Simple - Vietsciences
advertisement

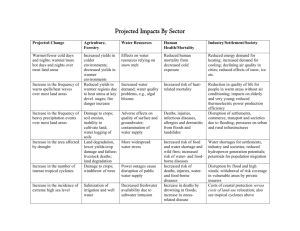
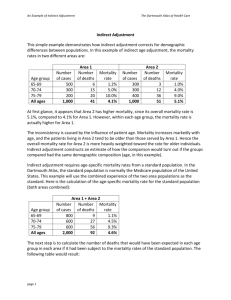
M2 Medical Epidemiology How to Fairly Compare Disease Frequencies Between Groups How to Fairly Compare Disease Frequencies Between Groups Simple epidemiologic indices: review/summary Interpreting epidemiologic comparisons: overview – chance – bias – confounding Adjustment of epidemiologic indices for confounding – direct – indirect Simple epidemiologic indices: review/summary Questions: What fraction of a group has the condition now? What fraction of the community carries the condition at any one time? What is the endemic level of the condition, relative to the size of a community? What fraction of UI students has hay fever now? Simple epidemiologic indices: review/summary Answer: Point prevalence, or prevalence for short. A dimensionless proportion. Sometimes erroneously called “prevalence rate” Simple epidemiologic indices: review/summary Questions: What is the cumulative risk (probability) of developing a condition at least once during a fixed time period? What fraction of a group can we predict will have developed a condition over a given time period, or during an epidemic? Why must I take this medicine, doctor? What are my chances of a heart attack in the next ten years, if I don't? Simple epidemiologic indices: review/summary Answers: Cumulative incidence A dimensionless proportion Called the attack rate when describing infectious disease outbreaks, – e.g., The attack rate in the county during the West Branch hepatitis outbreak was estimated as 6.5%=65 cases/1000 population. One women in 11 (9%) is expected to develop breast cancer during her lifetime. Simple epidemiologic indices: review/summary Questions: How strong is the process causing new cases? How many new cases occur per person per unit time, or other unit of experience (e.g., per passenger-trip, per passenger-mile traveled)? How many new cases of esophageal cancer occur in Illinois/1000 population per year? How many ruptured spleens occur from automotive accidents in Illinois, per million person-miles traveled? How many new HIV infections occur per 1000 acts of vaginal intercourse? Of anal intercourse? Simple epidemiologic indices: review/summary Answer: Incidence density (rate, dimension = new cases per unit of experience, such as personyear, passenger-mile, sexual acts) – e.g. 5 new cases per 1000 persons per year = – 5 new cases per 1000 person-years = – .005 new cases per person per year Units = e.g. – New cases / [persons x years] – New cases / million passenger-miles – New cases / 100 sexual acts Simple epidemiologic indices: review/summary Examples: Mortality rate: The death density, i.e. the incidence density of death. For political units in which records are kept routinely and where the population size may be constantly changing, often calculated using the mid-year population as denominator. The mid-year population approximates the total person-years exposure in the population for the full year. 10 Simple epidemiologic indices: review/summary Examples: Case-Fatality rate: The cumulative incidence of death due to a disease, during the course of the disease. i.e. the fraction of cases which result in death from the illness. Equivalently, the chance of dying from a case of the disease. Case Fatality Rate The cumulative incidence of death due to a disease, during the course of the disease. i.e. the fraction of cases which result in death from the illness. Equivalently, the chance of dying from a case of the disease. Number of deaths from a specific disease/number of cases of the disease. Usually overestimates. Why? Simple epidemiologic indices: review/summary Type of incidence Numerator Cumulative Density Number of new cases Denominator Population at risk at Person-years at risk, sometimes beginning of interval approximated by population at risk at midperiod Assumptions Constant population Constant risk over observation observed over entire span, so that 1 person observed period for two years gives same information as 2 persons observed for 1 year Uses To estimate risk for specified period and prognosis after disease event For inference about causal processes; to adjust for different lengths of observation for each individual, loss to follow-up, Simple epidemiologic indices: review/summary Incidence density (ID) vs. Cumulative incidence (CI) Question: In a population of 100 persons, deaths occur at the rate (incidence density) of 52 per 100 person-years or, equivalently, 1 per 100 person-weeks. After one year of this, what proportion of the 100 people will have died? Simple epidemiologic indices: review/summary Answer: 41%, not 52% Simple epidemiologic indices: review/summary For all factors stable, P = ID x MD where P = Prevalence MD = Mean Duration Example If incidence is 12 new cases per 1000 person-years. And duration of illness is 6 months. What is the average prevalence? 6 per thousand Simple epidemiologic indices: review/summary Relative Risk = RR either CUMULATIVE INCIDENCE RATIO CIR = CI1/CI0 or INCIDENCE DENSITY RATIO IDR = ID1/ID0 Association: a statistical feature of comparisons(s), with six possible explanations: Causation, with exposure promoting disease Chance Bias : 2 categories Selection Bias Measurement bias Confounding variable(s) Causation, with disease promoting appearance of the exposure Always ask: are there plausible alternative explanations for the data? Chance due to random variation from sampling or measurement addressed using – statistical tests of hypotheses (p-values) – confidence intervals – power analyses Bias. 2 types Selection, the way you selected subjects for the study biased your results. Measurement, the way you measured variables in your subjects biased the results. Selection bias Bias from the use of a non-representative group as the basis of generalization to a broader population of subjects or patients. For instance, a common bias of this type appears when – the prognosis of patients newly diagnosed with a given disease is inferred from the study of hospitalized patients with this disease at a major referral center, and – the disease in question has a broad spectrum behavior. Selection bias More commonly We have 2 groups Exposed and unexposed We compare them with regards to an outcome. But the way we selected the 2 groups causes differences in the outcome that have nothing to do with the exposure. Example if we used hospitalized smokers as the exposed and healthy volunteer nonsmokers as the unexposed. Selection Bias (Admission Rate -- Berkson) DISEASES OF BONES AND ORGANS OF MOVEMENT VS. RESPIRATORY DISEASE: TWO CROSS-SECTIONAL COMPARISONS DISEASES OF BONES AND ORGANS OF MOVEMENT GENERAL POPULATION RESPIRATORY DISEASE THOSE HOSPITALIZED IN PRIOR 6 MONTHS YES NO TOT. YES NO TOT. YES 17 207 234 5 15 20 NO 184 2376 2560 18 219 237 TOTAL 201 2583 2784 23 234 257 ODDS-RATIO = 1.06 ODDS-RATIO = 4.06 1 ADAPTED FROM ROBERTS RS, SPITZER WO, DELMORE T, AND SACKETT DL. J CHRON DIS 31:119-28. Selection Bias (Berkson) Necropsies TB CANCER CASES CONTROLS PRESENT 54 133 ABSENT 762 683 TOTAL 816 816 6.6 16.3 % WITH TB EOR = 0.36, P<.001 (CHI-SQUARE) More Selection Biases Whenever we compare a group of patients who use a drug to those who don’t in a non experimental observational study (cohort, not randomized). The 2 groups differ in many respects. One of the most important respects is that the patients on the drug have a reason to be on it (indication). The others don’t. Called “Bias by indication”. Bias by indication For example calcium channel blockers have 2 indications hypertension and coronary disease. If you compare hypertensive patients who are on Ca blockers to those who are on other agents (not randomized, totally at the discretion of their doctors), we would find: Bias by indication Patient on Ca blockers have higher prevalence of CAD Also higher prevalence of risk factors for CAD So if you do an observational study of hypertensive patients, comparing the outcome in those on Ca blockers to those on other agents, you may find Bias by indication That patients on Ca blockers have much worse outcomes. This is bias by indication. You can adjust and correct for preexisting heart disease and for risk factors, but may not be enough. Bias by indication If you compare hypertensive patients who are on minoxidil or hydralazine to those on other agents you find That patients on those agents have higher BP Is it because they don’t work as well ? No, the opposite. They are reserved for those with severe resistant hypertension. That is the indication for those agents. Survivor Treatment Bias Patients who received statin during admission for MI had much lower inhospital mortality. Statin? The ones who died are different. Some died very soon after admission (no statin). Competing Medical Issues Bias Some were so sick that they were treated with multiple drugs, modalities, ICU etc. No statin Bias by contraindication If you compare hypertensive patients who are on beta blockers to those on other agents you find that they have better outcomes. That does not mean they are better for you. No, this comparison is biased by contraindication. Beta blockers are contraindicated in severe COPD, CHF, PVD etc. Measurement bias Systematic or non-uniform failure of a measurement process to accurately represent the measurement target, e.g. – different approaches to questioning, when determining past exposures in a casecontrol study. – more complete medical history and physical examination of subjects who have been exposed to an agent suspected of causing a disease than of those who haven't been exposed to the agent. Measurement Bias -- Recall Bias INFLUENCE OF INTENSITY OF SEARCHING FOR EXPOSURE UPON REPORTED PROPORTIONS EXPOSED PRIOR EXPOSURE TO IRRADIATION ROUTINE QUESTIONING & RECORD SEARCH INTENSIVE QUESTIONING AND RECORD SEARCH 36 CASES OF NISHIYAMA ET AL.1 28 47 22 CASES OF RAVENTOS ET AL.2 0 50 STUDY 1 Nishayama, Schmidt, And Batsakis, J Amer Med Assoc 181:1034-38. 1 Raventos, Horn, And Ravdin, J Clin Endocr Metab 22:886-91. Measurement Bias Family information bias The flow of family information about exposures and illnesses is stimulated by and directed to a new case in its midst. Measurement Bias REPORTED PARENTAL HISTORY 1 WITH RHEUMATOID ARTHRITIS (%) WITHOUT RHEUMATOID ARTHRITIS (%) NEITHER PARENT 27 50 ONE PARENT 58 42 BOTH PARENTS 15 8 TOTAL 100 100 ADOPTED FROM SCHULL AND COBB, J CHRON DIS 22:217-22. Measurement Bias -- Family Information EFFECT OF THE SOURCE OF FAMILY INFORMATION UPON THE RESULTS OF THE FAMILY HISTORY REPORTED PARENTAL HISTORY 1 SIBLING PROVIDING FAMILY HISTORY WITH WITHOUT RHEUMATOID RHEUMATOID ARTHRITIS (%) ARTHRITIS (%) NEITHER PARENT 27 50 ONE PARENT 58 42 BOTH PARENTS 15 8 TOTAL 100 100 ADOPTED FROM SCHULL AND COBB, J CHRON DIS 22:217-22. Avoid confounding Confounding refers to distortion of the true biologic relation between an exposure and a disease outcome of interest, due to a research design and analysis that fail to properly account for additional variables associated with both. Such variables are referred to as confounders or, less formally, as lurking variables. Confounding ONE-MONTH INFANT SURVIVAL STATUS SURVIVAL AMOUNT OF CARE DEAD ALIVE TOTAL MORTALITY (%) LESS 20 373 393 5.1 MORE 6 316 322 1.9 TOTAL 26 689 715 3.6 Confounding ON ONE-MONTH INFANT SURVIVAL STATUS: CLINIC A SURVIVAL AMOUNT OF CARE DEAD ALIVE TOTAL MORTALITY (%) LESS 3 176 179 1.7 MORE 4 293 297 1.4 TOTAL 7 469 476 1.5 ONE-MONTH INFANT SURVIVAL STATUS: CLINIC B SURVIVAL AMOUNT OF CARE DEAD ALIVE TOTAL MORTALITY (%) LESS 17 197 214 7.9 MORE 2 23 25 8.0 TOTAL 19 220 239 8.0 Confounding COMMUNITY A (E.G. STATE OF ILLINOIS) AGE GROUP NUMBER IN DEATHS MORTALITY COMMUNITY IN YEAR (% PER YEAR) YOUNGER 70,000 700 1% OLDER 30,000 3000 10% TOTAL 100,000 3700 3.7% COMMUNITY B (E.G. DANVILLE) AGE GROUP NUMBER IN DEATHS MORTALITY COMMUNITY IN YEAR (% PER YEAR) YOUNGER 30,000 300 1% OLDER 70,000 7000 10% TOTAL 100,000 7300 7.3% Direct Rate Adjustment CITY A TOTAL CITY A POPULATION OBSERVED DEATHS CITY A MORTALITY RATE (PER 100,000 P-Y) 300,000 54 54/3 =18 CITY B TOTAL CITY B POPULATION OBSERVED DEATHS CITY B MORTALITY RATE (PER 100,000 P-Y) 100,000 22 22 Age specific mortality rate CITY A AGE GROUP CITY B Number Number Mortality Number of Deaths in Rate in POPULA (PER POPULA TION 100,000 TION P-Y) Number Mortality of Deaths Rate (PER 100,000 P-Y) 0-19 60,000 12 20 20,000 3 15 20-50 180,000 18 10 20,000 1 5 >50 60,000 24 40 60,000 18 30 TOTAL 300,000 54 18 100,000 22 22 Direct Rate Adjustment CITY A AGE GROUP Standard Population Agespecific CITY B Expected Deaths Mortality Rate (/100K) Agespecific Expected Deaths Mortality Rate (/100K) 0-19 20,000 20 4 15 3 20-50 40,000 10 4 5 2 >50 40,000 40 16 30 12 TOTAL 100% 24 17 Direct Rate Adjustment ANY CITY AGE GROUP Standard Population Agespecific Mortality Rate Expected Deaths (PER 100,000 P-Y) 0-19 20% … …X0.2 =… 20-50 40% … …X0.4 =… >50 40% … …X0.4 =… TOTAL 100% Age adjusted mortality rate Direct Rate Adjustment CITY A STANDARD POPULATION CITY A AGE-SPECIFIC MORTALITY RATE OBSERVED DEATHS (PER 100,000 P-Y) 0-19 50% 20/100,000 P-Y 10 20-50 30% 10/ " 3 >50 20% 40/ " 8 TOTAL 100% AGE GROUP Direct Rate Adjustment CITY A STANDARD POPULATION CITY A AGE-SPECIFIC MORTALITY RATE OBSERVED DEATHS (PER 100,000 P-Y) 0-19 50% 20/100,000 P-Y 10 20-50 30% 10/ " 3 >50 20% 40/ " 8 AGE GROUP TOTAL 100% DIRECTLY ADJUSTED RATE=DAR=21/100,000 P-Y 21 Direct Rate Adjustment CITY B STANDARD POPULATION CITY B AGE-SPECIFIC MORTALITY RATE OBSERVED DEATHS (PER 100,000 P-Y) 0-19 50% 15/100,000 P-Y 7.5 20-50 30% 5/ " 1.5 >50 20% 30/ " 6 AGE GROUP TOTAL 100% DIRECTLY ADJUSTED RATE=DAR=15/100,000 P-Y 15 Direct Rate Adjustment CITY A STANDARD POPULATION CITY A AGE-SPECIFIC MORTALITY RATE OBSERVED DEATHS (PER 100,000 P-Y) 0-19 33.3% 20/100,000 P-Y 6.67 20-50 33.3% 10/ " 3.33 >50 33.3% 40/ " 13.33 AGE GROUP TOTAL 100% OR, DAR=(1/3)(20+10+40)PER 100,000P-Y=23.3/100,000 PY 23.33 Direct Rate Adjustment CITY B AGE GROUP 0-19 20-50 >50 TOTAL STANDARD POPULATION CITY B AGE-SPECIFIC MORTALITY RATE OBSERVED DEATHS (PER 100,000 P-Y) 33.3% 15/100,000 P-Y 5 33.3% 5/ " 1.66 33.3% 30/ " 10 100% OR, DAR=(1/3)(15+5+30) PER 100,000 P-Y=16.7/100,000 P-Y 16.67 Indirect Rate Adjustment Calculate “Expected Deaths” Divide Observed Deaths by Expected Deaths (O/E) SMR (Standardized Mortality Ratio) Indirect Rate Adjustment Calculate SMR standardized mortality ratio. SMR = Observed mortality / Expected mortality To Calculate that you need to calculate expected mortality. Indirect Rate Adjustment STANDARD POPULATION MORTALITY = 28/100,000 P-Y 0-19 year old: 24/100k ; 20-50: 16/100k; >50: 50/100k CITY A AGE GROUP STANDARD CITY A POPULATION POPULATI AGE-SPECIFIC ON MORTALITY RATE 0-19 60K 20-50 180K >50 60K TOTAL 300K EXPECTED DEATHS (PER 100,000 P-Y) Indirect Rate Adjustment STANDARD POPULATION MORTALITY = 28/100,000 P-Y 0-19: 24; 20-50: 16; >50: 50 CITY A AGE GROUP STANDARD CITY A POPULATION POPULATI AGE-SPECIFIC ON MORTALITY RATE EXPECTED DEATHS (PER 100,000 P-Y) 0-19 60K 24/100,000 P-Y 14.4 20-50 180K 16/ " 28.8 >50 60K 50/ " 30.0 TOTAL 100% 73.2 Indirect Rate Adjustment Calculate “Expected Deaths” Divide Observed Deaths by Expected Deaths (O/E) SMR (Standardized Mortality Ratio) Indirect Rate Adjustment STANDARDIZED MORTALITY RATIO (SMR) = OBSERVED DEATHS/EXPECTED DEATH 54/73.2 = 74% Indirect Rate Adjustment STANDARD POPULATION 28/100,000 P-Y MORTALITY 0-19: 24; 20-50: 16; = >50: 50 CITY B AGE GROUP STANDARD CITY B POPULATION POPULATI AGE-SPECIFIC ON MORTALITY RATE EXPECTED DEATHS (PER 100,000 P-Y) 0-19 20K 24/100,000 P-Y 4.8 20-50 20K 16/ " 3.2 >50 60K 50/ " 30 TOTAL 100% 38.0 Indirect Rate Adjustment STANDARDIZED MORTALITY RATIO (SMR) = OBSERVED DEATHS/EXPECTED DEATHS 22/38 = 58% Proportional Mortality The 4 leading causes of death in Chamapign County are…. CAD is the leading cause being responsible for 32% of all deaths in the County in 2002. Proportional Mortality Number of deaths from a specific cause/ Total number of deaths in same time Proportional Mortality Ratio PMR Proportional Mortality Ratio Proportion of deaths from specified cause /Proportion of deaths from specified cause in comparison population Proportional Mortality Ratio PMR CAD is responsible for 32% of all deaths in the County in 2002. (Compared to 40% in the State of Illinois) PMR = 32%/40% = 32/40 = 0.8 Is that good or bad ? PMR Relative frequency of other causes of death can affect the PMR for the cause of interest An epidemic of a fatal disease in your population will decrease PMR for all other causes Low mortality from a very common cause (CAD for example) in your population will increase PMR for all other causes PMR Fast, easy, cheap Can be calculated when all you have is death certificates Don’t need information on demography of population. “Leading Causes of Death” How does one decide whether to present a set of data using crude, adjusted, or category-specific indices? If possible, use crude indices only to produce a quick picture of the magnitude of a problem in a population, for the purpose of establishing a prima facie need for public health and/or medical services, and as a first-cut at estimating the resources needed. How does one decide whether to present a set of data using crude, adjusted, or category-specific indices? Use category-specific indices when you wish to focus attention on the problem in one or a few population subgroups, when space is available to give a detailed presentation in order to communicate the fullest understanding of the data, and especially if specific indices vary between two populations being compared in a different manner in different population subgroups (e.g. effects are modified by age, sex or race). How does one decide whether to present a set of data using crude, adjusted, or category-specific indices? Use adjusted rates when – you wish to avoid possible confounding, – but do not have the space to present the full schedules of specific indices, or your audience does not have the patience for that, Avoid adjusted rates when – there variable being adjusted out is an “effect modifier,” that is, the relationship between groups being compared changes from stratum to stratum -- more later on this. How does one decide whether to present a set of data using crude, adjusted, or category-specific indices? Note that crude indices require one only to know the numerator cases and the denominator (population size or exposure-time) of each total population to be compared; indirect adjustment requires knowledge of only the numerator cases from the total populations and the (joint) distributions of confounder(s) in the populations to be compared; direct adjustment and specific rates require knowledge of both the numerator cases and the corresponding denominators within levels of the confounding variable(s), for all populations under comparison. Note that A directly adjusted rate of a single community means nothing by itself. It is only used to compare different communities and only if all of them are adjusted to the same standard population. SMR of a single community IS useful. It does by itself compare 2 populations.