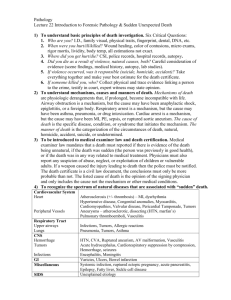
1 year 4 months old female. Vomiting and lethargy
advertisement

Pediatric Posterior Fossa Tumors: Diagnosis and follow up Esther de Luis MD. PhD. Hospital Universitario Madrid MontepríncipeSpain Clínica Universitaria de Navarra- Spain Hospital San Javier Guadalajara Mexico Pediatric Posterior Fossa Tumors • CNS tumors are the second most common pediatric tumors being exceed only by leukemya • Supratentorial and posterior fossa tumors occur in nearly equal frequency • Supratentorial tumors are more frequent in the first 2-3 years of life whereas infratentorial predominate from ages 4-10 years Objectives • Describe the intraparenchymal posterior fossa tumors in children and their imagining findings (MR and CT) and the importance of diffusion and spectroscopy in the differential diagnosis of these tumors • Review the most common complications that occur during treatment and the importance of the radiologic follow up Pediatric Posterior Fossa Tumors • The most common posterior fossa tumors in children are medulloblastoma, astrocytoma and ependymoma • The accurate diagnosis of these lesions is important to ensure that patients receive adequate therapy and prognostic information Medulloblastoma • Primitive Neuroectodermal Tumor of the posterior fossa (PNET) • Tumor with neuroblastic or glioblastic elements (embryonal tumor) • May appear intraventricular its origin is vermis cerebellar parenchyma • Children 6-11 years old • Males 2-4 times than females • The duration of symptoms is short: nausea, vomiting (area postrema), lethargy in small children and ataxia in older • Spinal metastases are present in initial diagnosis 30% cases • Extent of disease is the most important predictive prognosis • Increased frequency: Basal cell nevus syndrome Medulloblastoma 1 year 4 months old female. Vomiting and lethargy Medulloblastoma 1 year 4 months old female. Vomiting and lethargy Medulloblastoma 1 year 4 months old female. Vomiting and lethargy Medulloblastoma 1 year 4 months old female. Vomiting and lethargy Medulloblastoma 1 year 4 months old female. 2 months after surgery Medulloblastoma 5 years old female. Medulloblastoma removed 2 year before. Chemo and radiotherapy Medulloblastoma 5 years old female. Medulloblastoma removed 2 year before. Chemo and radiotherapy Medulloblastoma 16 years old male. Medulloblastoma removed 1 year before. Radiotherapy no chemotherapy Cerebellar Astrocytoma • 60% of astrocytomas in children are located in the posterior fossa: 40% cerebellum and 20% in the brainstem • Most common astrocytoma in children are of a specific type: Juvenile Pilocytic Astrocytoma (JPA): grade I WHO • JPA most benign astroglial tumor of CNS • JPA equal frequency males and females. 70% astrocytomas in children • Peak of incidence 8 years • Older children more frequent anaplastic astrocytoma • Symptoms: early morning headache and vomiting • Originate in midline, 30% extend into cerebellar hemispheres • 25% are solid • JPA excellent prognosis 90% survival rate after 25 years • Malignant transformation is exceeding rare • Gross total resection is curative • Tumors non surgically accessible: stereotactic radiosurgery Cerebellar Astrocytoma: JPA 15 years old female. Biopsy confirmed JPA Cerebellar Astrocytoma: JPA 15 years old female. Biopsy confirmed JPA Cerebellar Astrocytoma: JPA 15 years old female. Biopsy confirmed JPA Ependymoma • Constitute 8-12% primary CNS neoplasm in children and 815% posterior fossa tumors • Ependymal cell tumors: floor and roof of fourth ventricle • WHO grade II • The relative frequency diminishes as children grow up, they can appear at any age • In children are more common infratentorial (70%) • Slightly more frequent in males • Two age peaks: 1-5 years and four decade • Long clinical history • Nausea and vomiting, hydrocephalus (90%), torticollis, ataxia and lower cranial neuropathies(foramen of Luschka) Ependymoma Ependymoma Atypical rhabdoid teratoid tumor • • • • • Younger age than PNET Median age at diagnosis less than 2 years of age Lack of response to standard therapy Special microscopic techniques Rhabdoid cells: small round cells (only a minority of the tumor) • Cerebellum most common site • May spread through the subarachnoid space • Imaging similar to medulloblastoma, calcification is common, necrosis, cysts and hemorrhage Brainstem Tumors • Constitute 15% of all pediatric CNS tumors and 20-30% of infratentorial brain tumors • Peak of incidence 3-10 years of age • Different types: – Medullary tumors – Pontine tumors – Mesencephalic tumors • • • • Focal or diffuse Histology: astrocytoma, ganglioglioma, lymphoma The most frequent astrocytoma More frequent in NF 1 Brainstem Tumors: Medullary 15 years old male. JPA confirmed Brainstem Tumors: Pontine 9 years old male. Glioma grade II WHO Brainstem Tumors: Mesencephalic 19 years old female. JPA Brainstem: Quadrigeminal plate 16 years old female Brainstem Tumors: differential diagnosis Conclusions • It is important to know the best imaging technique and be familiar with the most common complications that occur during and after treatment • Radiologists play an important role not only in the diagnosis but also in the follow up of children with posterior fossa tumors References • • • • • • • • • • • • • • • • • • • Gallucci M, Catalucci A, Scheithauer BW, Forbes GS. Spontaneous involution of pilocytic astrocytoma in a patient without neurofibromatosis type 1: case report. Radiology. 2000 Jan;214(1):223-6. Hemant Parmar . Cynthia Hawkins . Eric Bouffet . James Rutka . Manohar Shroff . Imaging findings in primary intracranial atypical teratoid/rhabdoid tumors. Pediatr Radiol (2006) 36: 126–132 Severino M, Schwartz ES, Thurnher MM, Rydland J, Nikas I, Rossi A. Congenital tumors of the central nervous system. Neuroradiology. 2010 Jun;52(6):531-48 Garrè ML, Cama A, Bagnasco F, Morana G, Giangaspero F, Brisigotti M, Gambini C, Forni M, Rossi A, Haupt R, Nozza P, Barra S, Piatelli G, Viglizzo G, Capra V, Bruno W, Pastorino L, Massimino M, Tumolo M, Fidani P, Dallorso S, Schumacher RF, Milanaccio C, Pietsch T. Medulloblastoma variants: agedependent occurrence and relation to Gorlin syndrome--a new clinical perspective. Clin Cancer Res. 2009 Apr 1;15(7):2463-71. Vazquez E, Castellote A, Mayolas N, Carreras E, Peiro JL, Enríquez G. Congenital tumours involving the head, neck and central nervous system. Pediatr Radiol. 2009 Nov;39(11):1158-72. Barkovich AJ. Neuroimaging of pediatric brain tumors. Neurosurg Clin N Am. 1992 Oct;3(4):739-69. Takanashi J, Miyamoto T, Ando N, Kubota T, Oka M, Kato Z, Hamano S, Hirabayashi S, Kikuchi M, Barkovich AJ. Clinical and Radiological Features of Rotavirus Cerebellitis. AJNR Am J Neuroradiol. 2010 May 27. Yuh EL, Barkovich AJ, Gupta N. Imaging of ependymomas: MRI and CT. Childs Nerv Syst. 2009 Oct;25(10):1203-13. Gyure KA. Newly defined central nervous system neoplasms. Am J Clin Pathol. 2005 Jun;123 Suppl:S3-12. Hasselbalch B, Eriksen JG, Broholm H, Christensen IJ, Grunnet K, Horsman MR, Poulsen HS, Stockhausen MT, Lassen U. Prospective evaluation of angiogenic, hypoxic and EGFR-related biomarkers in recurrent glioblastoma multiforme treated with cetuximab, bevacizumab and irinotecan. APMIS. 2010 Aug;118(8):585-94. Pytel P, Lukas RV. Update on diagnostic practice: tumors of the nervous system. Arch Pathol Lab Med. 2009 Jul;133(7):1062-77. Rieken S, Gaiser T, Mohr A, Welzel T, Witt O, Kulozik AE, Wick W, Debus J, Combs SE. Outcome and prognostic factors of desmoplastic medulloblastoma treated within a multidisciplinary treatment concept. BMC Cancer. 2010 Aug 23;10(1):450. Muzumdar D, Ventureyra EC. Treatment of posterior fossa tumors in children. Expert Rev Neurother. 2010 Apr;10(4):525-46. Allen JC, Donahue B, DaRosso R, Nirenberg A. Hyperfractionated craniospinal radiotherapy and adjuvant chemotherapy for children with newly diagnosed medulloblastoma and other primitive neuroectodermal tumors. Int J Radiat Oncol Biol Phys. 1996 Dec 1;36(5):1155-61. Friedman HS, Prados MD, Wen PY, Mikkelsen T, Schiff D, Abrey LE, Yung WK, Paleologos N, Nicholas MK, Jensen R, Vredenburgh J, Huang J, Zheng M, Cloughesy T. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol. 2009 Oct 1;27(28):4733-40. Kalifa C, Grill J. The therapy of infantile malignant brain tumors: current status? J Neurooncol. 2005 Dec;75(3):279-85. Smith AB, Rushing EJ, Smirniotopoulos JG. Pigmented lesions of the central nervous system: radiologic-pathologic correlation. Radiographics. 2009 Sep-Oct;29(5):1503-24. Pediatric Neuroimaging. A.J.Barkovich. Lippincott forth edition Diagnostic Imaging. Brain. Osborn A. AMYRSIS