Comparative Study BetweenNebivolol And Lisinopril In
advertisement

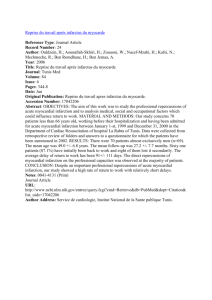
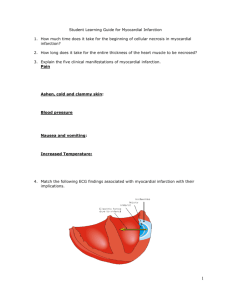
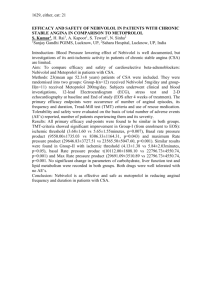
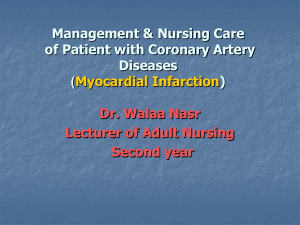
Comparative Study BetweenNebivolol And Lisinopril In Experimentally Induced Myocardial InfarctionIn Rats Mohamed El. Mansour, Mahmoud M. Elfouly, Omaima M. Abd Allah and Abeer A.Eldeeb Department of Pharmacology & Therapeutics, Benha Faculty of Medicine, Benha University. Abstract Myocardial infarction (MI) is an irreversible injury or subsequent necrosis of myocardial cells due to interruption of blood supply to a part of the heart.The present study was designed to compare the benificial therapeutic effects of nebivolol and lisinopril on the progression of myocardial infarction in a rat model of isoprenaline induced acute myocardial infarction. Animals were classified intonormal control group (received normal saline), Myocardial infarcted group (s.c injection ofisoprenaline at a dose of 150mg/kg/day diluted in 2ml of saline on two consecutive days with an interval of 24 hours between application, Nebivolol treated infarcted group(0.5mg/kg p.o.) once daily for 4 weeks after induction of MI, Lisinopril treated infarcted group (20mg/kg p.o.) once daily for 4 weeks after induction of MI. The obtained results in the current work revealed that induction of myocardial infarction by isoprenaline resulted in significant increase heart rate, decrease mean arterial blood pressure and increase T-wave voltageat the end of the study, while administration of nebivolol and lisinopril to myocardial infarcted rats for 4 weeks resulted in decrease of heart rate, decrease mean arterial blood pressure, decrease in T-wave voltageand improved histopathological changes of heart as compared to infarcted untreated rats. Conclusively:Administration of Nebivolol and lisinopril immediately afteroccurance of acute myocardial infarction prevent progression of the disease and improve pathological changes occurred in the heart. INTRODUCTION: Cardiovascular diseases cause 12 million deaths throughout the world each year, according to the third monitoring report of the World Health Organization (Gharacholou et al., 2011). Risk factors for CAD include smoking, hypertension, dyslipidemia, diabetes mellitus, obesity, mental stress and depression.The major cause of acute myocardial infarction is coronary atherosclerosis with superimposed luminal thrombus, which accounts for more than 80 percent of all infarcts. Myocardial infarctions resulting from non atherosclerotic diseases of the coronary arteries are rare (Ohtani et al., 2006). Disruption of plaques is considered to underlie most acute coronary syndrome (Boersma et al, 2003). Nebivolol has been shown to have protective effects in experimental models of experimental ischemia and reperfusion injury (Vandeplassche et al., 1991). In humans, it was shown that administration of nebivolol, as compared with atenolol, more effectively improves exercise tolerance and time to onset of angina during exercise test (Van Bortel et al., 1992). Nebivolol and carvedilol have been shown to increase coronary flow reserve in patients with ischemic heart disease and non ischemic dilated cardiomyopathy more consistently than other β-blockers,which is expected to be associated with a clinically relevant reduction in ischemic threshold (Galderisi et al., 2008).It has been suggested that early beta-blocker treatment decreases myocardial oxygen consumption, favorably influences coronary blood flow, reduces infarct size and improvements in ejection fraction (Halkin et al., 2004). Studies with nebivolol have showed that cardio-protective effects were not only mediated by their adrenergic receptor blocker activity, but also by other mechanisms such as antioxidant activity and anti-neutrophil effects (Yang et al., 2003 and Celik et al., 2006).The mechanism by which lisinopril improves the outcome following an acute MI involves reduced peripheral vascular resistance, improved perfusion and a direct action on the myocardium. Addition of an ACE inhibitor within the initial 24 hour period after an acute MI, attenuates LV dilatation, improves perfusion and inhibition of angiotensin II production reduces the workload on the heart, and inhibits collagen production (Maki Urushihara and Hiroyuki Kobori, 2011).ACE inhibitors reduce ischaemic events, mortality and hospital admissions (heart failure or further MI) in this group of patients. There is good evidence to suggest that they should be started early (Pedrazzini et al., 2008). MATERIALS AND METHODS: Myocardial infarction was induced in rats by subcutaneous injection of isoprenaline at a dose of 150mg/kg/day diluted in 2ml of saline on two consecutive days with an interval of 24 hours between application. Animal groups: each group contained 6 rats. Group (I): Normal control group (given saline only). Group (II): Myocardial infarction group. Myocardial infarction induced by subcutaneous injection of Isoprenaline at a dose of 150mg/kg/day diluted in 2ml of saline on two consecutive days with an interval of 24 hours between application (Lobo Filho et al., 2011).Group (III):Nebivolol treated infracted group: The rats of this group given nebivolol at a dose of 0.5 mg/kg p.o. once daily for 4 weeks after 2 days of administration of isoprenaline (Mercanoğlu et al., 2010).Group (IV):Lisinopril treated infracted group: The rats of this group given Lisinopril at a dose of 20 mg/kg p.o. once daily for 4 weeks after 2 days of administration of isoprenaline(Christian et al., 1996). STATISTICAL ANALYSIS All values were expressed as mean ± S.D. Data were statistically analyzed using one way ANOVA followed by Tukey's multiple comparison tests. The p value of less than 0.05 was considered to be statistically significant. RESULTS: Effect of nebivolol versus lisinopril on myocardial infarction parameters in rats after 4 weeks. Data in table (1) show that untreated infarcted group resulted in significant increase (489.3± 13.5) in HR in comparison to control group while nebivolol and lisinopril treated group show significant decrease (408.8±10.8and 424.6± 12.2) in HR in comparison to infracted untreated group. Table 1: Effects of nebivolol and lisinopril on heart ratein isoprnaline-induced myocardial infarction in rats at the end of study (after 4 weeks). group parameter Heart rate Control Untreatedinfarcted Nebivolol treatedLisinopril treated group group group a b 405.5± 15.2 489.3± 13.5 408.8±10.8 424.6± 12.2b Data represented as Mean ± SEM (n = 6). a: Significant difference from control group at p<0.05. b: Significant difference from infarcted group at p<0.05. Data in table (2) show that untreated infarcted group resulted in significant decrease in MBP (99.46± 1.6) while nebivolol and lisinopril treated group resulted in significant decrease (81.55± 0.98 and 88.6± 2.7) in MBP in comparison to untreated infracted group. Table 2: Effects of nebivolol and lisinopril on mean arterial blood pressure in isoprnalineinduced myocardial infarction in rats at the end of study (after 4 weeks). group Control parameter Mean arterial blood pressure (MBP) 109.88± 10.7 untreated Nebivolol treated Lisinopril treated Infarcted group group group 99.46± 1.6a 81.55± 0.98a,b 88.6± 2.7a,b Data represented as Mean ± SEM (n = 6). a: Significant difference from control group at p<0.05. b: Significant difference from infarcted group at p<0.05. Data in table (3) show that untreated infarcted group resulted in significant increase (1.15±0.04) in T-wave voltage while nebivolol and lisinopril treated group resulted in significant decrease (0.42 ± 0.02and 0.71± 0.04) in T-wave voltage in comparison to untreated infarcted group. Table 3: Effects of nebivolol and lisinopril on T-wave voltage in isoprnaline-induced myocardial infarction in rats at the end of study (after 4 weeks). group Control parameter T-wave voltage 0.00 UntreatedInfarctedNebivolol treatedLisinopril treated group group group 1.15±0.04a 0.42 ± 0.02a,b 0.71± 0.04a,b,c Data represented as Mean ± SEM (n = 6). a: Significant difference from control group at p<0.05. b: Significant difference from infarcted group at p<0.05. c: Significant difference from nebivolol-treated group at p<0.05 . Data in table (4) show that untreated infarcted group resulted in significant increase (41.81±2.7%) in Percent area of degenerativechanges (%) while nebivolol and lisinopril treated group resulted in significant decrease (33.16±2.02%and 34.66±2.23%) inPercent area of degenerativechanges (%) in comparison to untreated infarcted group. Table 4: Effects of nebivolol and lisinopril onpercent area of degenerativechanges (%) in isoprnaline-induced myocardial infarction in rats at the end of study (after 4 weeks). group parameter Percent area of degenerative changes (%) Control 0.00% UntreatedInfarctedNebivolol treatedLisinopril treated group group group 41.81±2.7%a 33.16±2.02%a,b 34.66±2.23%a,b Data represented as Mean ± SEM (n = 6). a: Significant difference from control group at p<0.05. b: Significant difference from infarcted group at p<0.05. Histopthological Examination: Sections were serially cut from the apex to the base at 1-mm intervals, deparaffinized and stained with hematoxylin-eosin (HE). Control group showed clear integrity of myocardial membrane, normal cardiac fibers without any infraction or infiltration of inflammatory cells (Figure 1).Myocardial infarcted group showed significant increase of area of degenerative changes in the form of cardiac muscle necrosis with congested blood vessels, interstitial edema and inflammatory cells infiltration (Figure 2). While nebivololand lisinopril treated group showed decrease of this pathological changes (figure 3 and 4). Figure (1): A photomicrograph of a cut section in the heart of a control rat (group I)Showing interlacing (a) bundles of cardiomyocytes with (b) spindle shaped nucleus with abundant eosinophilic cytoplasm (H&Ex40). Figure (2): A photomicrograph of a cut section in the heart of infarcted rat (group II)Showing (A) Cardiac muscle necrosis. (B) Congested blood vessels. (C) Interstitial edema. (D) Inflammatory cells infiltration. (H&Ex40). Figure (3): A photomicrograph of a cut section in the heart of infarcted rat (group II)Showing (A) Cardiac muscle necrosis. (D) Inflammatory cells infilteration. (H&Ex40). Figure (4): A photomicrograph of a cut section in the heart of lisinopril treated infarcted rat (group IV)Showing (A) Decrease cardiac muscle necrosis. (B) Decrease congested blood vessels (H&Ex40). DISCUSSION Myocardial infarction (MI) is defined as irreversible injury or subsequent necrosis of myocardial cells due to interruption of blood supply to a part of the heart (Patel et al., 2010 and Upaganlawar et al., 2010). Current pharmacological treatment of MI is to control the neurohormonal activation with angiotensin converting enzyme (ACE) inhibitors and beta blockers has been shown to decrease mortality and morbidity by reducing remodeling (Rahko, 2005). The present study was designed to explore the benificial therapeutic effects of nebivolol and lisinopril on the progression of experimentally induced myocardial infraction in rats model with isoprenaline regarding to their effects on heart rate, T-wave voltage changes, mean arterial blood pressure and percent area of degenerative changes of the heart (histopathological changes of the heart). The obtained results in the current work revealed that induction of myocardial infarction by isoprenaline resulted in significant increase heart rate, decrease mean arterial blood pressure, increase T-wave voltage at the end of the study (after 4 weeks) in untreated infarcted group. These results are in agreement with Thippeswamy et al., (2009); Goyal et al., (2010) and Upaganlawar et al., (2010), who observed that ISO injected rats showed MI which is evident by significant fall in systolic, diastolic and mean blood pressure and increase in heart rate. In the present study it was found that administration of nebivolol and lisinopril to myocardial infarcted rats for 4 weeks resulted in decrease of heart rate, decrease mean arterial blood pressure, decrease in T-wave voltage. These results are in agreement with Savsani et al., (2014), showed that ISO injected rats significantly decreased in DBP and MBP along with significantly increased in heart rate as compared to normal control rats. But nebivolol treatment significantly increased in MBP along with significantly decreased in heart rate as compared to ISO injected rats. Mercanoğlu et al., (2010), observed that treatment of MI in a rat with ischemia-reperfusion model with nebivolol significantly decrease heart rate and mean blood pressure. Rosei et al., (2003) showed that nebivolol was slightly more effective, in comparison with lisinopril, in terms of reduction in DBP. This greater efficacy was obtained without any increase in adverse effects, since both treatments were equally well tolerated. Wollert et al., (1994), observed that treatment of infarcted rats with lisinopril showed decrease of both heart rate and blood pressure. And these results is in line with Veeravalli et al., (2003), who observed that treatment of infarcted rat model of acute ischemia and perfusion with lisinopril alone or in combination with apstatin decreased blood pressure and heart rate. But Ahmad et al., (2008) showed that administration of lisinopril for 4 weeks after MI produced minor effect in MBP and significant decrease HR. One study in patients with heart failure and angina indicated that ACEI treatment may worsen ischemia, because of the hypotension that compromises myocardial perfusion (Cleland et al., 1991). Regarding ECG changes, the results of the present study revealed that, infarcted untreated group showed significant increase in T-wave voltage. These results are in agreement with those of Surawicz (1974) who reported that the "T" wave was elevated in rats after coronary ischemia. The ECG tracing showed sinus tachycardia in addition to the injury current in form of highly peaked T-wave. These results were in agreement with the observation of El-Hawary et al. (1988). These results are in agreement with Björck et al. (2010), who showed that use of aspirin, beta-blockers, ACE inhibitors, or statins before hospital admission in patients with a first acute MI is associated with substantially less risk of presenting with ST elevation myocardial infarction (STEMI). Savsani et al., (2014), showed that nebivolol treatment in isoproterenol treated rats prevented the altered ECG pattern towards normal suggesting the cell membrane stabilizing potential of nebivolol which might be due to its potent antioxidant property. The mechanism of benefit from beta-blocker therapy in STEMI (ST-elevation myocardial infraction) is still unclear. It has been suggested that early beta-blocker treatment decreases myocardial oxygen consumption, favorably influences coronary blood flow, reduces infarct size and improvements in ejection fraction (Halkin et al., 2004). Renin-angiotensin-aldosterone system modulation with ACEIs reduces early and late mortality in STEMI patients even in the absence of a reperfusion strategy (Marc Cohen et al., 2010). As regard to histopathological changes in the heart it was found that treatment of infarcted rats with nebivolol and lisinopril showed improvement these changes. Savsani et al., (2014), who showed that treatment of infarcted rats with nebivolol induce improvement in histopathological changes of the heart produced in infracted untreated group in the form of decrease infiltration of inflammatory cells and the morphology of cardiac muscle fibers was relatively well preserved with decrease of necrosis. Connelly et al., (2013), showed that histologic analysis demonstrated increased extracellular matrix deposition in the noninfarct, subendocardial region of all MI groups when compared with sham operated animals. ACEi significantly reduced matrix deposition. cardiomyocyte size was increased in MI animals and significantly decrease with ACEi therapy. In post-myocardial infarction and congestive heart failure studies, the benefit from beta1 blockade arises from decreased work of the heart (via reduced HR and blood pressure), reduced ventricular fibrillation risk, and a reduction in catecholamine-induced (beta-1) cardiac necrosis and apoptosis; thus, intrinsic sympathomimetic activity reduces efficacy (Podbregar and Voga, 2002). Studies with nebivolol have showed that cardio-protective effects were not only mediated by their adrenergic receptor blocker activity, but also by other mechanisms such as antioxidant activity and anti-neutrophil effects (Yang et al., 2003). Favorable effects of nebivolol on ventricular function in patients with chronic heart failure have been reported (Edes et al., 2005 and Kurlianskaya et al., 2005). The mechanism by which lisinopril improves the outcome following an acute MI involves reduced peripheral vascular resistance, improved perfusion and a direct action on the myocardium. Addition of an ACE inhibitor within the initial 24 hour period after an acute MI, attenuates LV dilatation, improves perfusion and inhibition of angiotensin II production reduces the workload on the heart, and inhibits collagen production (Maki Urushihara and Hiroyuki Kobori, 2011). REFERENCES: Ahmad, M.; White, R.; Tan, J.; Huang, B.S. andLeenen, F.H. (2008): Angiotensin-converting enzyme inhibitors, inhibition of brain and peripheral angiotensin-converting enzymes, and left ventricular dysfunction in rats after myocardial infarction. J CardiovascPharmacol., 51(6):565-72. Björck L, Wallentin L, Stenestrand U, Lappas G and Rosengren A.(2010): Medication in relation to ST-segment elevation myocardial infarction in patients with a first myocardial infarction: Swedish Register of Information and Knowledge About Swedish Heart Intensive Care Admissions (RIKS-HIA): Arch Intern Med. Aug 9;170(15):1375-81. Boersma, E.; Mercado, N.; Poldermans, D. et al., (2003): Acute myocardial infarction. Lancet., 361:847-858. Celik, T.; Iyisoy, A.; Kursaklioglu, H. et al., (2006): Comparative effects of nebivolol and metoprolol on oxidative stress, insulin resistance, plasma adiponectin and soluble P-selectin levels in hypertensive patients. J Hypertens.,24:591–6. Christian, G. B.; Luiz, M. andKarl, T.W. (1996):Advanced Hypertensive Heart Disease in Spontaneously Hypertensive Rats.Lisinopril-Mediated Regression of Myocardial Fibrosis.Hypertension., 28: 269-275. Cleland, J.G.F.; Henderson, E.; McLenachen, J. et al., (1991): Effect of captopril, an angiotensin-converting enzyme inhibitor, in patients with angina pectoris and heart failure. J Am Coll Cardiol.,17:733–739. Connelly, K.A.; Advani, A.; Advani, S.; Zhang, Y.; Thai, K.; Thomas, S.; Krum, H.; Kelly, D.J. andGilbert, R.E. (2013): Combination angiotensin converting enzyme and direct renin inhibition in heart failure following experimental myocardial infarction.CardiovascTher., 31(2):84-91. Edes, I.; Gasior, Z.; Wita, K. (2005): Effects of nebivolol on left ventricular function in elderly patients with chronic heart failure: results of the ENECA study. Eur J Heart Fail., 7:631-9. El-Hawary, M.B.I.; Mareie, A.; El-Brairy, A.; Isaak, Z.; Moktar, S. andKhalil, A. (1988): Estimation of isoprenaline induced myocardial infarction area by histochemical methods and its correlation with serum CPK level. Med. J. Cairo Univ. 56 (2), 65:79 Galderisi, M. and D’Errico, A. (2008): Beta-blockers and coronary flow reserve: the importance of a vasodilatory action. Drugs68:579 –90. Gharacholou, S.M.; Lopes, R.D.; Alexander, K,P.; Mehta, R.H.; Stebbins, A.L.; Pieper, K.S. et al., (2011): Age and Outcomes in ST-Segment Elevation Myocardial Infarction Treated With Primary Percutaneous Coronary Intervention: Findings From the APEX-AMI Trial. Arch Intern Med., 171(6):559-67. Goyal, S.N.; Arora, S.; Sharma, A.K.; Joshi, S.; Ray, R. and Bhatia, J. (2010): Preventive effect of crocin of Crocus sativus on hemodynamic, biochemical, histopathological and ultrastuctural alterations in isoproterenol-induced cardiotoxicity in rats. Phytomed.,17:227–232. Halkin, A.; Grines, C.L.; Cox, D.A. et al., (2004): Impact of intravenous beta-blockade before primary angioplasty on survival in patients undergoing mechanical reperfusion therapy for acute myocardial infarction. J Am CollCardiol., 43:1780–7. Kurlianskaya, A.K.; Atroshchenko, E.S. and Pashuk, O.V. (2005): Improvement of endothelial function and intracardiachaemodynamic caused by nebivolol in patients with chronic heart failure. Eur J Heart Fail., 4:33. Lobo Filho, H.G.; Nestor Lemos Ferreira; Rafael Bezerra de Sousa; Eduardo Rebouças de Carvalho; Patrícia Leal Dantas Lobo and José Glauco Lobo Filho. (2011): Experimental model of myocardial infarction induced by isoproterenol in rats. Rev Bras Cir Cardiovasc., 26(3):469-76. Maki Urushihara and Hiroyuki Kobori (2011): Angiotensinogen Expression Is Enhanced in the Progression of Glomerular Disease. International Journal of Clinical Medicine., (2):378-387. Marc Cohen, M.D.; CatalinBoiangiu, M.D. and MateenAbidi, M.D. (2010): Therapy for STSegment Elevation Myocardial Infarction Patients Who Present Late or Are Ineligible for Reperfusion Therapy. J Am CollCardiol., 55(18):1895-1906. Mercanoğlu, GO.; Pamukçu, B.; Safran, N.; Mercanoğlu, F.; Fici, F. and Güngör, M.(2010):Nebivolol prevents remodeling in a rat myocardial infarction model: an echocardiographic study. AnadoluKardiyolDerg., 10:18-27. Ohtani, T.; Ueda, Y.; Mizote, I. et al., (2006): Number of yellow plaques detected in a coronary artery is associated with future risk of acute coronary syndrome: Detection of vulnerable patients by angioscopy. J Am CollCardiol., 47:2194-2200. Patel, V.; Upaganlawar, A.; Zalawadia, R. et al., (2010):Cardioprotective effect of melatonin against isoproterenol induced myocardial infarction in rats: a biochemical, electrocardiographic and histoarchitectural evaluation. European journal of pharmacology., 644:160-168. Pedrazzini, G.; Santoro, E.; Latini, R. et al., (2008): Causes of death in patients with acute myocardial infarction treated with angiotensin-converting enzyme inhibitors: findings from the GruppoItaliano per lo Studio dellaSopravvivenzanell'Infarto(GISSI)-3 trial. Am Heart J., 155(2):388-94. Podbregar, M. and Voga, G. (2002): Effect of selective and nonselective betablockers on resting energy production rate and total body substrate utilization in chronic heart failure. J Cardiac Fail., 8:369-78. Rahko, P.S. (2005): An echocardiographic analysis of the long-term effects of carvedilol on left ventricular remodeling, systolic performance, and ventricular filling patterns in dilated cardiomyopathy. Echocardiography., 22: 547-54. Rosei E.A.; Rizzoni, D.; Comini S. and Boari, G. (2003): Evaluation of the efficacy and tolerability of nebivolol versus lisinopril in the treatment of essential arterial hypertension: a randomized, multicentre, double blind study. Blood Press Suppl., 1:30-35. Savsani, H.; Shah, H.; Patel, K. and Gandhi, T. (2014):cardioprotective effect of flavonoids rich fraction of premnamucronata on isoproterenol-induced myocardial infarction in wistar rats. International Journal of Phytopharmacology.,5(2):95-108. Surawicz, B. (1974): Clinical significant of primary T-waveabnormalities. In Schalnt, R.C. and Hurst J.W. (eds.): Advancesin electrocardiography, New York, Grune and Stratton PP. 377-421. Thippeswamy, B.S.; Thakker, S.P.; Tubachi, S.; Kalyani, G.A.; Netra, M.K. and Patil, U. (2009): Cardioprotective effect of CucumistrigonusRoxb on isoproterenol induced myocardial infarction in rat. Am J PharmacolToxicol., 4:29–37. Upaganlawar, A.; Hardik Gandhi and Balaraman, R. (2010): Effect of vitamin E alone and in combination with lycopene on biochemical and histopathological alterations in isoproterenol-induced myocardial infarction in rats. J PharmacolPharmacother., 1(1): 24-31. Upaganlawar, A.; Patel, V. and Balaraman, R. (2012): Tomato lycopene attenuates myocardial infarction induced by isoproterenol: Electrocardiographic, biochemical and anti– apoptotic study. Asian Pacific journal of tropical biomedicine., 2:345-351. Van Bortel, L.M. and van Baak, M.A. (1992): Exercise tolerance with nebivolol and atenolol. Cardiovasc Drugs Ther., 6:239–47. Vandeplassche, G.; Lu, H.R.; Wouters, L.; Flameng, W. and Borgers, M. (1991): Normothermic ischemic cardiac arrest in the isolated working rabbit heart: effects of dl-nebivolol and atenolol. Basic Res Cardiol., 86:21–31. Veeravalli, K.K.; A. Akula, A.A.; Routhu, K.V.; Kota, M.K. et al., (2003): Infarct size limiting effect of apstatin alone and in combination with enalapril, lisinopril and ramipril in rats with experimental myocardial infarction. Pharmacological research.,48(6):557– 563. Wollert, K.C.; Studer, R.; von Bulow, B. and Drexler, H. (1994): Survival after myocardial infarction in the rat.Role of tissue angiotensin converting enzyme inhibition. Circulation.,90:2457-2467. Yang, Y.; Tang, Y.; Ruan, Y.; Zhang, P.; Zhou, Y.W.; Wang, P.H. et al., (2003): Comparative effects of carvedilol and losartan alone and incombination for preventing left ventricular remodeling after acutemyocardial infarction in rats. Circ J., 67:159-62. دراسة مقارنة بين كال من النبيفولول والليسينوبريل فى احتشاء عضلة القلب المحدث تجريبيا فى فئ ارن التجارب محمد المتولى منصور ومحمود محمد الفولى وأميمة محمد عبدهللا وعبير على الديب قسم األدوية والعالج كلية طب بنها -جامعة بنها يعتبر احتشاء عضلة القلب هو ضرر ال رجعة فيها او نخر الحق بخاليا عضلة القلب بسبب انقطاع وصول الدم الى جزء من القلب .وقد تم تصميم هذه الدراسة لمقارنة األثار العالجية لكالم من عقار النبيفلول والليسينوبريل على تطور احتشاء عضلة القلب المحدث معمليا للفئران بااليزوبرينالين .المجموعة األولى "الضابطة" تم اعطاء الفئران محلول ملح .%9المجموعة الثانية تم احداث احتشاء بعضلة القلب باستخدام االيزوبرينالين "051مجم/كجم/يوم" ويخفف فى 2سم محلول ملح %1.9على مدار يومين بفرق 22ساعة بين الجرعتين .المجموعة الثالثة اخذت النبيفلول " 1.5مجم/كجم" مرة واحدة يوميا بالفم لمدة 2اسابيع بعد احداث احتشاء بعضلة القلب .المجموعة الرابعة أخذت الليسينوبريل "21مجم/كجم" مرة واحدة بالفم يوميا لمدة 2اسابيع بعد احداث احتشاء بعضلة القلب .وكشفت النتائج التي تم الحصول عليها في الدراسة ان حقن األيزوبرينالين "051مجم/كجم/يوم" مخففة فى 2سم محلول ملح فى يومين متتاليين مع فاصل 22ساعة بين الجرعتين أدى إلى احتشاء عضلة القلب من خالل زيادة عدد ضربات القلب مع تغيرات فى شكل موجات (ت) بالزيادة وانخفاض ضغط الدم واحداث تغيرات نسيجية بالقلب بالمقارنة مع المجم وعة الضابطة .أما إعطاء النبيفلول بعد إحداث احتشاء بعضلة القلب أدى إلى إنخفاض فى معدل ضربات القلب وضغط الدم وانخفاض الزيادة فى موجات (ت) وتحسين التغيرات النسيجية بالمقارنة مع المجموعة المصابة التى اخذت األيزوبرينالين بدون عالج .أما إعطاء الليسينوبريل بعد احداث احتشاء بعضلة القلب أدى إلى انخفاض فى ضربات القلب وانخفاض ضغط الدم وانخفاض الزيادة فى موجات (ت) وتحسين التغيرات النسيجية بالمقارنة مع المجموعة التى اخذت االيزوبرينالين بدون عالج.