presentation ( format, 6MB)
advertisement
")
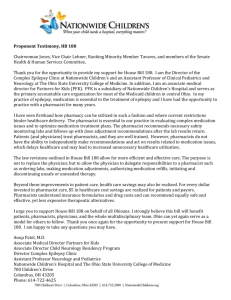
Establishing a Successful Collaborative Medication Therapy Management Service Thomas Buckley, RPh, MPH Assistant Clinical Professor University of Connecticut School of Pharmacy Faculty Disclosure Thomas Buckley has no actual or potential conflict of interest associated with this presentation. Learning Objectives 1. Describe the value of medication therapy management and collaborative drug therapy management within the patient centered medical home model 2. Illustrate the opportunities of MTM practice initiatives in Connecticut 3. Identify reimbursement options for pharmacist services Making Health Care Reform Sausage Health reform goal: Reduced cost through improved quality • Can pharmacists reduce costs through MTM services’ ability to improve outcomes? • Can pharmacists improve incentives for payfor-performance? – Shared savings? – Aligned incentives? – Integration of systems? – . . . end/reduction of fee-for-service????? “Why Pharmacists Belong In The Medical Home” • • • • Marie Smith (UConn) David Bates (Brigham&Women’s) Thomas Bodenheimer (UCSF) Paul Cleary (Yale) Health Affairs, May 2010; 29(5): 906-913 Pharmacists in Medical Home • Pharmacists “are well trained health professionals, yet they are often underused.” • “…the complementary knowledge and skills of pharmacists and prescribers can lead to improved patient care and medication use – especially for chronic conditions.” • “The medical home movement provides an opportunity to examine innovative approaches to expanding patientcentered pharmaceutical care in a collaborative, teambased practice model.” Source: Marie Smith, David W. Bates, Thomas Bodenheimer, and Paul D. Cleary. “Why Pharmacists Belong In The Medical Home. Health Affairs, May 2010; 29(5): 906-913. Patient-Centered Primary Care Collaborative “In primary care practices that offer a patientcentered medical home, comprehensive medication management by a "clinically oriented pharmacist" is needed for patients with complex regimens who are not at their therapeutic goal or are having adverse effects” Medication Facts • 75% of all healthcare costs are related to chronic disease • After lifestyle interventions, medications are the primary weapons used to prevent disease and effectively control chronic disease • Proper use of medications can lead to improved health, enhanced quality of life, and increased productivity when directly related to clinical outcome goals So why a quality gap? www.pcpcc.net Medication Facts • Four out of Five leave with at least 1 prescription¹ • One-third of all Americans take at least 5 medications • Medicare beneficiaries with multiple illnesses: – – – – – – See an average of 13 different physicians Have 50 different prescriptions filled each year Account for 76% of hospital admissions Account for 88% of all prescriptions filled each year Account for 72% of physician visits Are 100 times more likely to have a preventable hospitalization than someone without a chronic condition² Why is medication management needed in the PCMH? • Comprehensive medication management has facilitated the efficiency and effectiveness of the PCMH team in improving clinical outcomes, reducing morbidity/mortality, while lowering total healthcare costs • Medication management is even more essential when multiple providers are involved with complex patients Comprehensive medication management in the PCMH • • • • • • • Elements of comprehensive medication management: Assessment: Reveal the patient’s medication experience Identify drug-therapy problems Care Plan: Personalized goals of therapy Resolve drug problems Personalize interventions Follow-Up: Effectiveness and safety Determine patient outcomes www.pcpcc.net Core principles of PCMH In addition to cost & quality – Why is MTM needed? Adverse Drug Reactions • ADRs are the 4th leading cause of death in the US: – 106,000 deaths per year • ADR cost per year – $ 76.6 billion in US per year – The cost of drug-related morbidity and mortality exceeds the annual expenditure for drug therapy in the United States! • 28% of ADR’s are preventable Primary Care Med Use and Safety Issues 175,000 visits/yr to US emergency depts for adverse drug events (ADEs) in the elderly 32% adverse events leading to hospital admission attributed to medications 49% patients with unexplained med discrepancies between home to hospital discharge; 29% patients with unexplained med discrepancies between hospital discharge and 30-days post discharge SOURCES: National Ambulatory Medical Care Survey: 2006 Summary. Natl Health Stat Report. 2008 Aug 6;(3):1-39. Arch Intern Med. 2005;165:1842-1847; Ann Pharmacother 2008;42:1373-9.; JAMA. 2008;300(24):28672878. Ann Intern Med. 2007;147(11):755-765.; Arch Intern Med. 2006;166:565-571; Int J Med Informatics 2008:153–60; Jt Comm J Qual Patient Saf 2007 May:33(5):286-292. Primary Care Med Use and Safety Issues 71% of physician office visits involve medication therapy with 15% of visits having 4 or more prescriptions Only 47% of meds used at home were documented in EMRs; 89% of prescription medications and 76% of OTCs/herbals had discrepancies with EMR 30% patients taking prescription meds and 48% patients taking OTCs/herbals had actual meds used at home that were not recorded in EMRs Arch Intern Med. 2005;165:1842-1847; Ann Pharmacother 2008;42:1373-9.; JAMA. 2008;300(24):2867-2878. Ann Intern Med. 2007;147(11):755-765.; Arch Intern Med. 2006;166:565-571 Outcomes of MTM Studies Self-insured employer: The Diabetes 10 City Challenge • Decrease in A1C (5.2%), LDL (32%), SBP (16%), DBP (9%) • Increase in nutrition, exercise and weight loss • Employer savings of $918/employee of total health costs • ROI > 4:1 beginning in the 2nd year • 50% reduction in absenteeism and fewer worker’s compensation claims • 97.5% of patient satisfaction with diabetes care http://www.diabetestencitychallenge.com/ JAmPharmAssoc 2009; 49:383-91. MTM return on investment • Asheville Project: $1200/patient/year diabetes patients with improved outcomes • Minnesota Medicaid MTM: resolved 3.1 drug therapy problems per recipient generating average cost savings $403/patient/year – Reduction in total annual health costs exceeded cost of providing MTM by 12:1 J Am Pharm Assoc 2006; 46:133-47 J Am Pharm Assoc. 2008;48:203–11 Pharmacist Care MTM Practice Model* 1. Develop a comprehensive, active medication profile (CAMP) 2. Perform a systematic assessment of each medication for appropriateness, efficacy, safety, and adherence (in this sequence) to achieve optimal treatment goals; 3. Identify, resolve, monitor , and prevent drug therapy problems in collaboration with the PCP and other prescribers: drug therapy problems include: allergies, inappropriate medication selection, omissions, duplications, low or excessive dosages, drug interactions, adverse events, cultural competency and health literacy challenges, adherence issues, and costly regimens 4. Collaborate with the patient’s PCP, specialists, and health care professionals to optimize medication therapy and achieve treatment goals * APhA/NACDS MTM in Pharmacy Practice Core Elements 2.0 (2008) Pharmacist Care MTM Practice Model (cont’d) 5. Provide the patient with a personal medication record that can be shared with caregivers, prescribers (PCPs and specialists), and across care transitions 6. Providing the patient with a medication action plan to empower them to work on medication self-management goals and share decision-making 7. Sending the patient’s PCP (and other providers, as needed) the pharmacists’ care plan with evidence-based recommendations on identified drug therapy problems for review and action prior to inclusion in the patient’s medical record; 8. Schedule follow-up patient visits, as needed, to resolve drug therapy problems and to evaluate the patient’s progress toward achievement of medication self-management goals. Patient and PCP Reports Personal Medication Summary (Patient) • printed for patient at end of each visit • list of meds and conditions • patient medication action plan with self-management goals for continued follow-up MTM Summary Report (PCP) • med list (Rx, OTC, herbal) – directions & prescriber • drug therapy problems – linked to med & condition • comments to physician – SOAP note format Critical Perspective: CDTM vs. MTM (CDTM as a “tool” of MTM) Medication Therapy Management Service Description Collaborative Drug Therapy Management Practice Model (Provider Arrangement) Any service, regardless of intensity, Provided by a pharmacist to a patient. Practice relationship between the pharmacist, physician, and patient that provides enhanced management of care and improved health outcomes CDTM Definition (ACCP) • Collaborative practice agreement between physicians & qualified pharmacists whereby pharmacists work within the context of a defined protocol, permitting them to assume the professional responsibility for: – – – – Performing patient assessments Ordering drug therapy-related labs Administering drugs Selecting, initiating, monitoring, continuing, and adjusting drug regimens Numerous types of CDTM agreements • Smoking cessation • Emergency contraception • Immunization • HTN/hyperlipidemia • Diabetes • Pain • Depression/PTSD • • • • Refill protocol Anticoagulation Asthma/COPD UTI, pneumonia, antibiotics • STDs • Antiemetics • IV to oral therapy What is a Connecticut Model of Providing MTM? Pharmacist’s Network (Independent Practice Association) 1. CT Pharmacists Association 2. UConn School of Pharmacy faculty Contract with Health Plans/Payers, Employers, Providers, Health Systems for Pharmacist Services Recruit Qualified Pharmacists for contract services NETWORK SERVICES Negotiate Contracts • Administrative and billing service Direct payments to Pharmacists • Coordinate network of pharmacists Competency/skill-based qualifications Not dependent on pharmacists’ workplace • Validate credentials of pharmacists involved • Provide standardized pharmacist documentation tool HIPAA compliant Web-based , secure access Standardized reports • Systematic approach to all services offered Pharmacists Collaborate with Health Care Professionals & Provide PatientCentric Care Improved Patient Care and Outcomes PHARMACIST MTM: • Pharmacist at Point-of-Care (Primary Care Office/Telemedicine) • Perform Comprehensive Medication Review Develop a Personal Medication Record • Assess Medication-Related Problems (MRPs) Duplicate therapy/ Drug interactions Adverse events and side effects Adherence • Develop Patient Medication Action Plan • Document /Follow-up Plan • Communicate with Primary Care Provider CT DSS Medicaid Transformation Grant Building a Medicaid HIE and ERx Med Info Exchange UConn School of Pharmacy EHealthCT EDS Build/ Evaluate ERx Med Info Exchange Build Health Info Exchange Medicaid Data Transfer CT Pharmacist Network MEDICAID HEALTH INFO EXCHANGE Pharmacists conduct patient interviews, MTM and Adherence projects Inpatient and ED Discharge Info Hospitals Updated Med Info MTM DOCUMENTATION TOOL MTM and Adherence Reports Patient Medical Info Physician Offices Pharmacies Medicaid Ptnt Eligibility Preferred Drug List Sub-project: Medication Info Exchange Project 2008, UConn School of Pharmacy/Marie Smith, PharmD; Written permission required for any use including copying, modifying, duplication, or distribution 17 Medicaid Project - Objectives 1. Network Pharmacists build a comprehensive, active medication profile (CAMP – prescriptions, OTCs, herbal products, nutriceuticals) for Medicaid patients that can be accessed by health care providers via the Health Information Exchange. 2. Network Pharmacists assess primary care drug-therapy problems (DTPs) using the CAMP and communicate findings to primary care providers. 3. Advance the medical home concept through pharmacists’ collaboration with primary care providers 4. Improve medication adherence for Medicaid patients utilizing Rx fill data to alert prescribers on patient adherence trends. CT Medicaid MTM Results • 9 pharmacists providing MTM in PCP office; EHR access • 89 patients; 51 yo; 9.5 medical conditions; 15 meds; 4.5 visits/6 months • Medication discrepancies: >3200 between DSS claim, EHR med list, patient report • Drug Therapy Problems (DTPs): – 918 DTPs; mean 10.3 DTPs/patient – 83% resolved within 4 pharmacist/patient visits – Categories: Indication/Appropriateness(30%); Effectiveness(23%); Safety(20%); Adherence(26%) – 78% DTPs resolved through pharmacist/patient interaction (without PCP visit) • Illustrates pharmacists can improve PCP efficiency CT Medicaid MTM Results • Patient med therapy goals: 63% to 91% 1st to last visit • Cost analysis: using Medicaid drug & visit claims from previous year compared to project period – Approximate $1600/patient/year savings . . . ROI > 4:1 • Patient feedback - Overwhelmingly positive, 2 themes: • Improved patient empowerment: “answered questions not addressed in busy pharmacy”, “in control of my life”, “can now speak to my doctor” • Improved care coordination: “pharmacist communicated with my doctor and they are all on the same page” – PCP feedback • 82% PCPs made med change based on pharmacist recommendation • 90% wanted pharmacist MTM services for eligible patients Leveraging the Medicaid MTM experience Medication Optimization Grant from Center for Technology & Aging – Utilize CT Medicaid MTM model in high-risk, underserved Cambodian American communities – Pharmacist as member of Cambodian American Medical Home team – CT, MA, CA Benefits: – Patient outcomes – traditional MTM outcomes – Identification & resolution of social determinants – Cultural competency: cross-cultural teams with Community Health Workers “Delivering Culturally Appropriate Care to Optimize Medication Use in the Elderly” Use of telemedicine, videoconferencing, & spoken-format technologies Student involvement: Culturally-appropriate MTM Eliminating Barriers to Care Using Technology http://www.youtube.com/user/TechandAging?blend=7&ob=5 Project Need • Cambodian-Americans have exceptionally high prevalence of chronic mental and physical disease due to torture and trauma experienced during the Khmer Rouge regime. – escalating rates of life-threatening chronic disease • 6x rate of DM, 4x rate of stroke, 70% PTSD/depression • Lack of access to health care – – – – Language Culture Socioeconomic conditions – social isolation Lack of understanding of trauma issues • MTM research has not addressed individuals of ethnic/racial minorities – Particularly those afflicted with chronic disease from exposure to torture or trauma – Opportunity for pharmacists to impact health disparities Project Design • Goal of reaching: – 50 patients in Connecticut/Western Massachusetts (face-to-face consultation in home or clinic setting) – 50 patients in Long Beach, California (local CHW in their home or clinic and pharmacists in Connecticut via telemedicine) • Population identification – Connecticut/Western Massachusetts: case finding in the KHA provider network. – California: Mount Carmel Cambodian Project, an affiliate organization within the National Cambodian American Health Initiative – CHWs screen elderly patients to determine their use of chronic medications (risk assessment & medication history screening) – Patients matching the criteria (at least 2 chronic conditions and 3 chronic medications) will be eligible for participation in the project – Patients randomly selected and asked if they would like to participate in the project until the site number reaches 50 patients Project Design • Initial visit (pharmacist & CHW): – Developed comprehensive medication record of prescription and nonprescription therapies – Identification and potential resolution of drug-therapy problems (including medication adherence) – A medication action plan for the patient – MTM report for the patient’s provider, and f/u with provider if needed. • Follow-up visits occurred quarterly (with a goal of 4 total visits) to monitor progress with the plan • Patient received written report at each visit: – Med list (drug picture) matched to condition – List of medication-related problems (MRPs) – drug to condition – Medication action plan (what they need to do prior to next visit) • Primary care provider receives MTM report after each visit: – Med list matched to condition – MRPs match drug with condition – Pharmacist recommendations to patient and provider Results • 96 total patients (627 screened), 217 total visits (2.3/patient) over 8 months • The average patient had 6.6 medical conditions and was on 10.3 medications – 73% CVD, 72% depression/PTSD, 68% pain, 53% diabetes • 604 drug therapy problems (DTPs) were identified, or 6.3 per patient • 81% of DTPs involved medication appropriateness, effectiveness, or safety; 19% were due to nonadherence – DTPs are systems rather than patient issues Clinical Results • 93% of DTPs were resolved during the study period (with < 4 hours of MTM/patient) • Therapy outcomes goals improved 24% (69% to 93%) from initial to final MTM visit • Inappropriate medication use decreased 34.5% • Depression screen (mean Hopkins score) improved 24.5% (p=0.022) from initial to final MTM visit Clinical Results • Medication adherence behavior (Modified Morisky Survey) improved 22.5% (p=0.027) – Significantly more high adherers identified than low adherers (p=0.022) from first to final visit • Relating adherence to beliefs about medicine: – Low adherence correlated with overall negative health beliefs (p=0.015); low adherence strongly correlated with how they felt about meds in general (not their specific meds), and how prescribers use meds (p<0.001) – Reinforces importance of communication/relationship Financial Results • Cost avoidance was estimated using evidencebased analytics from Assurance© software • Calculating the costs of providing MTM: – Pharmacist & CHW costs for each patient – Compared to total of direct cost savings (drug changes or drug prevention costs) and cost avoidance (health care costs & prevention savings). – Health expenditure savings included clinic, ED, urgent care, lab, and specialty office visits avoided; work days saved, and drug therapy changes Summary of Service Savings and Costs Savings Cost Net Health Care: $329,263 $5,747 $323,516 Drugs: $13,820 $3,507 $10,313 Pharmacist & CHW $42,715 Totals: $343,083 $51,969 $291,114 (5.6 : 1) Per Encounter: $1581.03 $239.49 $1,341.54 Per Patient: $3573.78 $541.34 $3,032.44 Hospital/ER Utilization Rate Comparison 5 4.5 4.7 4 p=0.046 3.5 3 2.5 2 Non-MTM 1.75 p=0.032 1.5 p=0.032 1.5 1 0.5 0 Hospital visits Hospital LOS ER visits Survey of 140 Cambodian Americans during MTM study period Matched controls of conditions: MTM patients vs non-MTM patients MTM Culturally Appropriate MTM Conclusions • Empowered high-risk trauma patients – Realized value of health for the 1st time – Overcame mistrust of health care system – Revealed information to pharmacists never given to PCPs or family members • Reduced the burden on caregivers and the need for higher cost medical care • Identified & addressed social determinants that impact med use & overall health Culturally specific medical home Khmer Health Advocates Inc. How are MTM services recognized through payment? • Private & public sector payment approaches – State vs federal provider recognition • Consistent w/primary care payment reform • 3 approved time-based CPT codes for MTM – Document service delivery & bill any health plan (including Medicare Part D) – Federal provider recognition of pharmacists: pending legislation in Congress – would allow Part B billing • Capitation approaches for payment – PMPM; or annual capitated basis for receiving service (? model for ACO or PCMH) Credentialing Requirements of Payers • Varies widely by payer – with regard to: – Pharmacist credentials – Service delivered to patient – Recipient eligibility – Electronic documentation – Space to provide service – Billing & reimbursement Credentialing Requirements of Payers • To submit a claim, 2 things need to be in place: – Practitioner needs to be recognized as a provider by the payer • Payer specific provider ID, issued by the payer • National Provider Identification (NPI) – issued by federal gov’t http://www.cms.hhs.gov/NationalProvidentStand – Facility that submits claim must also be recognized as a facility by the payer • Licensed health care facility ID (clinic, hospital, etc) • Licensed pharmacy ID • NPI • If all payer credentials are met & when both of above are in place, you submit claim to any payer who has ability to accept claims for pharmacy services using a CMS 1500 claim form (for Medicare or Medicaid claims) Compensated Services of Current Payers • Clearly defining & understanding the service you are being asked to perform is critical – MTM services have not been well defined – Some payers define MTM clearly – Each payer may set a definition of services – Compensation rates vary by payer, important you understand services you perform & rate to be paid for that service MTM as a Health Care Service • Medicare Modernization Act & Health Information Portability and Accountability Act (HIPAA) have assisted in providing guidance for MTM reimbursement • HIPAA requires that all health care service billing done through CMS 1500 form – ICD-9 codes have specific reimbursement eligibility – Most CMS 1500 is electronic, but can use paper Medicare Part D Required MTM forms (as of 1/1/13) • Medicare Part D requires use of CMS Standardized Format: – Cover letter – Medication Action Plan (MAP) – Personal medication list for the comprehensive medication review Can be downloaded at: http://www.cms.gov/Medicare/Prescription-DrugCoverage/PrescriptionDrugCovContra/MTM.html MTM documentation/billing systems • MirixaPro, founded by the National Community Pharmacists Association (www.mirixa.com) • OutcomesMTM System (www.getoutcomes.com) • ConXus MTM, from Protocol Driven Healthcare, Inc. (www.pdhi.com) • Medication Management Systems/Assurance Pharmaceutical Care Documentation Software, from the University of Minnesota Peters Institute of Pharmaceutical Care (www.medsmanagement.com) • Medication Pathfinder, from Clinical Support Software (www.medicationpathfinder.com) • MTM 360, from Elsevier Clinical Decision Support (www.goldstandard.com/product/medication-therapy-management/mtm-360) • PharmMD, from PharmMD (www.pharmmd.com) • IQ Ware (www.iqwareinc.com) Billing Strategies for MTM • Outside of Medicare/Medicaid • Must have private pay rate defined to use as measuring stick for complexity of patients • CPT Codes for MTM as of January 2008 Differentiating Product from Service Medication Therapy Management Drug Regimen Review Patient Care Patient Education Prescriptions Product AMA Current Procedural Terminology (CPT) Medication Therapy Management (MTM) MTM describes face to face patient assessment and intervention as appropriate, by a pharmacist, upon request. MTM is provided to optimize the response to medications or to manage treatment related medication interactions or complications. MTM includes the following documented elements: review of the pertinent patient history, medication profile (prescription and nonprescription), and recommendations for improving health outcomes and treatment compliance. These codes are not to be used to describe the provision of product specific information at the point of dispensing or any other routine dispensing related activities. 99605 Medication therapy management service(s) provided by a pharmacist, individual, face to face with patient, with assessment and intervention if provided; initial 15 minutes, new patient 99606 initial 15 minutes, established patient 99607 each additional 15 minutes (List separately in addition to code for primary service) MEDICATION THERAPY MANAGEMENT SERVICES: Level of Service Provided Assessment of Drug -related Needs Identification Drug Therapy Problems Complexity of Care Planning & Follow -up Evaluation CPT Category III Codes b Level #1 Level #3 Level #4 Level #5 Detailed Expanded Detailed a Comprehensive 2 Medications 3-5 Medications 6-8 Medications =9 Medications Problem -focused Expanded Problem Detailed Expanded Detailed Comprehensive 0 Drug Therapy Problems 1 Drug Therapy Problem 2 Drug Therapy Problems 3 Drug Therapy Problems =4 Drug Therapy Problems Straightforward Straightforward Low Complexity Moderate Complexity High Complexity 1 Medical Condition 1 Medical Condition 2 Medical Conditions 3 Medical Conditions =4 Medical Conditions 99605 initial encounter with a new patient c 99605 (or 99606 99605 (or 99606 99605 (or 99606 99605 (or99606) Problem -focused Level #2 Resource -based Relative Value Scale Expanded Problem a 1 Medication (or 99606 for all follow -up encounters) and and and and 99607 2 X 99607 3 X 99607 >4 X 99606 Face -to-face Time 15 minutes 16-30 minutes 31-45 minutes 46-60 minutes >60 minutes Amount $32 $25 $76 $58 $100 $82 $124 $106 $148 $130 Mechanisms for Reimbursement • • • • • • • Fee-for-Service Contracted Service Prescription Drug Plan (Medicare Part D) Health Plan (fee schedule) Physician Practice (“Incident-To” – Level 1) At Risk Contracts (Point of Service) Currently cannot bill Medicare Part B as independent provider Additional Billing Strategies • Dependent on practice model • “Incident to” billing – i.e. Medicare Part B, use MD CPT codes – requires direct supervision of MD, “integral but incidental” to MD care – Not guaranteed, may be lower level of payment • Per member per month (PMPM) or Per Enrollee (or utilizing member) per month – Working with employers – At risk contract (capitated) Critical Goal: Medicare Part B Eligible Provider Status Report to the Surgeon General “The 2011 Report provides rationale and compelling discussion to support health reform through pharmacists currently delivering expanded patient care services.” Report to the Surgeon General • Focus Point 1: “pharmacists are already integrated into primary care as health care providers – However, pharmacists may be the only health professionals (that manage disease through medications and provide other patient care services) that are not recognized in national health policy as health care providers or practitioners.” Report to the Surgeon General • Focus Points 2 & 3: “pharmacists must be recognized as health care providers by statute via legislation and policy, and compensated commensurate with level of services provided” • Focus Point 4: “thousands of articles, systematic reviews and meta-analyses of positive patient and health system outcomes have been published that validate this model as evidencebased” Objectives of Surgeon General Report • Obtain advocacy from the U.S. Surgeon General to: – Acknowledge pharmacists that manage disease through medication use and deliver patient care services, as an accepted and successful model of health care delivery in the United States – Amend the Social Security Act to include pharmacists among health care professionals classified as “health care providers.” – Have pharmacists recognized by CMS as Non-Physician Practitioners in CMS documents, policies, and compensation tables Keys to Reimbursement Success • Build relationships!!! – Provider & patient relationships critical – Offer yourself as a resource to providers, payers, legislators – Learn strategies from other providers • The only thing harder than taking care of patients is billing for the service – look for resources that can assist you. • Reimbursement texts: – ASHP Guidelines for Implementing & Obtaining Compensation for Clinical Services by Pharmacists www.ashp.com/bestpractices/pharm-mgmt – “The Pharmacist’s Guide to Compensation for Patient Care Services” Michael D. Hogue, PharmD • Released by APhA www.pharmacist.com – “How to Bill for Clinical Pharmacy Services” • ACCP publication www.accp.com/strhowtobill Conclusions • Pharmacists can be valuable members of PCMH, but are underutilized resource • MTM services improve outcomes, reduce health costs • MTM services are eligible and capable of being reimbursed with and without a CDTM agreement. • CDTM agreements may enhance reimbursement options for MTM services. • Federal recognition of pharmacist provider should reduce confusion of payers toward reimbursement • There are no limitations on the delivery of MTM services to patients by pharmacists; but liability increases Thank You! Questions . . . and some answers? thomas.e.buckley@uconn.edu