Changes You May Wish to Make in Practice
advertisement

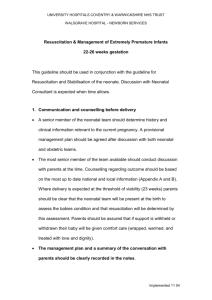
Influential Articles in Neonatal Resuscitation Henry C. Lee, MD, FAAP Lucile Packard Children’s Hospital Stanford, CA Steven Ringer, MD, PhD, FAAP Brigham and Women’s Hospital Boston, MA Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in this CME activity. I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation. • Session objectives – Discuss recent articles on evolving topics surrounding neonatal resuscitation – Discuss recent articles that may impact future neonatal resuscitation guidelines and practice • Topics to be discussed: – Encephalopathy / hypothermia – Periviable birth – Oxygen concentration for resuscitation – Cord clamping timing • Term • Preterm • Encephalopathy / Hypothermia – Hypothermia increases chance of better outcomes • Need for awareness of identification, appropriate diagnosis, and prompt therapy – Neurologic care may be next frontier for neonatology • Executive summary: Neonatal Encephalopathy and Neurologic Outcome, Second Edition, Report of the American College of Obstetricians and Gynecologists’ Task Force on Neonatal Encephalopathy. OB&GYN, April 2014; 123(4):896-901. PMID: 24785633 • Definition of neonatal encephalopathy – clinical syndrome of disturbed neurologic function in the earliest days of life in an infant born at or beyond 35 weeks gestation – Subnormal level of consciousness or seizures – Often accompanied by difficulty with initiating and maintaining respirations and depression of tone and reflexes • Signs consistent with acute peripartum or intrapartum event – Apgar score ≤ 5 at 5 and 10 minutes • (≥ 7 – unlikely to be hypoxia-ischemia) – Umbilical artery blood gas pH < 7.0 or base deficit ≥12 mmol/L • (> 7.20 – unlikely that intrapartum hypoxia played role) – Multisystem organ failure consistent with hypoxicischemic encephalopathy • Contributing factors consistent with acute peripartum or intraparum event – Sentinel hypoxic or ischemic event immediately before or during labor and delivery (such as ruptured uterus, abruption…) – Fetal heart rate monitor patterns (such as patient presenting with Category I pattern converting to Category III) • Magnetic resonance imaging / spectroscopy preferred – Ideal timing is between 24 and 96 hours after delivery – (with repeat at day 10 or later) – Timing of injury still requires further research • Hypothermia and Neonatal Encephalopathy. Committee on Fetus and Newborn. Pediatrics 2014;133(6):1146-50. PMID: 24864176 – Update from 2005 workshop / COFN commentary – Summary of randomized controlled trials of hypothermia • • • • 6 trials ~1200 infants, head or whole body cooling > 35 or 36 weeks, < 6 hours of birth Target temperature 33.5 to 34.5 degrees C for 72 hours Moderate to severe encephalopathy • Summary of large trials: – Reduction in death or major neurodevelopmental disability at 18 to 24 months by 24% (RR 0.76, 95%CI 0.69-0.84) – Number needed to treat: 7 • Areas of uncertainty: – < 35 weeks – Cooling initiation prior to transfer to cooling center • “Because the majority of infants who have neonatal encephalopathy are born at community hospitals, centers that perform cooling should work with their referring hospitals to implement education programs focused on increasing the awareness and identification of infants at risk for encephalopathy, and the initial clinical management of affected infants.” • Effects of Hypothermia for Perinatal Asphyxia on Childhood Outcomes. Azzopardi et al. (TOBY Study Group). NEJM July 10, 2014; 371(2):140-9. PMID: 25006720 – United Kingdom, original enrollment 2002 to 2006 – 325 newborns > 36 weeks – Previous study showed reduced cerebral palsy at 18 months – Current study: evaluation at 6 to 7 years of age • Testing: – Wechsler Scale of Intelligence (general measure of IQ) – Other assessments of neuro / psychosocial function • 15% loss to follow-up; 30% died • Optimal therapy requires prompt identification and initiation of protocols. » Kracer JPEDS 2014; 165(2):267-273. Changes You May Wish to Make in Practice 1. Educate others about hypothermia therapy for moderate to severe neonatal encephalopathy. 2. Develop procedures for identification and early clinical care for patients eligible for hypothermia. • Periviable birth – What is the appropriate minimum gestational age for attempting resuscitation? • Does GA affect neurodevelopmental outcomes for ventilated infants who survive to discharge home? • 199 infants at one NICU between 23 to 28 weeks GA • Limited to infants who required mechanical ventilation Outcomes did not vary by GA for those who survived • “In the US… resuscitation of infants born at 24 weeks or below is considered optional. Our data suggest that these policies make sense only if “trying and failing” in the NICU is deemed to have no moral worth.” • JAMA 2011;306(21) • Previous trials on antenatal steroids have been limited in addressing the most preterm infants (22 to 25 weeks) • Should steroids be given prior to birth before 24 weeks? • NICHD Neonatal Research Network • 1993 to 2009 • Born between 22 to 25 weeks, BW 4011000 grams • 1848 total infants • At 18 to 22 month f/u – death or neurodevelopmental impairment was less frequent when exposed to antenatal steroids: – Odds ratio 0.60 (95% CI 0.53-0.69) Death or ND impairment Antenatal steroids No steroids 22 weeks 90.2% -x 93.1% 23 weeks 83.4% 90.5% 24 weeks 68.4% 80.3% 25 weeks 52.7% 67.9% ALL 64.2% 81.5% • Overall intact survival low even with steroids (35.8%) • Limitation – observational study – could be biased by intentions of parents / clinicians • Higher rate of BPD for those exposed to antenatal steroids Periviable Birth Executive Summary of a Joint Workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists – May 2014 • “periviable period” – 20 0/7 weeks – 25 6/7 weeks • Purpose: guide management and counseling issues • “When counseling parents, it is appropriate to present the data regarding the rate of survival and long-term disabilities separately, since the parents’ perspectives and the importance they give these may be different. Physicians should recognize that the parents’ views on what is “severe” disability may be different from those of the researchers or clinicians…” • “Because most newborns at 24-25 weeks of gestation will survive if resuscitated, efforts to prolong pregnancy, intrapartum interventions for fetal benefit, and neonatal resuscitation should generally be offered, if appropriate.” Letter to Editor Jeffrey Perlman, MB, ChB Obstetrics & Gynecology Sept 2014 • “… concern – Table 3 particularly troubling … omission of a parent representative group, a critical stakeholder.” • “All studies referenced raise serious concerns for risk of bias for all outcomes…” • Dr. Perlman – – “… fetal outcomes at 23 to 23 6/7 weeks are distinctly different from those of larger fetuses. – Two possible recommendations: • Recommend against routine administration of interventions for 23 – 23 6/7 weeks except under special circumstances • All interventions may be considered (low quality of evidence) in accordance with parent preferences) – Recommend GRADE (Grading of Recommendations Assessment, Development and Evaluation) process rather than expert opinion. • Dr. Keith Barrington’s Neonatal Research blog – “Executive Summary… overall a reasonable reflection of our discussions, but… some disagreement.” – Table 3 – cesarean delivery is not recommended for fetal indications up to and including 22 weeks and 6 days, but then suddenly becomes recommended at 23 weeks and 0 days. • Dr. Keith Barrington – We do not know exact GA (except in IVF) – “This recommendation must be nuanced and take into account the particular clinical circumstances of the mother, and her values and desires.” Changes You May Wish to Make in Practice 1. Discuss issues surrounding periviable birth with a multi-disciplinary team. 2. Be able to counsel parents before and after extremely preterm birth. • What is the correct oxygen concentration to initiate resuscitation for preterm infants? • • • • • 21% 30% 60% 90% 100% • NRP 5th ed. 2005/2006 – Preference of 100% O2 with vigilance and adjustment down – Allowance of less O2 ok – Recommend pulse oximetry • NRP 6th ed. 2010/2011 – Titrate O2 to achieve saturation goals similar to term infants – No specific oxygen concentration recommended (probably not 100%, probably not 21%) Targeted Pre-ductal SPO2 After Birth 1 min 60%-65% 2 min 65%-70% 3 min 70%-75% 4 min 75%-80% 5 min 80%-85% 10 min 85%-95% • Kapadia VS, Chalak LF, Sparks JE, Allen JR, Savani RC, Wyckoff MH. Resuscitation of preterm neonates with limited versus high oxygen strategy. Pediatrics 2013;132(6):e148896. PMID: 24218465 • Testing initial FiO2 of 21% vs 100% and titrating by 10% every 30 seconds to meet NRP goals • Primary outcome: total hydroperoxide (TH), biological antioxidant potential (BAP), BAP/TH Protection Against Oxidative Stress and “IGF-I Deficiency Conditions” Munoz Biochemistry, Genetics and Molecular Biology 2012 • Eligible infants 24 to 34 weeks GA • Due to equipoise, antenatal consent not needed as long as consent obtained subsequently • Treatment failure: HR < 60 despite 30 seconds of effective PPV 100% FiO2 • Total hydroperoxide higher in high oxygen group at first hour after birth • Conclusion – May be OK to start at 21% and if needed, gradually increase to meet goal saturations. • Rook D, Schierbeek H, Vento M, Vlaardingerbroek H, van der Eijk AC, Longini M, Buonocore G, Escobar J, van Goudoever JB, Vermeulen MJ. Resuscitation of preterm infants with different inspired oxygen fractions. J Pediatr. 2014 Jun;164(6):1322-6.e3. PMID: 24655537 • Double blinded randomized trial • GA < 32 weeks • 30% vs 65% • Written informed consent prior to delivery – Led to some difficulty / selection bias • Goal saturation 88%-94% at 10 minutes – Study concentration abandoned when: • HR < 100, SpO2 / HR drop, – Start at 21% and manually adjusted per clinician • Results – Of 781 eligible infants, 193 were analyzed • Main reason for exclusion was imminent delivery • No difference in glutathione concentration or other markers of oxidative stress. • Recommendation: starting with initial concentration of 30% and subsequent adjustment Kapadia Rook Starting oxygen concentrations 21% vs 100% 30% vs 65% Enrollment All eligible Consent prior to delivery 193/781 Randomization Yes Yes Blinding No Double-blind • Rich Pediatrics 2012; 129:480 • Rich Pediatrics 2012; 129:480 Changes You May Wish to Make in Practice 1. Develop a protocol for initial oxygen concentration for resuscitation of preterm infants (?21% / 30%) 2. Develop protocols for titrating oxygen concentration based on oxygen saturation monitoring. Optimal timing of umbilical cord clamping Steven Ringer MD PhD Harvard Medical School •October 10, 2014 Not such a new concept “ Another thing very injurious to the child, is the tying and cutting of the navel string too soon; which should always be left till the child has not only repeatedly breathed but till all pulsation in the cord ceases. As otherwise the child is much weaker than it ought to be, a portion of the blood being left in the placenta, which ought to have been in the child….” Erasmus Darwin 1801 Arguments to clamp early • Potential delay in resuscitation • May interfere with cord blood banking (argued against by ACOG) • May cause polycythemia (never demonstrated) • May be more of a problem in high risk pregnancies – Maternal Diabetes – Growth Restriction On the other hand... • Abrupt interruption of umbilical cord blood flow may result in apparent need for resuscitation • Studies in fetuses demonstrated reflex bradycardia in response to umbilical cord occlusion • Dawes and co-workers, in the hallmark studies on asphyxia in Rhesus monkeys, noted that tying the cord in asphyxiated monkeys resulted in sudden bradycardia, gasps and then apnea. • If blood pressure was maintained, heart rate could be restored by positive pressure ventilation • So, does early clamping precipitate factors that then call for resuscitation, and might a delay actually avoid the need? Current recommendations • 2010 International Liaison Committee on Resuscitation (ILCOR) consensus on Science states Cord Clamping should be delayed for at least one minute in babies who do not require resuscitation….Evidence is insufficient to recommend a time for clamping in those who require resuscitation Fetal Circulation • • • • Between 30 and 50% of the combined cardiac output flows to the placenta Therefore, the same 30 to 50% of cardiac venous return comes from the placenta About 30% ( humans) of UV blood bypasses the liver through the ductus venosus. Most goes directly to left atrium The rest of venous return is to right ventricle but high PVR results in shunting to aorta Changes with cord clamping • • • • Loss of low resistance placentaSVR increases, and venous return to heart drops 30 to 50% Both effects may compromise cardiac output Left ventricular preload and output become largely dependent on pulmonary blood flow and pulmonary venous return Respirations result in decreased PVR and thereby improved LV preload and output Placental Transfusion Most of transfusion is in first 60-90 seconds, amount 25-40 ml/kg Effect on calculated blood volume in newborn and placenta Timing of umbilical cord clamping after birth for optimizing placental transfusion. Raju, Tonse Current Opinion in Pediatrics. 25(2):180-187, April 2013. DOI: 10.1097/MOP.0b013e32835d2a9e 2 Clamping and respirations • Instrumented preterm lambs, anesthetized and intubated • Randomized to Clamp 1st (filled circles): immediate cord clamping and ventilation at 2 minutes, or • Vent 1st (open circles): ventilation until pulmonary blood flow increased over 3 to 4 minutes, followed by cord clamping • Vent 1st: Immediate drop in HR, low pulmonary blood flow , spike in carotid blood pressure and flow with clamping, followed by pressure drop and flow decrease Bhatt, et al. J Physiol 2013;591:2113-2126. Changes with Ventilation Pulmonary blood flow increased, but still remained lower than Vent 1st group Carotid arterial pressure and flow rose back to high levels So, clamping before respirations resulted in decreased right ventricular output and low pulmonary blood flow, with wide fluctuations in carotid arterial pressure and flow Ventilation First, then clamp • Heart rate remained stable before and after c lamping • Pulmonary blood flow rose steadily, remained about twice as high • Carotid pressure drifted a bit lower then returned to baseline, with steady flow • Lung expansion before clamping results in stable Heart Rate, progressive rise in PBF, and stable carotid blood flow. Clinical Impact- Term Infants • • • • • • Iron deficiency in mothers and infants is a major global problem- up to 30 % of infants born to FE- deficient mothers have anemia In developed country, available supplements prevent this problem A one minute delay in cord clamping results in 80 ml transfusion in a term baby- the additional iron may prevent deficiency Numerous studies have demonstrated higher hematocrit/hemoglobin levels (2-3 gm/dL) which persist for 4-6 months No increase in polycythemia, but a potential for increased jaundice and need for phototherapy No increase in maternal hemorrhage McDonald SJ, Middleton P, Dowsweell T , Morris PS. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes Improved hemoglobin and iron status Impact in term infants and mothers • Analysis of available trials • No demonstrated maternal risk • No increase in polycythemia • Some increase in jaundice requiring phototherapy Benefits in Preterm Infants Benefits in preterm infants • Review of studies in infants 24-36 weeks gestational age. Cord clamping in the various trials delayed for 30-180 seconds. • Cochrane review found decreased incidence of any IVH in 7/10 trials ( 16.4% vs 28.7 %) (RR 1.90 for early clamping (95% CI 1.27-2.84) – Death rate similar in the two groups • No increase in need for exchange transfusion for polycythemia or hyperbilirubinemia • Recent revised Cochrane review concluded that delayed clamping results in additional benefits Intraventricular hemorrhage – all grades Severe IVH Less Necrotizing Enterocolitis No change in admission temperature Benefits in preterm infants • Systematic review of 10 trials in 454 preterm infants (<37 weeks) : • No differences in – Cord pH – Apgar scores (RR for 5 minutes score <8 was 1.17 (95% CI 0.62-2.20) – Admission temperature (mean difference 0.14 degrees(95% CI -.310.03) • Many trials document higher blood pressures and higher red cell volume • Systemic review showed reduced need for transfusions for hypotension, trend to less IVH Ghavam S, Batra D, Mercer J, Kugelman A, Hosono S, Oh W, Rabe H, Kirpalani H. Effects of placental transfusion in extremely low birthweight infants: meta-analysis of long- and short-term outcomes. Transfusion. 2014 Apr;54(4):1192-8. Caution is advised • Published randomized trials include < 200 infants < 30 weeks gestation ( the same trials cited by Ghavam) • Two RCTs followed 42 children at 18-24 months but used different developmental scales and were inconclusive • Without long term follow up and well powered studies, short term benefits may fool us into a bad practice • Unclear whether low grade IVH is a surrogate for long term outcome • These authors strongly urge caution until more data is obtained. Tarnow-Mordi WO1, Duley L2, Field D3, Marlow N4, Morris J5, Newnham J6, Paneth N7, Soll RF8, Sweet D9Timing of cord clamping in very preterm infants: more evidence is needed. Am J Obstet Gynecol. 2014 Aug;211(2):118-23. Humans likely to need resuscitation • Few trials in humans, but QI studies do add information • Infants < 35 weeks in whom cord clamping was delayed 45 seconds were compared with historical controls: – 77 VLBW and 172 LBW infants matched to controls – Vaginal births, held 10-20 cm below introitus in warm towel, gently dried. C/S births held similarly between mother’s legs – Six babies excluded based on assessment of need for resuscitation • 1 minute Apgar scores higher in delayed group • Fewer infants required resuscitation • Admission temperatures similar Is it feasible to do? • Single center study of infants less than 33 weeks gestation:Mean gestational age was less than 30 weeks and mean birth weight less than 1500 g • 480 infants, 73% (349) eligible: 236 clamped@ 45 seconds, 113 clamped early • No difference in 1 or 5 minute Apgar scores or in need for intubation • Among later clamped infants, fewer had temperatures <36.3 ⁰C • Incidence of NEC lower in late clamped group What if the infant has experienced severe acute or chronic asphyxia? • Studies on cord clamping have generally excluded those needing major resuscitation • Establishing ventilation with positive pressure ventilation does facilitate placental transfusion in experimental lambs, but it has not been studied when severe metabolic acidosis was present, as well as altered feto-placental blood flow, or compromised fetal organ function(e.g, persistent pulmonary hypertension) • The mechanics of resuscitation with the cord intact are considerable, especially during cesarean section. What if the infant has experienced severe acute or chronic asphyxia? • During fetal asphyxia, blood usually shifts from placenta to fetus- the blood volume in the delivered infant may already be as high as in infants whose cords are clamped later. • In these infants, pulmonary vascular resistance may be high, and myocardial contractility may be compromised. • One can hypothesize that a sudden increase in LV afterload and decreased preload with early cord clamping may adversely affect the infant, independent of placental transfusion • At present, these are hypothetical considerations, more studies are needed to determine whether resuscitation with the cord intact is beneficial Conclusions • • • • • In stable infants, the benefits of later cord clamping among term infants relate primarily to improved iron stores and prevention of later anemia- benefits that are primarily realized in low resource settings In stable preterm infants, numerous benefits may result from later cord clamping. Most prominent among these is a marked reduction in intraventricular hemorrhage. Caution urged before extending this practice to all low GA infants The putative benefits of later cord clamping in infants who require resuscitation are yet to be proven, although additional evidence is currently being accrued Consideration of the conduct of resuscitation when the cord is intact requires a careful evaluation of needs for team and equipment. As with all aspects of neonatal resuscitation, team training through simulation debriefing should play a major role as teams consider this change in practice! References The list of all of the articles discussed during this breakout session are available as a handout.