Complex Regional Pain Syndrome (CRPS)
advertisement
")
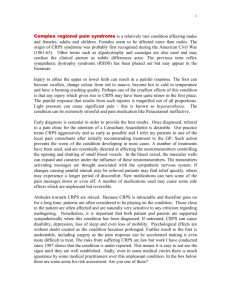
Neurology Blueprint PANCE/PANRE Review Diseases of the Peripheral Nerves Complex Regional Pain Syndrome (CRPS) CRPS frequently begins after surgery, injury, vascular event such as stroke. Another name for CRPS reflex sympathetic dystrophy. Two Types of CRPS: 1. Type I- corresponds with patients with CRPS without a definable nerve lesion in represents most clinical presentations. 2. Type II- refers to patients with CRPS where there is a definable nerve lesion. Complex Regional Pain Syndrome (CRPS) Three Stages of CRPS: 1. Stage 1-Occurs either after an event or without an apparent cause. The patient develops pain in a limb. The common symptoms are: burning, throbbing pain, diffuse, uncomfortable achy, insensitivity to cold or touch, localized edema. 2. Stage 2-is marked by a progression of soft tissue edema, thickening of skin, and articular soft tissues. There is muscle wasting, and the development of brawny skin. This stage typically takes 3 to 6 months. 3. Stage 3- the third stage is most severe. It is characterized my limitation of movement, contractures of the digits, waxy trophic skin changes, and brittle nails. The longer a patient is in Stage 3, the harder it is to reverse the clinical course with any type of intervention. Complex Regional Pain Syndrome (CRPS) Using Laboratory & Diagnostic Studies: -Plain radiographs, CT scans, and MRI may show late findings of the disease. -Plain radiographs often will show osteopenia -MRI may show soft tissue edema, skin thickening, and muscle atrophy -CT scan may show areas of osteoporosis in a swiss cheese appearance that is consistent with stage III. Complex Regional Pain Syndrome (CRPS) Formulating Most Likely Diagnosis: -Diagnosis of CRPS early is difficult do to lack of objective findings. -Autonomic testing and scintigraphy may provide an early clue in the diagnosis. Radiographic studies can be helpful later on in the diagnosis. -The patients response to treatment often is the best diagnostic test. -Differential diagnosis includes: Central nerve root impingement, Pancoast syndrome, vasculitis, migratory osteolysis, arteriovenous fistula, progressive systemic sclerosis, thoracic outlet syndrome, RA, peripheral neuropathy, venous thrombosis, diffuse atrophy, and angioedema. Complex Regional Pain Syndrome (CRPS) Health Maintenance: -Early mobilization may reduce the risk of development of CRPS. -Supplementation with Vitamin C has been used as another preventive measure in fractures for reducing the risk of CRPS. Complex Regional Pain Syndrome (CRPS) Clinical Intervention: -Sympathetic regional nerve block used to be the hallmark for diagnosis of CRPS. It is no longer considered the gold standard. -Patients that have had physical and occupational therapy with CPRS had better pain control but no difference in range of motion after one year. -Cigarette smoking is a risk factor for CRPS so cessation is recommended. -Other clinical interventions include: tender point injections, nerve stimulation and epidural clonidine. Complex Regional Pain Syndrome (CRPS) Pharmaceutical Therapeutics: -Several medications have been show to be better than placebo in clinical trials with CRPS. These medications include: anticonvulsants, biphosphonates, oral glucocorticoids, and nasal calcitonin -Antidepressants are often effective in reducing neuropathic pain -Guidelines developed for CRPS include treating with antidepressant such as elavil, an anticonvulsant such as neurontin, an NSAID, and opioids for those with severe pain. -Other strategies that have been used include nerve blocks with clondine and bretylium or lidocaine and labetolol combination. Complex Regional Pain Syndrome (CRPS) Applying Basic Science Concepts: -The pathogenesis of complex regional pain syndrome is unclear, but is thought to involve formation of a reflex arc after an inciting event. -the pain sensation response to Injury may lead to increased sensitivity of increased axons to epinephrine and other substances released by local sympathetic nerves. Peripheral Neuropathies History Taking & Performing Physical Exam: -Peripheral neuropathy refers to generalized, homogenous process affecting many peripheral nerves, with the distal nerves are affected most prominently. Tend to occur in a glove and stocking distribution. -Physical exam findings are dependent on type if axonal or demyelinating. -Patients with axonal neuropathy, motor exam may disclose some wasting of intrinsic muscles of the feet or lower leg. Distal loss of sensation to pin prick, light touch, vibration cold, and proprioception may occur. Reflexes may be hypoactive. Peripheral Neuropathies -Generalized weakness is the usual presentation for patients presenting with fulminant polyneuropathy secondary to demyelination process. Sensation is also reduced. Vibratory and proprioception are also out of proportion to loss of pin prick and temperature sensation. -Patients with axonal neuropathy tend to present over year. -Patients with inflammatory demyelinating polyneuropathy are variable. Patients with Guillain Barre Syndrome a 2-6 weeks decline is followed by stabilization. Peripheral Neuropathies Using Laboratory & Diagnostic Studies: -EMG’s can be used to help diagnose peripheral neuropathy but are only needed if the symptoms are severe and rapidly progressing or no clear etiology. -Routine lab evaluation CBC, Thyroid Panel, Folate, Vitamin B12 levels. -Nerve biopsy is occasionally helpful for diagnosing etiology of peripheral neuropathy to determine if it is axonal or demyelinating. Peripheral Neuropathies Formulating Most Likely Diagnosis: -Differential diagnosis includes spinal cord process, acute myopathy, neuromuscular junction disease, or central process may mimic GBS. -Abnormal EMG have the highest specificity in case of neuropathy. It should not be used only. Patients need EMG’s if there is no clear etiology or when symptoms are severe and rapidly progressive. Peripheral Neuropathies Health Maintenance: -Patients that suffer from diabetic neuropathy need aggressive management of the blood sugar and HgA1C -Patients with hypothyroidism need to have thyroid replacement. -Patients with Vitamin B12 and Folate Deficiencies need to have that replaced. -Patients with toxic exposure due to alcohol abuse or heavy metals need to avoid contact with those substances. Peripheral Neuropathies Clinical Intervention: -Reducing exposure to the exogenous or endogenous toxin in the most important step with axonal neuropathies. -Patients with diabetic neuropathy need aggressive management of their blood sugar. -Thyroid replacement generally helps neuropathy due to hypothyroidism -The mainstays of treatment with patients with demyelinating neuropathies with chronic inflammatory peripheral neuropathy are IV immunoglobulin, glucocorticoids, and plasma exchange. Peripheral Neuropathies Pharmaceutical Therapeutics: -Patients with painful neuropathy have shown response to various medications such as: neurontin, tegretol, dilantin, topamax, baclofen, lyrica, elavil, and cymbalta. -Patients with break through pain are sometimes given NSAIDS or Ultram. Peripheral Neuropathies Applying Basic Science Concepts: -Peripheral neuropathy has a variety of causes: diabetes, alcohol abuse, HIV infection, Charcot Marie Tooth Disease -Diabetic peripheral neuropathy is most common and is predominantly axonal. The mechanism that causes this is related to inflammatory, metabolic and ischemic effects. -Other systemic disease cause peripheral neuropathies: amyloidosis, hypothyroidism, Vitamin B12 and Folate deficiency, and Lyme Disease -Many neuropathies are toxic such as due to chemotherapy, heavy metals, and alcohol abuse. -Some neuropathies can be environmental induced from vibration or even be idiopathic.