Risk Management?
advertisement

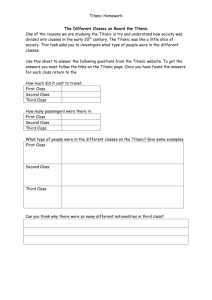
RISK MANAGEMENT? Presented By: KHURRAM ALI KHAN MarshEFU Risk Management 0 Relevance of Losses to (Engineering) Risk Management? Stages of Risk Management Risk Identification – what can go wrong Risk Quantification – probability and severity Mitigation – safeguards, “hard” and “soft” Risk Tolerance Criteria – Corporate, Legislative, Social Acceptability – ALARP “As Low as Reasonably Practical” Relevance of Losses ? MarshEFU Risk Management 1 Relevance of Losses to (Engineering) Risk Management? Tolerability criteria and Mitigation requirements, both legislative or corporate, are often based on incident investigations – ASME Boiler codes written in blood spilled in the 19th and 20th centuries. Hauge street explosion, New York 1850 , 67 dead SS Pennsylvania, Memphis 1858, 250 dead Town and son factory, Yorkshire 1869, 15 dead “Rules for construction of Boilers” issued in 1914 as an act of public service in response to numerous failures and mishaps in ships, factories, steel mills and woodworking shops” – Management of Change procedures – post Flixbrough and 28 fatalities MarshEFU Risk Management 2 Incre asing C onseq uen ce Risk Evaluation – Risk Matrices Frequency of Losses helps quantify probability 4 - Ca t a st ro ph ic C B A A 3 - C ritic a l D C B A 2 - M a rg ina l D D C B 1 - N e glig a ble D D D C 1 - U nlik e ly 2 - O c c a s ion a l 3 - P ro ba b le 4 - Fr e qu e nt I n c re a s in g F re q u e n c y CONSEQUENCE - People / Reputation / Environment / Assets MarshEFU Risk Management 3 Does Learning From Losses have a Shelf Life? To help with this question we will examine a 1912 loss, the most famous maritime disaster in history. Recognise this Ship? MarshEFU Risk Management 5 Recognise this Ship? The White Star Liner’s The Olympic MarshEFU Risk Management 6 The White Star Liner Company The Olympic: Commissioned 14th June 1911 The Titanic: Commissioned 11th April 1912 MarshEFU Risk Management 7 Sinking of Titanic, 15 April 1912 Owner: White Star Line Construction: Harland & Wolff, Belfast MarshEFU Risk Management 8 Olympic Class of White Star Steamers Developed by JP Morgan’s White StarShipping Group Constructed by Harland & Wolff in Belfast included The Olympic, The Titanic and The Britannic Designed to compete with Cunard & German Shippers on the prestigious Transatlantic English Channel in the early 1900s Built for affluent travelers offering highspeed luxury – The prized ‘Blue Riband’ was bestowed upon the ship with the fastest crossing. Held by Cunard’s Mauretania 1907-1929 Reference: ‘The Riddle of the Titanic’, Gardiner et. al. Orion, 1998 MarshEFU Risk Management 9 Sinking of Titanic, 15 April 1912 Details: – 882 ft 9 in (269.1 m) long, 92 ft 6 in (28.2 m) wide – Gross register tonnage of 46,328 tons – Steam from 29 boilers powered two reciprocating steam engines and one low-pressure Parsons turbine, which drove three propellers. – Possible top speed of 23 knots (43 km/h). MarshEFU Risk Management 10 What has changed since 1912 Information technology – Computers, phones, radar Advanced materials – metallurgy, plastics, resins Huge advances in machinery design. Mass transit systems MarshEFU Risk Management 11 Timeline 10 April 12:00 departure Titanic from Southampton on maiden voyage to New York (via Cherbourg and Queenstown) 12 April, reports of ice fields on course coming in 14 April, increasing ice field reports, course altered to south, speed maintained at 22 knots 14 April, night: moonless, clam seas, temperatures just below freezing 14 April, 23:00, Californian radioed more ice and mentioned it stopped for the night because of pack ice, answer from Marconi radio operator ”shut up, shut up, I’m busy, I’m working Cape Race” MarshEFU Risk Management 12 Timeline 14 April, 23:40 – “iceberg directly ahead” alarm from crows nest to bridge – First Officer Murdoch ordered helm hard to starboard and engines stopped – to prevent stern hitting iceberg, he then ordered helm hard to port, this manoeuvre came too early and – ship’s bow hit undersea shelf of ice, causing damage to riveted seams 14 April, 23:52 decision to restart engines by Ismay, increasing leak, with rivets popped open below water line over length of 90 m, allowing increasing amounts of water to enter damaged compartments, causing bow to sink, and water eventually to rise above watertight bulkheads terminating at E deck MarshEFU Risk Management 13 Timeline 15 April, 00:10 distress calls started (SOS) 15 April, 00:19 engines stopped for last time 15 April, 00:27 first lifeboat lowered (with capacity for 65 people, carrying 27) 15 April, 00:35 distress rockets launched 15 April, 02:20 Titanic sinks 15 April, 04:10 Carpathia arrived on scene MarshEFU Risk Management 14 What lessons can we (still) learn ?? Learning from previous Incidents Staff Selection Organizational Goals and Leadership Management of Change Material Integrity Emergency Planning MarshEFU Risk Management 15 The Olympic – Prelude to Disaster Learning from Incidents and Staff Selection 21st Jun 1911 – Upon commissioning crashed into & almost sunk O.L. Halenbeck in Manhattan 20th Sep 1911 - Crashed into the Naval Cruiser the HMS Hawke in Southampton 24th Feb 1912 - Knocked-off one of its twenty-six tone propellers on a well-known wreck in the Grand Banks Captained by Edward J. Smith. Were large displacement effects understood? How were people trained? MarshEFU Risk Management 16 Staff selection and learning from previous incidents Regarded as very experienced but….. 27th Jan 1889 - Ran The Republic aground in New York 1st Dec 1890 - Ran The Coptic aground in Rio de Janerio 4th Nov 1909 - Ran The Adriatic aground outside New York History of running ships too fast through narrow passages.. and of not adequately training his officers Captain Smith was commissioned to command the Titanic MarshEFU Risk Management 17 Setting the Right Culture Titanic was “Unsinkable” and specifically built to “Compete” for the fastest Atlantic crossing – This set the tone for poor decisions and leadership pressures Personnel competency and leadership (pressure to make fast crossing Incident investigation (no culture of near miss reporting and accident / incident investigation on previous events involving captain Smith) Decision by Ismay (White Star Managing Director) to start engines after impact and reach Halifax under own steam) Smith received at least six warnings of Ice from ships at dead stop in the area Titanic sped toward ice field at 22.5 knots vs a recommended 10 knots in such conditions No binoculars in the crows nest made early warning near impossible No need for lifeboats MarshEFU Risk Management 18 ‘Safety outweighing every other consideration’ Was the framed notice in the chart room of every White Star liner in 1912 MarshEFU Risk Management 19 Setting the right culture “… I faced a dilemma on the day, standing 20 metres from the explosion and the fire as to whether or not I should activate ESD 1, because I was for some strange reason, worried about the possible impact on production …” MarshEFU Risk Management 20 Quality Control and Material Identification Asset integrity (rivets of best rather than best-best quality with high concentration of slags) Shortage of skilled riveters Rivets popping contributed to speed of sinking Inferior quality of steel alloys is a genuine concern today Mix-up of materials is a known cause of incidents – 2nd fire at Texas City MarshEFU Risk Management 21 Quality Control and Material Identification France: 6,500 faulty Chinese valves in use N-090925-02 Sud Robinetterie (SRI). Vannes Rigau S.A.S. On September 24, the regional newspaper La Provence reported that it had exclusive information, confirmed by Direction Régionale de l’Environnement, de l’Aménagement et du Logement (DREAL – Regional Administration of Environment, Planning and Housing), that several thousand substandard Chinese-made valves were in use throughout French industry. The valves were reportedly delivered to Vannes Rigau S.A.S., in Lille, on the orders of its parent company in Marseille, Sud Robinetterie. The valves in question were described as “corner or angle valves”, “globe valves”, and “flapper valves”, in carbon steel, and certified by the German TÜV before their entry into France. According to La Provence, the valves have incorrect heat treatment, and are prone to leak at low temperatures. Expected to operate down to -10ºC, they can only be used down to +5ºC. It was alleged that one of these valves may have been involved in an un-reported incident at Total’s Gonfreville site in April, 2009 MarshEFU Risk Management 22 Management of Change Lowering watertight bulkheads to allow ease of movement of people – As the bow sank, water came above E deck, accelerating the sinking as there were no bulkheads to limit the ingress. – Hazard evaluation (requirement to be unsinkable relies on integrity of watertight compartments, see above) Was the decision to change the rivets a conscious one? Lifeboats had been reduced for 64 to 22 in favour of more expansive promenade decks cf Olympic design Insufficient to take the passengers and crew MarshEFU Risk Management 23 Management Of Modifications As important as ever Norway's PSA criticizes StatoilHydro's safety culture In May 2008, StatoilHydro’s Statfjord A platform, discharged 400 m³ of oil from one of the shafts into the Norwegian North Sea. StatoilHydro was forced to evacuate 156 persons. MarshEFU Risk Management 24 Management Of Modifications As important as ever Norway's PSA criticises StatoilHydro's safety culture LONDON, September 27 2008 – Norway’s Petroleum Safety Authority (PSA) has released a report attacking StatoilHydro's safety standards on the Norwegian continental shelf PSA indicated dissatisfaction with the quality of the risk assessment StatoilHydro and partners Industrikonsult AS (IK) and Aker Solutions AS carried out for the modification work on Statfjord A's utility shaft. It said they had failed to meet regulatory standards PSA issued an order to StatoilHydro to revamp its procedures for these types of projects by November 1. It also ordered that management of modification improvements be appreciably improved by December 1 PSA also ordered Aker "to identify and implement necessary improvements in the company's management of modification assignments, including identification of risk and use of information about risk in planning and executing hazardous work operations, including the selection of work methods and equipment, and follow-up of subcontractors" MarshEFU Risk Management 25 Emergency Planning Major accident potential (worst case scenario sinking) was discounted. Emergency response arrangements (total lifeboat capacity of 1,172 for maximum number of passengers and crew of 3,547, however complying with regulatory requirements. – Original design had just about enough lifeboats The officers on board The Titanic had not trained with the lifeboats and were unsure of their holding capacity. Smith often claimed to have never faced a “near disaster” – Reportedly his performance deteriorated in the last two hours. Many people could not read the English signs There was not a standing safety-response plan.. the ‘Women and Children first’ response was a (commendable) reaction more than a previously-agreed plan. MarshEFU Risk Management 26 Lack of Emergency Planning – the results Lives Saved: Lives Lost: Total passengers Max Lifeboat Capacity 705 1500 2,205 1,600 It wasn’t until 45 minutes after the collision that officers commence preparing the lifeboats Twenty lifeboats were launched Officers feared that the ship’s davits & winches would not hold the weight of the recommended 70 people All but the last few lifeboats floated were half-filled It is a fact that had the Officers filled the lifeboats per their specification an additional 600+ people could have been saved. MarshEFU Risk Management 27 Does learning have a shelf life? The lessons from Titanic are still relevant today There are good lessons which cross between industries “Can we learn from the past”….the Risk Engineering team would say yes! MarshEFU Risk Management 28 Learning From Losses – The Insurance Perspective Much has been written on learning from incidents – Almost all clients have incident reporting systems – Few formal systems for ‘third party’ incidents Major incidents occur relatively often somewhere – Focus has been mainly on personnel safety – Lessons do not appear to be new Major incidents continue to occur Lessons are well documented, but not always learnt by other organisations – A number of possible reasons for this exist MarshEFU Risk Management 29 Risk Management and Losses “Why is learning from losses difficult?” MarshEFU Risk Management 30 (Not) learning from positive results Learning from Transformer fires ? – See plenty of transformers with no dividing fire walls – See plenty of large transformers with no deluge systems MarshEFU Risk Management 31 “Classic” Process Industry Losses around the World MarshEFU Risk Management 32 Date Country Fatalities Injuries Marsh 2004 Algeria 27 80 33 Date Country Fatalities Injuries Financial Loss (PD) Marsh 2005 India 13 300 USD 380m 34 So why do we not learn ? Distance effects Time effects Cultural effects Tunnel vision MarshEFU Risk Management 35 Distance effects Local awareness Local media pressure Local regulatory effects Potential differences between multinationals and NOCs MarshEFU Risk Management 36 Incident Timeline 1966 France 1975 UAE 1974 UK MarshEFU 1987 UK 1984 Mexico Risk Management 1989 Indonesia 1988 Brazil 1993 Venzuela 1992 France 2000 Kuwait 1998 Australia 2005 USA 2004 Algeria 2005 UK 37 Time effects “Time is a great healer” Loss of experienced people Loss of corporate memory Young companies – Not just in the Middle East Understanding Risk can change with age of plant – “Has worked fine for 20 years” MarshEFU Risk Management 38 Loss Trends and Analysis Losses by Age of Process Unit (excluding Nat Cat.) Only includes losses where age of process plant known (sample size of 79 losses) 65% of losses involve process units >30 years old Typical design life 25-30 years Losses by Age of Process Unit 3,500 3,000 Total Loss (USD Millions) 2,500 2,000 1,500 1,000 500 0 <10yrs 10 to 20yrs 20 to 30yrs >30yrs Source: LIU Loss Database MarshEFU Risk Management 39 Cultural effects “It has not happened here” Engineers like to believe things work – not consider failure Flawed assumptions re “international standards” Personnel safety vs Process safety Fear of litigation Fear of blame Difficulty in challenging upwards in some cultures MarshEFU Risk Management 40 Tunnel vision Within a site Within a division Within a company Within the industry “Unsinkable”, “built to compete” Focus is on projects, rationalisation, expansion, staying afloat MarshEFU Risk Management 41 Feyzin, France 1966 Marsh Date 1966 Country France Fatalities 18 Injuries 18 Extensive damage to nearby village 42 FEYZIN 1966 – The Lessons Design sphere drains / sample points – with fixed valve handles – to discharge outside shadow of sphere – no catch pits under spheres Improved training about: – importance of correct valve sequence and operating procedures – BLEVE can occur with water sprays and open relief valve Improved means and training about raising the alarm Coordination of emergency plans with public authorities to stop public traffic, etc. Improve fire brigade response times MarshEFU Risk Management 43 The effect of distance, time, and language ? Feyzin – French spheres generally good – Japanese spheres poorer – Recent Japanesedesigned installations below average – Recent survey found plant with most ball-valve handles removed MarshEFU Risk Management 44 What was learnt from these 2 incidents? MarshEFU Risk Management 45 1998 – Australia MarshEFU Risk Management 2005 – USA 46 Longford vs. Texas City Longford Royal Commission Report 1998 “Those who were operating GP1 on 25 Sept 1998 did not have knowledge of the dangers associated with loss of lean oil flow and did not take steps necessary to avert those dangers. Nor did those charged with supervision of the operations have the necessary knowledge and the steps taken by them were inappropriate”. Texas City Report 2005 Raffinate Splitter Startup Procedures and Application of Skills and Knowledge: “Failure to follow the startup procedure contributed to the loss of process control. Key individuals (management and operators) displayed lack of applied skills and knowledge and there was a lack of supervisory presence and oversight during this startup.” MarshEFU Risk Management 47 Conclusions: how we can learn from mistakes Recognise barriers of time and distance – Keep the lessons alive Recognise cultural barriers Promote culture of learning – not blame Share positives and negatives Recognise limitations of national and international standards Look at other industries, Columbia 2003, Nimrod 2006 Extract value from your broker relationship .. It’s a great potential knowledge transfer opportunity MarshEFU Risk Management 48