Chapter 8
Companion site for Basic Medical Endocrinology, 4th Edition
Author: Dr. Goodman
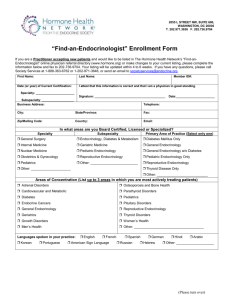
FIGURE 8.1
Storage and utilization of biological fuels.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
2
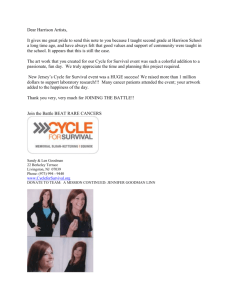
FIGURE 8.2
Intraorgan flow of substrate and the competitive regulatory effects of glucose and fatty acids that
comprise the glucose–fatty acid cycle. See text for details.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
3
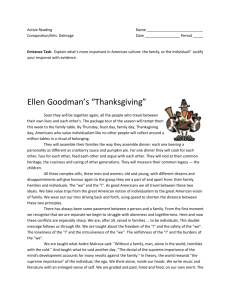
FIGURE 8.3
Actions of AMP activated protein kinase (AMPK) in muscle increase oxidation of fatty acids and
glucose. Phosphorylation inactivates acetyl CoA carboxylase (ACC) and activates malonyl CoA
decarboxylase (MCD). (See text for details.) TG = triglyceride; PL = phospholipids; DAG =
diacylglycerol; FACoA = fatty acyl coenzyme A; ACT-1 = acyl carnitine transferase-1; FA-carnitine
= fatty acyl carnitine.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
4
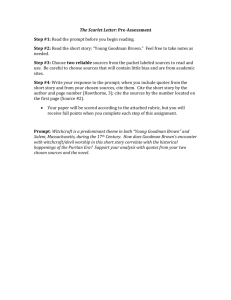
FIGURE 8.4
Multiple effects of AMP activated kinase (AMPK) that summate to increase energy producing
reactions and inhibit energy consuming reactions.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
5
FIGURE 8.5
Interaction of hormones to maintain the blood glucose concentration. Green arrows denote
increase; red arrows denote decrease.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
6
FIGURE 8.6
Counterregulatory hormonal responses to insulin-induced hypoglycemia. The infusion of insulin
reduced plasma glucose concentration to 50 to 55 mg/dL. (From Sacca, L., Sherwin R., Hendler,
R., and Felig P. (1979) Influence of continuous physiologic hyperinsulinemia on glucose kinetics
and counterregulatory hormones in normal and diabetic humans. J. Clin. Invest. 63: 849–857.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
7
FIGURE 8.7
Synergistic effects of cortisol, glucagon, and epinephrine on increasing plasma glucose
concentration. Note that the hyperglycemic response to the triple hormone infusion is far greater
than the additive response of all three hormones given singly. (Redrawn from data of Eigler, N.,
Sacca, L., and Sherwin, R.S. (1979) Synergistic interactions of physiologic increments of glucagon,
epinephrine, and cortisol in the dog. J. Clin. Invest. 63: 114–123.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
8
FIGURE 8.8
Hormonal effects on FFA production. Epinephrine and norepinephrine stimulate hormone-sensitive
lipase through a cyclic AMP mediated process. Insulin antagonizes this effect by stimulating cyclic
AMP degradation. T3, cortisol, and growth hormone increase the response of adipocytes to
epinephrine and norepinephrine. Growth hormone also directly stimulates lipolysis. Insulin indirectly
antagonizes the release of FFA by increasing reesterification. Growth hormone and cortisol
increase FFA release by inhibiting reesterification.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
9
FIGURE 8.9
Effects of metabolic hormones on adipose tissue. *Lipolytic effects of cortisol are permissive.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
10
FIGURE 8.10
Effects of metabolic hormones on skeletal muscle. *The stimulation of fatty acid oxidation by growth
hormone and cortisol are indirect and result from increased fatty acid mobilization.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
11
FIGURE 8.11
Effects of metabolic hormones on the liver.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
12
FIGURE 8.12
Quantitative turnover of substrates in a hypothetical person in the basal state after fasting for 24
hours [–1,800 calories]. (From Cahill, G.F. Jr. (1970) Starvation in man. N. Engl. J. Med. 282: 668–
675.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
13
FIGURE 8.13
Representative values for plasma glucose and metabolic hormones during fasting. Values for
growth hormone are averaged over 24 hours. The small decline in cortisol may reflect a decrease in
cortisol binding globulin.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
14
FIGURE 8.14
Effects of 1 day of fasting on GH secretion. A. Normal fed young man. B,L,D indicate meal times.
GHRH (1μg/kg) was given intravenously at the time indicated by the arrow. B. GH concentrations in
plasma in the same subject after a 24-hour fast. Blood was sampled every 20 minutes. Note that
GH secretion is pulsatile and that the amplitudes of the spontaneous secretory bursts and the
response to GHRH were increased by fasting. (From Ho, K.Y., Veldhuis, J.D., Johnson, M.L.,
Furlanetto, R., Evans, W.S., Alberti, K.G., Thorner, M.O. (1988) Fasting enhances growth hormone
secretion and amplifies the complex rhythms of growth hormone secretion in man. J. Clin. Invest.
81: 968.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
15
FIGURE 8.15
Plasma concentrations of glucose in normal subjects and patients suffering from isolated deficiency
of GH during control days of normal food intake and while fasting. Some GH-deficient patients were
untreated and others were given 5 mg of hGH per day (treated). The fast began after the collection
of blood on day 2. (From Merimee, T. J., Felig, P., Marliss, E., Fineberg, S.E., Cahill, G.F. Jr. (1971)
Glucose and lipid homeostasis in the absence of human growth hormone. J. Clin. Invest. 50: 574–
582.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
16
FIGURE 8.16
Changes in sources of fuels utilized during prolonged exercise at 30% of maximal oxygen
consumption. (Drawn from the data of Ahlborg, G., Felig, P., Hagenfeldt, L., Hendler, R., and
Wahren, J. (1974) Substrate turnover during prolonged exercise in man. Splanchnic and leg
metabolism of glucose, free fatty acids, and amino acids J. Clin Invest. 53: 1080–1090.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
17
FIGURE 8.17
Changes in concentration of insulin and counterregulatory hormones during prolonged moderate
exercise. Values shown are the means obtained for eight young men exercising on a bicycle
ergometer at ~50% of maximum oxygen consumption. (Drawn from data of Davis, S.N., Galassetti,
P., Wasserman, D.H., and Tate, D. (2000) Effects of gender on neuroendocrine and metabolic
counterregulatory responses to exercise in normal man. J. Clin. Endocrinol. Metab. 85: 224–230.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
18
FIGURE 8.18
Postulated interaction between exercising muscle and resting muscle via the Cori cycle. (Redrawn
from Ahlborg, G., Wahren, J., and Felig, P. (1986) Splanchnic and peripheral glucose and lactate
metabolism during and after prolonged arm exercise. J. Clin. Invest. 77: 690–699.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
19
FIGURE 8.19
Adipocyte differentiation. GH = growth hormone; IGF-I = insulin-like growth factor-I; TNF- = tumor
necrosis factor-; PDGF = platelet-derived growth factor; FGF = fibroblast growth factor; EGF =
epidermal growth factor; TGF-= transforming growth factor-; TGF-= transforming growth factor.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
20
FIGURE 8.20
Data showing changes in body weight and fat content with aging obtained in five independent
studies of individuals living in the early to middle decades of the twentieth century. (From Forbes,
G.B., Reina, J.C. (1970) Adult lean body mass declines with age: Some longitudinal observations.
Metabolism 19: 653–663.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
21
FIGURE 8.21
Changes in energy expenditure after increase or decrease of body weight. Thirteen normal subjects
were overfed a defined diet until their body weight increased by 10%. Eleven normal subjects were
underfed until their body weight decreased by 10%. Both groups were then fed just enough to
maintain their new weights for two weeks, at which time energy expenditure and lean body mass
were measured. (Drawn from data of Leibel, R.L., Rosenbaum, M., Hirsch. (1995) Changes in
energy expenditure resulting from altered body weight. N. Engl. J. Med. 332: 673–674.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
22
FIGURE 8.22
Hypothetical regulatory system for maintaining constancy of adipose mass by monitoring the mass
of stored fat. Adjustments in energy intake and expenditure are made to maintain constancy. Green
arrows (+) denote increase; red arrows () denote decrease.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
23
FIGURE 8.23
Schematic drawing of the relationship between the principal neurons in the arcuate nuclei that
control fuel consumption and energy utilization to each other and to their up- and downstream
effectors. NPY = neuropeptide Y; NPYR = NPY receptor; AGRP = agouti related peptide; MCR4 =
melanocortin receptor 4 (MSH receptor); MCH = melanin concentrating hormone; -MSH = melanocyte stimulating hormone; CART = cocaine and amphetamine related transcript; GABA =
gama amino butyric acid; GnRH = gonadotropin releasing hormone; CRH = corticotropin releasing
hormone; TRH = thyrotropin releasing hormone; GHRH = growth hormone releasing hormone.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
24
FIGURE 8.24
Effects of leptin in leptin-deficient mice. Body weights of female obese mice treated with saline
(Control) or 270 μg of leptin/day were compared to body weights of obese mice treated with saline,
but were fed an amount of food equal to that consumed by the leptin-treated mice (pair-fed). Note
that the loss of body weight produced by leptin was not accounted for simply by decreased food
intake. (From Levin, N., Nelson, C., Gurney, A., Vandlen, R., de Sauvage, F. (1996) Pair-feeding
studies provide compelling evidence that the ob protein exerts adipose-reducing effects in excess
of those induced by reductions in food intake. Proc. Natl. Acad. Sci. USA 93: 1726–1730.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
25
FIGURE 8.25
Leptin concentrations in blood plasma correlate with body fat content in 500 human subjects. (From
Caro, J.F., Sinha, M.K., Kolaczynski, J.W., Zhang, P.L., Considine, R.V. (1996) Leptin: The tale of
an obesity gene. Diabetes 45: 1455–1462.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
26
FIGURE 8.26
Twenty-four-hour profiles of plasma concentrations of glucose and insulin in 15 obese and 14 ageand sex-matched normal subjects. The greater excursions of insulin values in the obese despite
virtually identical levels of blood glucose are indicative of decreased sensitivity of liver, muscle, and
adipose tissue to the actions of insulin. (From Polonsky, K., Given, B.D., and Van Cauter, E. (1988)
Twenty-four-hour profiles and pulsatile patterns of insulin secretion in normal and obese subjects. J.
Clin. Invest. 81: 442–448.)
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
27
FIGURE 8.27
Overall regulation of energy balance. Ghrelin is the only known hunger signal arising from gut. All
other input from the GI tract signal satiety. Leptin and insulin are the principal adiposity signals.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
28
FIGURE 8.28
Major routes of communication in the regulation of energy balance. Cross talk between the
hypothalamus and the dorsal vagal complex integrates input from adiposity and satiety signals. The
dorsal vagal complex includes the area postrema, the nucleus of the tractus solitarius, and the
dorsal motor nucleus of the vagus. IL-6 = interleukin 6; CRH = corticotropin releasing hormone;
MCH = melanin concentrating hormone; OXM = oxyntomodulin; PYY = peptide YY; CCK =
cholecystokinin; GLP-1 = glucagon-like peptide-1; PPP = pancreatic polypeptide.
Companion site for Basic Medical Endocrinology, 4th Edition. by Dr. Goodman
Copyright © 2009 by Academic Press. All rights reserved.
29