PowerPoint Slides
advertisement

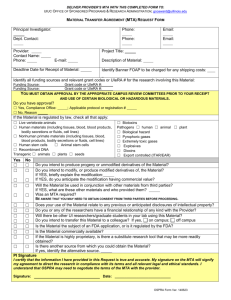
Evaluation and Management Services April 2013 INPATIENT AND OUTPATIENT SERVICES MTA, Inc What is E&M Coding? Evaluation and Management Codes (E&M) Three to 5 levels of codes for each type/location of visit Can document using: 2 Reimbursement dependent on level Documentation Guidelines Time spent in counseling and coordination of care 1997 guidelines best for psychiatry as includes a single system exam. MTA, Inc Understanding Billing Codes and Their Requirements Evaluation and Management Codes (E&M) Work Based Coding Decision based on: 3 the type and comprehensiveness of the history; extensiveness of the examination; complexity of the medical decision-making MTA, Inc Understanding Billing Codes and Their Requirements Evaluation and Management Codes (E&M) New or established client groupings 4 New: client who has not received any professional services from the physician/nonphysician practitioner or another physician of the same specialty or sub-specialty in the same group within the past 3 years. OMH consider the clinic the group. On-call: original physician’s relationship to client rules if a part of the group No distinction of new/established in an emergency room Also for payers other than Medicare, consultations may be available codes MTA, Inc Understanding Billing Codes and Their Requirements Evaluation and Management Codes (E&M) Time is defined differently depending on location: Office and OP: Face to face time Inpatient 5 Non face to face time is not included but included in work value for the service Face to face time plus work on floor or unit – reviewing charts, talking to family or other treatment staff, etc. Counseling and coordination of care MUST take place at bedside or on floor unit MTA, Inc The Three Key Components History: counting elements and components Examination: counting elements Medical Decision Making (MDM): presenting problems, additional information reviewed to determine diagnoses and management options and risk associated with management options. -6- MTA, Inc History Documentation of History will include some or all of the following elements: • Chief Complaint (CC) • History of Present Illness (HPI): must be taken by prescriber • Review of Systems (ROS): can be documented by pati • Past Medical, Family, and/or Social History (PFSH) -7- MTA, Inc Elements of HPI Timing: onset of illness; description of onset – rapid, slow, intermittent Severity: intensity; in pain management would use a 1-10 scale; Quality: how does it feel? What is the quality of the symptom Location: where is it felt? Duration: if episodic, how long last? Felt intensely for how long? Context: risk factors present or absent; when is it worse and when better – night, morning, in public, at work, etc. Modifying Factors: what makes it better – any self-help, symptoms management; what makes it worse – symptoms are relieved by or symptoms are made worse by Associated Signs and Symptoms – complains of and/or denies -8- MTA, Inc Review of Systems (ROS) A ROS is an inventory of body systems obtained through a series of questions seeking to identify signs and/or symptoms that the patient may be experiencing or has experienced. The following systems are recognized: -9- Constitutional Eyes Ears/Nose/Mouth/Throat Cardiovascular Respiratory Gastrointestinal Genitourinary Musculoskeletal Integumentary Neurological Psychiatric Endocrine Hematologic/Lymphatic Allergic/Immunologic MTA, Inc Review of Systems - ROS An earlier ROS does not need to be re-recorded. Instead, correlate to the previous ROS by noting the date and location of the earlier ROS. A review of systems may be recorded by ancillary staff or on a form completed by the patient. To document that the physician reviewed the information, there must be a notation supplementing or confirming the information recorded by others. For a Complete ROS, you may document all positive or pertinent negative responses and then state “all other systems reviewed and negative”. At least 2 positive or pertinent negative must be documented and then can do the round-up of all others. -10- MTA, Inc Past, Family, & Social History - PFSH Past Medical/Psych History Family History Social history -11- Behavioral Health Treatment, Medications Hospitalizations, Allergies Chronic Diseases General Medical Hx, developmental Hx, if appropriate Parents, Siblings, Etc. Specific Diseases Related to CC, e.g. substances, MH Hereditary/Congenital Diseases Marital Status/Family Structure Employment and Military Hx Legal Hx Sexual History Education Hobbies MTA, Inc History - Special Exception If the physician is unable to obtain a history from the patient or other source, the record should describe the patient’s condition or other circumstance that precludes obtaining a history. History will be considered comprehensive Example: “Unable to obtain history - patient unconscious” -12- MTA, Inc Documentation of History Summary: 3 of 3 required History of Present Illness (HPI) Review of Systems (ROS) Brief N/A Past, Family, and/or Social History (PFSH) N/A Brief Problem-Pertinent N/A 1-3 elements 1 system Expanded ProblemFocused Extended Extended Pertinent Detailed 4+ elements 2-9 systems 1 area Extended Complete Complete 4+ elements >9 systems 3 areas Type of History Problem-Focused 1-3 elements Comprehensive * Lowest level of the 3 components determines level of -13- history MTA, Inc 1997 Documentation of Psych Examination Problem Focused One to five elements identified by a bullet. Expanded Problem Focused At least six elements identified by a bullet. Detailed At least nine elements identified by a bullet. Comprehensive Perform all elements identified by a bullet from constitutional and psyc section and at least one element from the Muculoskeletal section. -14- MTA, Inc Medical Decision Making - MDM Number of Diagnoses or Management Options Amount and/or Risk of Complexity of Data Complications and/or to be Reviewed Morbidity or Mortality Type of Decision Making Minimal Minimal or none Minimal Straightforward Limited Limited Low Low Complexity Multiple Moderate Moderate Moderate Complexity Extensive Extensive High High Complexity Remember, two of the three elements must be met or exceeded. Medical Decision Making - MDM Number of Diagnoses or Management Options Amount and/or Risk of Complexity of Data Complications and/or to be Reviewed Morbidity or Mortality Type of Decision Making Minimal Minimal or none Minimal Straightforward Limited Limited Low Low Complexity Multiple Moderate Moderate Moderate Complexity Extensive Extensive High High Complexity Remember, two of the three elements must be met or exceeded. Coding E&M Outpatient: often the MD must code the service themselves May have nursing or other billing back-up Templates have to be helpful in assisting with the coding Inpatient: professional coders will code the service based only on your documentation 17 Templates: dictation or EMR provide guidance and reminders Paper records: take your cheat sheets with you MTA, Inc Example: Documentation Outpatient The client is a 23 year old female who needs a refill of their prescription for Lithium and Klonopin. Client moved to area 2 months ago from Florida. Diagnosed with bi-polar disorder at age of 17 years. States she is well-controlled on current medications. States she is compliant with meds and uses Klonopin only 2-3 times a week for sleep, usually after stressful work days or fights with boyfriend. 18 MTA, Inc Example: Documentation ( CC:The client is a 23 year old female who needs a refill of their prescription for Lithium and Klonopin.) (PFSH 1: Client moved to area 2 months ago from Florida.) (HPI 1: Diagnosed with bi-polar disorder at age of 17 years. HPI 2: States she is well-controlled on current medications. HPI 3: States she is compliant with meds and HPI 4: uses Klonopin only 2-3 times a week for sleep, usually after (PFSH 2: stressful work ) days or (PFSH 3: fights with boyfriend. ) CC: yes PFSH: 1 count –only social history, no past medical or family hx ROS: none HPI: Brief to extended problem pertinent Equals: Problem Focused History 19 MTA, Inc HPI Factors Timing: yes onset described Severity: yes well controlled Quality: Location: Duration: Context: yes – use of Klonopin Modifying Factors: yes - compliant with medication Associated Signs and Symptoms: 20 MTA, Inc Example: New Client PX: WDWN female in no acute distress; temp 98.6, pulse 68, BP 120/70, respirations 20. HEENT within normal limits; MSE normal, oriented x 3. Impression: Bi-polar disorder, stable on present medications. 1995 Guidelines: 3 systems = Expanded problem focused – vitals, HEENT, MSE 1 element 1997 Guidelines: one system for psych – depends on completeness of MSE – need more detail in documentation or cannot be counted – vitals and only 1 element of MSE Client stable with known illness; even though med management brings it to moderate level risk all other elements are for “straightforward”. Plan: Prescription for 60 days; Lithium level now; client to check back sooner if any problems; client referred to Health Center for annual checkup. No case management or other MH needs at this time. RTC in 60 days. 21 MTA, Inc Example: Documentation Problem-focused history Problem to Expanded problem focused exam Straightforward medical decision-making Equals: 99201 22 MTA, Inc How Codes Chosen Outpatient Services chart Inpatient Services chart 23 MTA, Inc Special Coding Considerations Time-based, Consultations, and Prolonged Services Understanding Billing Codes and Their Requirements Evaluation and Management Codes (E&M) If counseling and coordination of care are 50% or more of the time spent in the encounter: 25 E&M become time-based codes Counseling and coordination of care must be documented Time spent in C&CofC and total time must be documented MTA, Inc Level of Service Based on Time TEACHING PHYSICIANS: teaching physician may not add time spent by the resident in the absence of teaching physician to face-to-face time spent with the patient by the teaching physician with or without the resident present . Example: 26 “30 of 45 minutes on the floor concerned the coordination of ____________ care and in discussion with patient and family about treatment options. Will follow-up with them tomorrow after they have had time to discuss. “30 of 40 minutes spent at __________ bedside discussing medications and plans to ………” MTA, Inc Consultation Services Documentation required: The service is provided by a physician/NPP whose opinion/advice regarding the evaluation and management of a specific issue is being sought and has been requested by a provider. The request is recognition of the consultant’s expertise in a specific medical area beyond the requesting provider’s knowledge; The request must be documented in the medical record including why and from who the consult is being sought. A written report of the consultant’s findings, opinions, and recommendations is documented in the inpatient record. Intent is to return the patient to requesting provider for ongoing care of the problem. The consultant may: Perform or order diagnostic tests, or Initiate a treatment plan, including performing emergent procedures. 27 MTA, Inc Prolonged Services Only count the duration of direct face-to-face contact between the physician and the patient (whether the service was continuous or not) beyond the typical/average time of the E/M visit code billed for the same date of service. Must be 30 minutes or more beyond the typical time assigned to the E/M level coded Example: Average time for 99232 = 25 minutes, so a minimum of 55 minutes would be required to also bill 99356. Cannot bill prolonged services: Based on time spent reviewing charts or discussing a patient with house medical staff without direct face-to-face contact with the patient. These are add-on codes must have an underlying inpatient E/M service on the same date of service If the total duration of direct face-to-face time does not equal or exceed the threshold time for the level of E/M service the provider is billing When the E/M service is selected based on time, prolonged services may only be reported as the companion code with the highest code level in that family of codes (i.e., 99223, 99233, or 99255). 28 MTA, Inc Split Visits This is a shared visit between a physician and an NPP (within scope of practice) from the SAME practice. Can occur in hospital inpatient, outpatient (incident to) or ED Each perform a part of the E&M service Physician MUST provide a face to face portion of the E&M (clearly documented) Same patient and same DOS There is NO supervision requirement Each documents their portion Signatures and credentials of both 29 MTA, Inc Split Visits This is not simply a review of the work of the NPP – physician must clearly perform a face to face portion of the E&M NO: Seen and agree Discussed and agree Pt. seen and evaluated Code is chosen using combined work and documentation Billed at 100% of physician schedule 30 MTA, Inc Split Visits CNS makes a morning round and sees patient for subsequent hospital visit Interval history and exam Psychiatrist comes later in pm and sees patient, reviews earlier note, does brief exam and writes orders for labs, makes medication changes. 31 MTA, Inc Thank You! For additional information: Mary Thornton mthornton@marythornton.com 617-730-5800 32 MTA, Inc