makes substantial and consistent contributions to psychotherapy
outcome, independent of specific type of treatment
Acts in concert with discrete interventions, clients
characteristics, and clinician qualities in determining treatment
effectiveness
Adapting or tailoring the therapy relationship to specific client
needs and characteristics enhances the effectiveness of treatment
Practice and treatment guidelines should explicitly address
therapist behaviors and qualities that promote a facilitative
therapy relationship
Empirically Supported Relationship Variables
Demonstrated Effective
Therapeutic Alliance
Promising and Probably
Effective
Positive regard
Cohesion in group therapy
Congruence/genuineness
Empathy
Feedback
Goal consensus and
collaboration
Customizing therapy
Repair of alliance ruptures
Management of
countertransference
Self-disclosure
Therapeutic Alliance
Three elements of Conceptualization
An emotional or interpersonal bond between therapist and client
Mutual agreement on appropriate goals, emphasis on changes valued by
client
Intervention strategies or tasks that are viewed as important and
relevant by client and therapist
Core conditions of effective treatment:
Empathy, Respect, Genuineness, and Warmth
Outcome:
Clients feel understood, safe, and encouraged to disclose intimate
material
Sense of connectedness with therapist
Relational-Style Counselor Preferences of Ethnic Group Clients
Themes
African-American
Clients
Latino Clients
Non-LatinoWhite
Clients
Listening
Listen to who the client Listen in a way that
is; recognize that clients communicates “paying
are experts on
attention.”
themselves.
Listen so that the client
is comfortable enough
to talk and express
feelings
Understanding
Understand beyond
Understand feeling of
immediate impressions; clients.
understand hidden
aspects of the client.
Understand complexity
of client choices and
circumstances.
Counselor Qualities
Counselor should
“lower” self to client’s
levels; egalitarian
relationship.
Be authoritative, but
connect first, then offer
concrete advice and
solutions.
Not judge because of
social distance;
maintain professional
distance but be human.
Spending Time
Not listed as factor.
Take time to connect
deeply.
Allow time for feelings
to emerge at their own
pace.
Emotional or Interpersonal Bond
Collaborative partnership based on:
Empathy
Cognitive empathy – ability to understand the issues
facing the client
Positive regard, Genuineness, Respect, and Warmth
Self-disclosure
Controversial, may enhance the therapeutic relationship
or interfere with the therapist-client relationship
Management of Countertransference
Goal Consensus
Evidence-Based Practice and Diversity
Issues in Therapy
Requires a comprehensive understanding of the client’s background
and problem; considers best approach to provide the best outcome
Accepts research evidence from qualitative studies, clinical
observations, systematic case studies, and interventions derived in
naturalistic settings
Clinical expertise focuses on skills essential for comprehensive
assessment of the client’s problems and client strengths
Based on ongoing emphasis on client characteristics, culture, and
preferences and the importance of working collaboratively with the
client to develop goals and treatment strategies that are mutually
agreeable.
Best available
research
Patient
characteristics,
culture, and
preferences
EBP
Decisions
Clinical
expertise
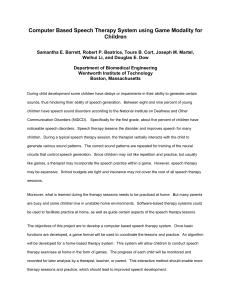
Case Study
Anna is a 14-year-old American Indian female who was
sexually abused by a 22-year-old male in her small
community. Anna disclosed the abuse to her school counselor,
who then reported the incident to tribal law enforcement.
After word of the incident spread through the community,
several individuals accused Anna of lying and then harassed her
in an attempt to recant her allegations. Anna began isolating
herself at home and stopped attending school. Anna became
increasingly depressed and demonstrated symptoms consistent
with PTSD.
How would you integrate EBP and multicultural sensitivity?
 0
0