Infection Control for the OB/GYN Surgeon

Infection Control for the OB/GYN
Surgeon
Gonzalo Bearman, MD, MPH
Assistant Professor of Internal Medicine &
Epidemiology
Associate Hospital Epidemiologist
Outline
• Nosocomial Infections are a significant cause of morbidity and mortality
• There has been increased public interest in nosocomial infections
• Shifting paradigm
– Many infections are preventable
• SSI and OB/GYN
– Surveillance data
– Risk factors
– Modifiable risk factors- modifiable interventions
• BSI and OB/GYN
– Surveillane
– Risk reduction strategies
• Proliferation of drug resistant nosocomial pathogens
– Hand Hygeiene and Contact precautions
“11,600 patients got infections in Pa. hospitals “
7/13/2005
"The consequences clearly are huge," says Marc
Volavka, executive director of the Pennsylvania Health
Care Cost Containment
Council, an independent state agency that published the data. "Everyone is paying the bill."
Hospital-acquired infections reported by
Pennsylvania hospitals in 2004:
Infection Number
Urinary tract
Bloodstream
6,139
1,932
Pneumonia
Surgical site
1,335
1,317
Multiple infections 945
Total 11,668
Source: Pennsylvania Health Care Cost Containment
Council
U.S. News and World Report, July 18, 2005.
Shifting Vantage Points on
Nosocomial Infections
Many infections are inevitable, although some can be prevented
Each infection is potentially preventable unless proven otherwise
Gerberding JL. Ann Intern Med 2002;137:665-670 .
Nosocomial Infections
• 5-10% of patients admitted to acute care hospitals acquire infections
– 2 million patients/year
– ¼ of nosocomial infections occur in ICUs
– 90,000 deaths/year
– Attributable annual cost: $4.5 – $5.7 billion
• Cost is largely borne by the healthcare facility not 3 rd party payors
Weinstein RA. Emerg Infect Dis 1998;4:416-420.
Jarvis WR. Emerg Infect Dis 2001;7:170-173.
Nosocomial Infections
• 70% are due to antibiotic-resistant organisms
• Invasive devices are more important than underlying diseases in determining susceptibility to nosocomial infection
Burke JP. New Engl J Med 2003;348:651-656.
Safdar N et al. Current Infect Dis Reports 2001;3:487-495.
Attributable Costs of Nosocomial
Infections
Cost per Infection
Wound infections $3,000 - $27,000
Sternal wound infection $20,000 - $80,000
Catheter-associated
BSI
Pneumonia
$5,000 - $34,000
$10,000 - $29,000
Urinary tract infection $700
Nettleman M. In: Wenzel RP, ed. Prevention and Control of Nosocomial Infections,
4 th ed. 2003:36.
Major Sites of Nosocomial
Infections
• Urinary tract infection
• Bloodstream infection
• Pneumonia (ventilator-associated)
• Surgical site infection
Surgical Site Infections in
Obstetrics and Gynecology
National Nosocomial Infections
Surveillance System (NNIS)
• NNIS is the only national system for tracking
HAIs
• Voluntary reporting system has approximately
300 hospitals
• The NNIS database uses standardized definitions of HAI’s to:
– Describe the epidemiology of HAIs
– Describe antimicrobial resistance associated with
HAIs
– Produce aggregated HAI rates suitable for interhospital comparison http://www.cdc.gov/ncidod/hip/SURVEILL/NNIS.HTM
National Nosocomial Infections
Surveillance System (NNIS)
Classification
Clean
Clean-contaminated:
GI/GU tracts entered in a controlled manner
Contaminated: open, fresh, traumatic wounds infected urine, bile gross spillage from GI tract
Dirty-infected:
Wound Class
0
1
2
3
SSI Risk
Lower
Higher
NNIS- SSI Surveillance 1992-2004
Abdominal Hysterectomy
Risk Index Number of hospitals
Pooled mean rate
Per 100 operations
0 107 1.36
1 100 2.32
2,3 53 5.17
Median- 50% percentile
0.91
1.96
4.21
Am J Infect Control 2004;32:470-85
NNIS- SSI Surveillance 1992-2004
Vaginal Hysterectomy
Risk Index Number of hospitals
Pooled mean rate
Per 100 operations
Median-
50% percentile
0,1,2,3 71 1.31
0.91
Am J Infect Control 2004;32:470-85
NNIS- SSI Surveillance 1992-2004
0
1
Cesarean Section
Risk Index Number of hospitals
Pooled mean rate
Per 100 operations
2,3
130
117
51
2.71
4.14
7.53
Median-
50% percentile
2.17
3.19
5.38
Am J Infect Control 2004;32:470-85
Hospital Morbidity Due to Post-operative
Infections in Obstetrics and Gynecology
• Post operative infections prospectively surveyed from 1997-1998 in tertiary care medical center, Bahrain
– Definition of postoperative infection:
• Fever
• Purulent discharge from wound
– With or without a positive microbiologic culture
• Re-admissions for wound infections were not included in the study
Saudi Medical Journal 2000: Vol 21 (3) 270-273
Hospital Morbidity Due to Post-operative
Infections in Obstetrics and Gynecology
Type of operation
(%)
No. of
Operations
(%)
Cesarean section
Major
Gynecologic
Surgery
2193
1839
Wound
Infection alone (%)
35 (2)
9 (0.4)
Fever alone
(%)
Both wound
Infection and
Fever (%)
30 (1)
5 (0.3)
7 (0.3)
4 (0.2)
Total 4032 35 (0.9) 35 (0.9) 11(0.3)
Saudi Medical Journal 2000: Vol 21 (3) 270-273
Hospital Morbidity Due to Post-operative
Infections in Obstetrics and Gynecology
Number of Isolates Organism
Gram Positive
• S.aureus
•
S.epidermidis
• Streptococci
•
Enterococci
Gram Negative
• Enterbacter
•
Klebsiella
• E.coli
•
Proteus
• P.aeruginosa
•
Acinetobacter
•
Gram negative bacilli
Candida
Total
3 (3)
13 (14)
6(6)
19 (20)
4(4)
14(15)
11(12)
9(10)
8(8.5)
1(1)
1(1)
5(5)
94
Genitourinary flora is a significant source of contamination during surgery
Saudi Medical Journal 2000: Vol 21 (3) 270-273
Risk Factors for Surgical Site Infections
Following Cesarean Section
• OBJECTIVE: To identify risk factors associated with surgical-site infections (SSIs) following cesarean sections.
• DESIGN: Prospective cohort study.
• SETTING: High-risk obstetrics and neonatal tertiary-care center in upstate New York.
• METHODS:
• Prospective surgical-site surveillance was conducted using methodology of the National Nosocomial
Infections Surveillance System.
• Infections were identified on admission, within 30 days following the cesarean section, by readmission to the hospital or by a postdischarge survey.
• Multiple logistic-regression analysis used for risk factor identification
Infect Control Hosp Epidemiol. 2001 Oct;22(10):613-7
Risk Factors for Surgical Site Infections
Following Cesarean Section
Multiple logistic-regression analysis
Risk Factor Odds Ratio/ 95% CI/ P value
2.63; 1.50-4.6; P=.008
Absence of antibiotic prophylaxis
Length surgery
<7 prenatal visits
Duration of ruptured membranes
1.01; 1.00-1.02; P=.04
3.99; 1.74-9.15; P=.001
1.02; 1.01-1.03; P=.04
Infect Control Hosp Epidemiol. 2001 Oct;22(10):613-7
Summary: SSI’s in OB/GYN
• NNIS- SSIs are reported to occur in 1%-
7% of OB/GYN surgeries
• SSI are typically caused by maternal cutaneous or endometrial/vaginal flora
• When an exogenous source is the cause of SSI in the obstetrical patient,
S.aureus
is frequently implicated
Preventing Surgical Site Infections
Focus on modifiable risk factors
Sources of SSIs
• Endogenous: patient’s skin or mucosal flora
– Increased risk with devitalized tissue, fluid collection, edema, larger inocula
• Exogenous
– Includes OR environment/instruments, OR air, personnel
• Hematogenous/lymphatic: seeding of surgical site from a distant focus of infection
– May occur days to weeks following the procedure
• Most infections occur due to organisms implanted during the procedure
Up to 20% of skin-associated bacteria in skin appendages (hair follicles, sebaceous glands) & are not eliminated by topical antisepsis. Transection of these skin structures by surgical incision may carry the patient's resident bacteria deep into the wound and set the stage for subsequent infection.
Downloaded from: Principles and Practice of Infectious Diseases
© 2004 Elsevier
Risk Factors for SSI
• Duration of pre-op hospitalization
* increase in endogenous reservoir
• Pre-op hair removal
* esp if time before surgery > 12 hours
* shaving>>clipping>depilatories
• Duration of operation
*increased bacterial contamination
* tissue damage
* suppression of host defenses
* personnel fatigue
SCIP
• A national partnership of organizations to improve the safety of surgical care by reducing post-operative complications through a national campaign
• Goal: reduce the incidence of surgical complications by 25 percent by the year 2010
• Initiated in 2003 by the Centers for Medicare &
Medicaid Services (CMS) & the Centers for Disease
Control & Prevention (CDC)
– Steering committee of 10 national organizations
– More than 20 additional organizations provide technical expertise
Putting risk reduction guidelines into practice
SCIP Steering Committee
Organizations
• Agency for Healthcare Research and Quality
• American College of Surgeons
• American Hospital Association
• American Society of Anesthesiologists
• Association of periOperative Registered Nurses
• Centers for Disease Control and Prevention
• Centers for Medicare & Medicaid Services
• Department of Veterans Affairs
• Institute for Healthcare Improvement
• Joint Commission on Accreditation of Healthcare
Organizations
SCIP Performance Measures
Surgical infection prevention
• SSI rates
• Appropriate prophylactic antibiotic chosen
• Antibiotic given within 1 hour before incision
• Discontinuation of antibiotic within 24 hours of surgery
• Glucose control
• Proper hair removal
• Normothermia in colorectal surgery patients
Monetary incentives for promoting quality and compliance with SSI risk reduction guidelines:
March 12, 2005
In recent years, the healthcare industry has placed a stronger emphasis on reducing medical errors, monitoring everything from how long doctors sleep to whether or not their handwriting is legible.
Now one organization is not only recognizing the hospitals that follow patient safety and clinical guidelines, but rewarding them for doing so. Anthem Blue Cross and Blue Shield recently gave a total of $6 million to 16 Virginia hospitals as part of the company's new Quality-In-Sights Hospital Incentive Program
(Q-HIP).
http:// www.richmond.com
ID=15
Downloaded from: Principles and Practice of Infectious Diseases
Process Indicators:
Appropriate Antibiotic Prophylaxis
Procedure Approved Antibiotics
Hysterectomy
•Cefazolin
•Cefoxitin
Approved for β-lactam allergy
•Clindamycin + gentamicin
•Clindamycin + levofloxacin
•Metronidazole + gentamicin
•Metronidazole + levofloxacin
•Clindamycin
Process Indicators:
Duration of Antimicrobial Prophylaxis
Prophylactic antimicrobials should be discontinued within 24 hrs after the end of surgery
Bratzler DW et al. Clin Infect Dis 2004;38:1706-15.
Process Indicators:
Timing of First Antibiotic Dose
Infusion should begin within 60 minutes of the incision
Bratzler DW et al. Clin Infect Dis 2004;38:1706-15.
Nosocomial Bloodstream Infections
Nosocomial Bloodstream Infections,
1995-2002
Rank Pathogen Percent
N= 24,847
52 BSI/10,000 admissions
5
6
7
3
4
8
9
1
2
Coagulase-negative Staph
S. aureus
Enterococci
Candida spp
E. coli
Klebsiella spp
Pseudomonas aeruginosa
Enterobacter spp
Serratia spp
10 Acinetobacter spp
31.3%
20.2%
9.4%
9.0%
5.6%
4.8%
4.3%
3.9%
1.7%
1.3%
Edmond M. SCOPE Project .
Nosocomial Bloodstream Infections,
1995-2002
Obstetrics and Gynecology
N= 24,847
52 BSI/10,000 admissions
•Proportion of all BSI 0.9% (n=209)
• E.coli (33%)
• S.aureus ( 11.7%)
• Enterococci (11.7)
In obstetrics, BSIs are uncommon.
However, the principal pathogen is
E.coli and not coagulase negative staphylococci.
The source is typically genitourinary
Edmond M. SCOPE Project .
Nosocomial Bloodstream Infections
• 12-25% attributable mortality
• Risk for bloodstream infection:
BSI per 1,000 catheter/days
Subclavian or internal jugular CVC 5-7
Hickman/Broviac (cuffed, tunneled)
PICC
1
0.2 - 2.2
Risk Factors for Nosocomial BSIs
• Heavy skin colonization at the insertion site
• Internal jugular or femoral vein sites
• Duration of placement
• Contamination of the catheter hub
Prevention of Nosocomial BSIs
• Coated catheters
– In meta-analysis C/SS catheter decreases BSI
(OR 0.56, CI95 0.37-0.84)
– M/R catheter may be more effective than C/SS
– Disadvantages: potential for development of resistance; cost (M/R > C/SS > uncoated)
• Use of heparin
– Flushes or SC injections decreases catheter thrombosis, catheter colonization & may decrease BSI
Prevention of Nosocomial BSIs
• Limit duration of use of intravascular catheters
– No advantage to changing catheters routinely
• Change CVCs to PICCs when possible
• Maximal barrier precautions for insertion
– Sterile gloves, gown, mask, cap, full-size drape
– Moderately strong supporting evidence
• Chlorhexidine prep for catheter insertion
30%-40% of all Nosocomial
Infections are Attributed to
Cross Transmission-
Implication For The Spread
Drug Resistant Pathogens
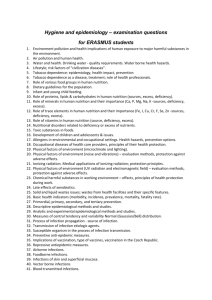
NNIS: Selected antimicrobial resistant pathogens associated with HAIs
Fig 1. Selected antimicrobial-resistant pathogens associated with nosocomial infections in
ICU patients, comparison of resistance rates from January through December 2003 with
1998 through 2002, NNIS System.
Am J Infect Control 2004;32:470-85
Antimicrobial Resistant
Pathogens of Ongoing Concern
• Vancomycin resistant enterocci
– 12% increase in 2003 when compared to 1998-2002
• MRSA
– 12% increase in 2003 when compared to 1998-2002
– Increased reports of Community-Acquired MRSA
• Cephalosporin and Imipenem resistant gram negative rods
– Klebsiella pneumonia
–
Pseudomonas aeruginosa
Am J Infect Control 2004;32:470-85
Transfer of VRE via HCW Hands
16 transfers (10.6%) occurred in 151 opportunities.
•
13 transfers occurred in rooms of unconscious patients who were unable to spontaneously touch their immediate environment
Duckro et al. Archive of Int Med. Vol.165,2005
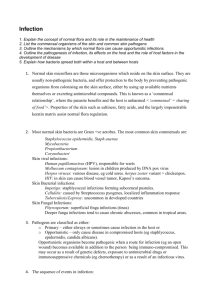
The inanimate environment is a reservoir of pathogens
X represents a positive Enterococcus culture
The pathogens are ubiquitous
~ Contaminated surfaces increase cross-transmission ~
Abstract: The Risk of Hand and Glove Contamination after Contact with a VRE (+) Patient Environment. Hayden M, ICAAC, 2001, Chicago, IL.
Community-associated methicillinresistant Staphylococcus aureus in hospital nursery and maternity units.
• Outbreak of 7 cases of skin and soft tissue infections due to a strain of CA-MRSA.
– All patients were admitted to the labor and delivery, nursery, or maternity units during a 3-week period.
– Genetic fingerprinting showed that the outbreak strain was closely related to the
USA 400 strain that includes the midwestern strain MW2
Emerg Infect Dis. 2005 Jun;11(6):808-13 .
Table 1. Clinical information for patients with methicillin-resistant Staphylococcus aureus infection during the outbreak period
Patient
Age at onset Sex Strain Infection type Initial therapy Definitive therapy
P1, newborn
P2, newborn
P3, mother
P4, newborn
P5, newborn
P6, newborn
P7, newborn
P8, mother
8 d
13 d
33 y
2 d
4 d
2 d
1 d
24 y
F USA 400
F USA 400
F USA 400
Preseptal cellulitis
Omphalitis, otitis externa
Breast abscess
Nafcillin, cefotaxime
Ampicillin, cefotaxime
Cefazolin
M USA 400 Omphalitis, pustulosis Nafcillin Gentamicin
M USA 400
M USA 400
Pustulosis
Pustulosis
F
F
USA 400
Unique
Pustulosis, mastitis
Peripheral IV catheter site
Cephalexin
None
Topical mupirocin
Cefazolin
Topical gentamicin
Topical mupirocin
Surgical drainage, vancomycin, topical mupirocin
Gentamicin, topical mupirocin
Topical bacitracin
Local wound care
Vancomycin
Trimethoprim-sulfamethoxazole, catheter removal
Emerg Infect Dis. 2005 Jun;11(6):808-13.
Epidemic of Staphylococcus aureus nosocomial infections resistant to methicillin in a maternity ward
• Seventeen cases were recorded over a nineweek period (two cases per week).
– All were skin and soft tissue infections
• Pulsed field gradient gel electrophoresis confirmed the clonal character of the strain.
• No definite risk factors were determined by a case-control study.
• Environmental factors were considered key in the persistence of this MRSA outbreak.
Pathol Biol (Paris). 2001 Feb;49(1):16-22.
The inanimate environment is a reservoir of pathogens
Recovery of MRSA, VRE, C.
diff CNS and GNR
Devine et al. Journal of Hospital Infection. 2001;43;72-75
Lemmen et al Journal of Hospital Infection. 2004; 56:191-197
Trick et al. Arch Phy Med Rehabil Vol 83, July 2002
Walther et al. Biol Review, 2004:849-869
The inanimate environment is a reservoir of pathogens
Recovery of MRSA, VRE, CNS. C.
diff and GNR
Devine et al. Journal of Hospital Infection. 2001;43;72-75
Lemmen et al Journal of Hospital Infection. 2004; 56:191-197
Trick et al. Arch Phy Med Rehabil Vol 83, July 2002
Walther et al. Biol Review, 2004 :849-869
The inanimate environment is a reservoir of pathogens
Recovery of MRSA, VRE, CNS. C.
diff and GNR
Devine et al. Journal of Hospital Infection. 2001;43;72-75
Lemmen et al Journal of Hospital Infection. 2004; 56:191-197
Trick et al. Arch Phy Med Rehabil Vol 83, July 2002
Walther et al. Biol Review, 2004:849-869
Alcohol based hand hygiene
Quick
solutions
Easy to use
Very effective antisepsis due to bactericidal properties of alcohol
Hand Hygiene
• Single most important method to limit cross transmission of nosocomial pathogens
• Multiple opportunities exist for HCW hand contamination
– Direct patient care
– Inanimate environment
• Alcohol based hand sanitizers are ubiquitous
– USE THEM BEFORE AND AFTER PATIENT
CARE ACTIVITIES
Contact
Precautions for drug resistant pathogens.
Gowns and gloves must be worn upon entry into the patient’s room
Conclusion
• Nosocomial Infections are a significant causes of morbidity and mortality
• There has been increased public interest in nosocomial infections- this will likely result in greater compliance with IC guidelines
• Shifting paradigm
– Many infections are preventable
• SSI and OB/GYN
– 1-7 % of all OB/GYN procedures (NNIS)
– Increased scrutiny of compliance with risk reduction intervention
– Preoperative antibiotics: choice, timing, discontinuation;
• BSI and OB/GYN
– BSI is less common than in Medicine/Surgical services
– Risk reduction strategies should include appropriate use and prompt removal of invasive devices
• Proliferation of drug resistant nosocomial pathogens
– Importance of Hand Hygiene and Contact precautions