Monitoring Pulse Oximetry - The Kansas Board of Emergency
advertisement

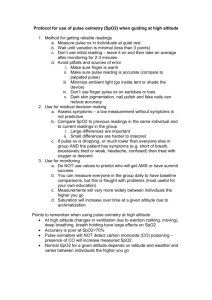
Monitoring Pulse Oximetry By the EMT-Basic Objectives Understand the Kansas Regulations relative to monitoring pulse oximetry by the EMT-B Review the signs and symptoms of respiratory compromise Understand the importance of adequate tissue perfusion Define hypoxia and describe the clinical signs and symptoms continued Describe the technology of the pulse oximeter Define normal parameters of oxygen saturation Describe the relationship between oxygen saturation and partial pressure oxygen Describe the significance of the information provided by pulse oximetry Describe monitoring pulse oximetry during patient assessment continued Describe the use of pulse oximetry with pediatrics Describe patient conditions that may affect pulse oximetry accuracy Describe patient environments that may affect pulse oximetry accuracy Describe the evaluation and documentation of pulse oximetry monitoring Kansas Regulations Regulation 109-6-4 Adopts “EMT-Basic Advanced Initiatives” Allows EMTs to monitor saturation of arterial oxygen levels of blood by way of pulse oximetry Appropriate physician oversight On line medical control or written protocols Complete a course of instruction Respiratory Compromise Signs and Symptoms Dyspnea Accessory muscle use Inability to speak in full sentences Adventitious breath sounds Increased or decreased breathing rates Shallow breathing Flared nostrils or pursed lips continued Retractions Upright or tripod position Unusual anatomy changes Hypoxemia Decreased oxygen in arterial blood Results in decreased cellular oxygenation Anaerobic metabolism Loss of cellular energy production Hypoxemia Etiology Inadequate External Respiration Inadequate Oxygen Transport Decreased on-loading of oxygen at pulmonary capillaries Decreased oxygen carrying capacity Inadequate Internal Respiration Decreased off-loading of oxygen at cellular capillaries External Respiration Exchange of gases between the alveoli and pulmonary capillaries Oxygen diffuses from an area of higher concentration to an area of lower oxygen concentration Oxygen must be available and must be able to diffuse across alveolar and capillary membranes Oxygen must be able to saturate the hemoglobin Inadequate External Respiration Decreased oxygen available in the environment Smoke inhalation Toxic gas inhalation High altitudes Enclosures without outside ventilation Inadequate mechanical ventilation Pain Rib fractures Pleurisy continued Traumatic injuries Open pneumothorax Crushing injuries of the neck and chest Increased intrathoracic pressures reducing ventilation Hemothorax Traumatic asphyxia Crushing neck injuries Tension pneumothorax Loss of ability to change intrathoracic pressures Blood in thoracic cavity reducing lung expansion Flail Chest Loss of ability to change intrathoracic pressures continued Other conditions Upper Airway Obstruction Epiglottitis Croup Airway Edema-anaphylaxis Lower Airway Obstructions Asthma Airway Edema from inhalation of toxic substances continued Hypoventilation Muscle Paralysis Drug Overdose Spinal injuries Paralytic drug for intubation Respiratory depressants Brain Stem Injuries Damage to the respiratory center continued Inadequate oxygen diffusion Pulmonary edema Fluid between alveoli and capillaries inhibit diffusion Pneumonia Consolidation reduces surface area of respiratory membranes Reduces the ventilation-perfusion ratio COPD Air trapping in alveoli Loss of surface area of respiratory membranes continued Pulmonary emboli Area of the lung is ventilated but hypoperfused Loss of functional respiration membranes Oxygen Transport Most of the oxygen in arterial blood is saturated on hemoglobin Red blood cells must be adequate in number and have adequate hemoglobin Sufficient circulation is necessary to transport oxygen to the cellular level Inadequate Oxygen Transport Anemia Poisoning Reduces red blood cells reduce oxygen carrying capacity Inadequate hemoglobin results in the loss of oxygen saturation Carbon monoxide on-loads on the hemoglobin more readily preventing oxygen saturation and oxygen carrying capacity Shock Low blood pressures result in inadequate oxygen carrying capacity Internal Respiration Exchange of gases from the systemic capillaries to the tissue cells Oxygen must be able to off-load the hemoglobin Oxygen moves from a area of higher concentration to an area of lower concentration of oxygen Inadequate Internal Respiration Shock Cellular environment is not conducive to off-loading oxygen Oxygen is not available due to massive peripheral vasoconstriction or micro-emboli Acid Base Imbalance Lower than normal temperature Poisoning CO will reduce the oxygen available at the cellular level Signs and Symptoms of Hypoxemia Restlessness Altered or deteriorating mental status Increased or decreased pulse rates Increased or decrease respiratory rates Decreased oxygen oximetry readings Cyanosis (late sign) Pathophysiology Oxygen is exchanged by diffusion from higher concentrations to lower concentrations Most of the oxygen in the arterial blood is carried bound to hemoglobin 97% of total oxygen is normally bound to hemoglobin 3% of total oxygen is dissolved in the plasma Oxygen Saturation Percentage of hemoglobin saturated with oxygen Normal SpO2 is 95-98% Suspect cellular perfusion compromise if less than 95% SpO2 Insure adequate airway Provide supplemental oxygen Monitor carefully for further changes and intervene appropriately continued Suspect severe cellular perfusion compromise when SpO2 is less than 90% Insure airway and provide positive ventilations if necessary Administer high flow oxygen Head injured patients should never drop below 90% SpO2 SpO2 and PaO2 SpO2 indicates the oxygen bound to hemoglobin Closely corresponds to SaO2 measured in laboratory tests SpO2 indicates the saturation was obtained with non-invasive oximetry PaO2 indicates the oxygen dissolved in the plasma Measured in ABGs continued Normal PaO2 is 80-100 mmHg Normally 80-100 mm Hg corresponds to 95-100% SpO2 60 mm Hg corresponds to 90% SpO2 40 mm Hg corresponds to 75% SpO2 Technology The pulse oximeter has Light-emitting diodes (LEDs) that produce red and infrared light LEDs and the detector are on opposite sides of the sensor Sensor must be place so light passes through a capillary bed Requires physiological pulsatile waves to measure saturation Requires a pulse or a pulse wave (Adequate CPR) continued Oxygenated blood and deoxygenated blood absorb different light sources Oxyhemoglobin absorbs more infrared light Reduced hemoglobin absorbs more red light Pulse oximetry reveals arterial saturation my measuring the difference. Patient Assessment Patient assessment should include all components Scene Size-up Initial Assessment Rapid Trauma Assessment or Focused Physical Exam Focused History Vital Signs Detailed Assessment Ongoing Assessment Pulse Oximetry Monitoring Pulse oximetry monitoring is NOT intended to replace any part of the patient assessment Pulse oximetry is a useful adjunct in assessing the patient’s oxygenation and monitoring treatment interventions Initiate pulse oximetry immediately prior to or concurrently with oxygen administration Continuous Monitoring Monitor current oxygenation status and response to oxygen therapy Monitor response to nebulized treatments Monitor patient following intubation Monitor patient following positioning patients for stabilization and transport Decreased circulating oxygen in the blood may occur rapidly without immediate clinical signs and symptoms Pediatrics Use appropriate sized sensors Active movement may cause erroneous readings Adult sensors may be used on arms or feet Pulse rate on the oximeter must coincide with palpated pulse Poor perfusion will cause erroneous readings Treat patient according to clinical status when in doubt Pulse oximetry is useless in pediatric cardiac arrest Conditions Affecting Accuracy Patient conditions Carboxyhemoglobin Anemia Hypovolemia/Hypotension Hypothermia Carboxyhemoglobin Carbon monoxide has 200-250 greater affinity for the hemoglobin molecule than oxygen Binds at the oxygen binding site Prevents on-loading of oxygen Fails of readily off-load at the tissue cells Carboxyhemoglobin can not be distinguished from oxyhemoglobin by pulse oximetry Erroneously high reading may present continued Suspect the presence of carboxyhemoglobin in patient with: Smoke inhalation Intentional and accidental CO poisoning Heavy cigarette smoking Treat carboxyhemoglobin with high flow oxygen irregardless of the pulse oximetry reading! Anemia Low quantities of erythrocytes or hemoglobin Normal value of hemoglobin is 11-18 g/dl Values as low as 5 g/dl may result in 100% SpO2 Anemic patients require high levels of oxygen to compensate for low oxygen carrying capacities! Hypovolemia/Hypotension Adequate oxygen saturation but reduced oxygen carrying capacity Vasoconstriction or reduction in cardiac output may result in loss of detectable pulsatile waveform at sensor site Patients in shock or receiving vasoconstrictors may not have adequate perfusion to be detected by oximetry Always administer oxygen to patients with poor perfusion! Hypothermia Severe peripheral vasoconstriction may prevent oximetry detection Shivering may result in erroneous oximetry motion Pulse rate on oximeter must coincide with palpable pulse rate to be considered accurate Treat the patient according to hypothermic guidelines and administer oxygen accordingly! Patient Environments Ambient Light Excessive Motion Ambient Lighting Any external light exposure to capillary bed where sampling is occurring may result in an erroneous reading Most sensors are designed to prevent light from passing through the shell Shielding the sensor by covering the extremity is acceptable Excessive Motion New technology filters out most motion artifact Always compare the palpable pulse rate with the pulse rate indicated on the pulse oximetry If they do not coincide, reading must be considered inaccurate Other Concerns Fingernail polish and pressed on nails Most commonly use nails and fingernail polish will not affect pulse oximetry accuracy Some shades of blue, black and green may affect accuracy (remove with acetone pad) Metallic flaked polish should be removed with acetone pad The sensor may be placed on the ear if reading is affected continued Skin pigmentation Apply sensor to the fingertips of darkly pigmented patients. Interpreting Pulse Oximetry Assess and treat the PATIENT not the oximeter! Use oximetry as an adjunct to patient assessment and treatment evaluation NEVER withhold oxygen if the patient ahs signs or symptoms of hypoxia or hypoxemia irregardless of oximetry readings! continued Pulse oximetry measures oxygenation not ventilation Pulse oximetry does NOT indicate the removal of carbon dioxide from the blood! Documentation Pulse oximetry is usually documented as SpO2 Distinguishes non-invasive pulse oximetry from SaO2 determined by laboratory testing Document oximetry readings as frequently as other vital signs When oximetry reading is obtained before oxygen administration, designate the reading as “room air” continued When oxygen administration is changed, document the evaluation of pulse oximetry When treatments provided could potentially affect respiration or ventilation, document pulse oximetry Spinal immobilization Shock position Fluid administration Summary As with all monitoring devices, the interpretation of information and response to that interpretation is the responsibility of a properly trained technician! References Bledsoe, B. et al. (2003). Essentials of paramedic care. Upper Saddle River, New Jersey: Prentice Hall. Halstead, D., Progress in pulse oximetry—a powerful tool for EMS providers. JEMS, 2001: 55-66. Henry, M., Stapleton, E. (1997). EMT prehospital care (2nd ed.). Philadelphia: W.B. Saunders. Limmer, D., et al. (2001) Emergency Care (9th ed.). Upper Saddle River, New Jersey: Prentice Hall. Porter, R., et al: The fifth vital sign. Emergency, 1991 22(3): 127-130. Sanders, M., (2001). Paramedic textbook (rev. 2nd ed.). St. Louis: Mosby. Shade, B., et al. (2002). EMT intermediate textbook (2nd ed.). St. Louis: Mosby. Cason, D., Pons, P. (1997) Paramedic field care: a complaint approach. St. Louis: Mosby.