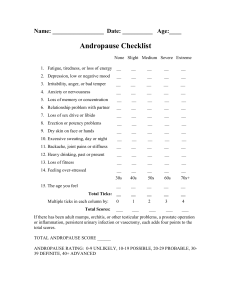
Andropause and Menopause April 19
advertisement

“Hormones for MEN” → Male Menopause → Andropause → PADAM Partial Androgen Deficiency Aging Men Condition may affect millions, but symptoms are rarely recognized Public awareness campaign launched to help them-SARCASM 2 page ad in Time. In last several years, lots of ads in Money, Forbes, and various magazines. “testosterone running on empty” Video game at Endocrine Meeting since 2003- several drug Co many marketing Test Primary Care Journals Doctors told screen symptoms ↓ T • Andropause • Top Male Enhancement Products Reviewed. See Our Readers Poll Results. • TheMansChoice.com/Andropause • Andropause • We Tested Andropause. Read our Investigative Report. • www.mentested.com • Top 5 Male Formulas Rated • What Products Boost Drive,Enhance Maleness & Support Youthful Levels? • www.TheArticleInsiders.com • • • • andropause Symptoms, Causes & Treatments. Free Info on Erectile Dysfunction. Healthline.com See your message here “Hormones for MEN” “testosterone running on empty” Video game at Endocrine Meeting since 2003- several drug Co many marketing Test Primary Care Journals Doctors told screen symptoms ↓ T Ads paid by Unimed, a part of Belgian conglomerate (Solvay) Make Androgel – FDA approved In 2000 Fastest growing T replacement therapy for men Pills (introduced in the 60’s) – often causes liver damage IntraMus injection – sharp T spike then mall, mood swings, libido, energy Transdermal Patch (late 80’s) – still widely used. Safe steady dose, skin irritation, falls off in exercise Androgel – colorless drying gel rubbed on shoulders 1x a day Convenient to use in almost any man If HRT for andropause common as menopause – Which is the ambition of drug companies DRAMATIC medical and financial consequences Given popular desire to reverse human aging and growing intimacy of commercial and clinical concerns-trend may be irresistible (look up Andropause on net----anti aging web sites) Pharm. Company is “in the business of inventing treatments” how about diseases? Dr. Abraham Morgentaler – urologist specializes in male sexual dysfunction and infertility Views T deficiency in older men as silent epidemic 5 million USA men affected and >95% not diagnosed Replace T?? Restore youthful muscle tone, bone strength, potency, vigor AD in Boston Globe-have T tested-paid for by Unimed Patient in office was getting T levels tested. Doctor said several patients (professors) “made their brains much sharper” Need to make sure no prostate cancer – highly aggravated by T Six biopsies samples to check -PSA (prostate specific antigen) blood test Give you prescription now and you can start once we complete tests T-derived from cholesterol, primarily made in testes via pituitary signals Men older than 40, decreased T by 1.2% per year Patient 1 – little low, excited about T therapy Patient 2 – said Primary care doc normal T 800 ng/dl Morgantaler – T normal range “free T” was another matter Normally 2% free – not bound to other proteins & thus active Patient’s free T little under lower limit (for normal men in mid 20’s) Check PSA & start Androgel FDA never approved Androgel for andropause. Intended for use Klinfelter’s & pituitary dysfunction and viral effected testes Klinfelter’s - Congenital disorder in men, have extra X and underdeveloped testes Not many people with these or similar conditions (pit or hypothamic), yet 35 million US men over 50 so if “andropause takes of”… billions $$$ ERT in menopausal women > 2 billion year for Wyeth, for Premarin Marketing & Medicine part ways Big Pharmaceutical gets approval for drug of rare disease to hopefully expand/profit later on Drug approved – doctor can legally prescribe for any clinical condition FDA prohibits ads of “off label uses”-alternative strategies Run an ad to “raise awareness” of condition Align themselves with experts and “opinion leaders” Finance Certain Research from MD’s Offer them consulting opportunities Endorsed by a major medical society Endocrine Society 2000 – 1st Ann. Andropause Conference Support by Medical Society Helps Panel to define andropause and how it should be treated Men over 50 should be screened & get T therapy if lower than 300 And no condition that would rule out therapy (Prostate cancer) } NO STUDY TO SHOW BENEFIT OF T IN OLDER MEN Panel predicted that Low T found in more than 10% of males over 50 30% of males over 70 7 million MEN in USA Unimed grant sole source of conference funding and recommended panel members. 9 out 13 panelist had ties to drug company BAD!!!!!!!!!!!!!!!!!!!! “Bid to Medicalize Middle age may be supported by pharmaceutical industry, but it remains poorly supported by scientific research” Decline In T levels really responsible for most symptoms in aging men??? What T levels normal??? Andropause exist??? Limits of our medical knowledge was evident from a visit to Dr. William Crowley & Dr. Hayes MGH measure hormone levels Found Huge variability in T levels Studied hypogonadalim and needed good indication of normal T levels Healthy Men in Early 20’s –drew blood every 10 min for 24hrs 15% below normal levels during day > 50% below cutoff T LEVELS REALLY VARY in healthy MEN Efficiency of T receptors (highly efficient, don’t need much T?) - Stress decreases sex steroids - Unsure of Variation in T levels, maybe effected by drug interactions T deficiency may be easily over diagnosed because of variability Don’t understand where # of 5 million andropause men comes from Commercial Tests physicians use notoriously unreliable (300-900) with one test and (160-700) on another Test for free T even less accurate Dr. Morgentaler says doesn’t matter – even gives it as preventative treatment No waiting for scientific validation NIH “closest thing to independent scientific consensus” – says Andropause UNPROVEN Studies on increased lean muscle mass strength and bone mineral density are small (40 men) and effects not dramatic Largest & longest term study showed no improvements in Energy level, sex performance, or strength Uncertainty about effects on decreased T with age UPDATE ON NOVEMBER 2006 NIH (NIA) is conducting a clinical trial to examine declining T levels in men >65 • Expected Total Enrollment: 75 • Expected completion: February 2007 Approximately 20% of men over the age of 70 have low testosterone levels. In some studies, testosterone replacement has resulted in improvement in bone mass, muscle strength, quality of life and memory function. In the body, testosterone is converted into estrogen. Hence, it is unclear whether these beneficial effects are due to testosterone or estrogen. Side effects of T gynecomastia (abnormal breast enlargement) testicular shrinkage (gonads compensate by making less hormone) Also Increases circulating RBC and if excessive blood gets viscous and can lead to congestive heart failure or stroke Men 100 mg/day Androgel over a year 20% prostate disorder like prostatic hyperplasia T really accelerates growth of Prostate Cancer Most Men over 65 have clusters of cancer cells in prostate “occult” and “indolent” Hard to find, may not cause trouble Here the perils are 2 fold 1-unnecessary biopsies lead to unnecessary surgery aimed at eradicating cancer may have stayed inactive 2-biopsies can miss cancer that under T therapy will be more aggressive and become dangerous Safety issue – huge concern NIH thinking of 6 yr study placebo controlled Andropause driven by Pharmaceutical Co rather than physiology Elevate T in 72 yr old man to levels he had at 20 – is this normal Might be better to have lower levels with aging-protect against P cancer Cause epidemic of prostate cancer?? Conventional HRT in women increases risk of Breast Cancer, heart attack, blood clots, and stroke Nationwide trials were SHUT DOWN 26% increase in invasive Breast cancer Nonetheless, T replacement increasingly popular In 2001 sales transdermal T doubled Well over ¼ million US Men use T Rates Continue – 1 million within 2 years Total sales of testosterone in the United States were about $18 million until 1988; the figure rose to $400 million in 2002 In 2004, the testosterone replacement market in Europe and in the US was estimated to be approximately $600 million. The US market is by far the most attractive with a growth rate of 40% (cash) and sales of $537million, of which $422 million were sales of testosterone gels VAST UNCONTROLLED EXPERIMENT APRIL 2010 global sales of testosterone therapies have grown to more than $1 billion per year, with sales of testosterone gels in the US comprising $700 million. Action of T on target cells Hormone binds SHBG in circulation. Sex hormone binding globulin When free can diffuse across PM Acted upon by 5a-reductase to make DHT AR is in cytosol and bound to HSP Displaced by DHT (DihydroT) AR gets phosphorylated and forms a dimer and translocated to the nucleus Binds to promoters at AREs (Androgen Response Elements) Does Menopause exist? Ovary is unique in that woman’s age at which it ceases to function appear to have remained constant despite our increased longevity over last century Loss of ovary function-profound impact on hormonal milieu Risks of disease due to decreased Estrogen In males, germ cells become quiescent and maintain stem cell identity In females, all germ cells differentiate prior to birth 90% of women experience menopause at 51.2 years. Remainder prior to age 46 Only 1% before the age of 40 Both genetic and environmental factors effect decline in fertility and onset of M M=ovarian aging supported by Coincident occurrence of follicular depletion Elevation of gonadotropins Menstrual irregularity with ultimate cessation Estrogens Main estrogen during premenopause is 17b estradiol. Controlled by developing follicle and corpus luteam 95% derived from ovaries Other sources Peripheral conversion from T to estradiol In post menopausal women-estrone Biological potency 1/3 that of estradiol Derived from peripheral conversion from androstenedione. Derived from peripheral conversion from androstenedione. AROMATASE Extra glandular aromatase-fat, liver, some nuclei in hypothalamus Activity increases with age and amount of FAT Estrone and Estradiol 40ug/dl and 6 ug/dl post MEN 80-500 ug/dl in PreMEN Nearly all Estrogen derived from ESTRONE POST men Menopausal consequences 1. Vasomoter symptoms (hot flash) 80% women have for at least a year 25% still have 5 yrs after last period Correlate with pulses of LH Likely some central mediator as LH does not induce hot flash Disturb REM sleep Usually treated with estrogen Menopausal consequences 2. Genital Atrophy Vagina, vulva, urethra and bladder all have estrogen receptors No estrogen-atrophy Itching and vaginal thinning Dryness, painful intercourse pH changes, different flora increase risk of UT infections Treatment-vaginal estrogen. Menopausal consequences 3. Osteoporosis-condition in which bone loss has been sufficient to allow mechanical fracture with limited stress. Menopausal bone loss begins before final menstrual period Post men osteoporosis accounts of 1.3 million fractures per year in USA Most hip fractures (250,000) due to osteoporosis 15% patients die within one year of hip fracture and 75% lose independence Menopausal consequences 3. OSTEOPOROSIS cont….. Bone loss premen 1-2% year Compared to 4% post men Treatment –estrogen Alternative therapies Calcitonin-hormone made by thyroid gland Effect in bone density in 12-18 months SERMS-selective estrogen receptor modulators Calcium and Vitamin D Discussion POINTS Does Menopause exist? YOU BET Women different then men (GERM CELLS) Does andropause EXIST? Maybe not How evil are drug companies? How greedy are some doctors? (politicians) vacation areas for conference Consulting fees • • • HOMOSEXUALITY Proc Natl Acad Sci U S A. 2005 May 17;102(20):7356-61. Brain response to putative pheromones in homosexual men. Savic I, Berglund H, Lindstrom P. Department of Clinical Neuroscience, Karolinska University Hospital, Stockholm, Sweden. The testosterone derivative 4,16-androstadien-3-one (AND) and the estrogen-like steroid estra-1,3,5(10),16-tetraen-3-ol (EST) are candidate compounds for human pheromones. AND is detected primarily in male sweat, whereas EST has been found in female urine. In a previous study, we found that smelling AND and EST activated regions covering sexually dimorphic nuclei of the anterior hypothalamus, and that this activation was differentiated with respect to sex and compound. In the present study, the pattern of activation induced by AND and EST was compared among homosexual men, heterosexual men, and heterosexual women. In contrast to heterosexual men, and in congruence with heterosexual women, homosexual men displayed hypothalamic activation in response to AND. Maximal activation was observed in the medial preoptic area/anterior hypothalamus, which, according to animal studies, is highly involved in sexual behavior. As opposed to putative pheromones, common odors were processed similarly in all three groups of subjects and engaged only the olfactory brain. These findings show that our brain reacts differently to the two putative pheromones compared with common odors, and suggest a link between sexual orientation and hypothalamic neuronal processes. • HOMOSEXUALITY • J Genet. 2004 Dec;83(3):251. – Excess of counterclockwise scalp hair-whorl rotation in homosexual men. Klar AJ. While most men prefer women as their sexual partners, some are bisexual and others are homosexuals. It has been debated for a long time whether a person's sexual preference is innate, learned, or due to a combination of both causes. It was recently discovered that the human right-versus-left-hand use preference and the direction of scalp hair-whorl rotation develop from a common genetic mechanism. Such a mechanism controls functional specialization of brain hemispheres. Whether the same mechanism specifying mental makeup influences sexual preference was determined here by comparing hair-whorl rotation in groups enriched with homosexual men with that in males at large. Only a minority of 8.2% (n = 207) unselected 'control' group of males had counterclockwise rotation. In contrast, all three samples enriched with homosexual men exhibited highly significant (P < 0.0001), 3.6-fold excess (29.8%, n = 272) counterclockwise rotation. These results suggest that sexual preference may be influenced in a significant proportion of homosexual men by a biological/genetic factor that also controls direction of hair-whorl rotation. • HOMOSEXUALITY-yes, it exists in NATURE • J Exp Biol. 2005 Mar;208(Pt 5):891-8. – Social experience and pheromonal perception can change male-male interactions in Drosophila melanogaster. Svetec N, Ferveur JF. Social interaction with conspecifics can influence the developing brain and behaviour of the exposed animal. This experience can involve the exchange and retention of visual, chemical, acoustic and tactile signals. When several Drosophila melanogaster male flies are associated with mated females in the presence of food, they show frequent aggressive interactions. To measure the role of social experience on malemale interaction, two tester males - naive or exposed to sibling(s) during a variable period of their adult development were confronted in the absence of female and food. The two males displayed homosexual courtship and aggressive behaviours, the frequency, intensity and directionality of which varied according to their experience. The effect of social experience was greatly enhanced between transgenic males partially defective for pheromonal perception, indicating that male inhibitory pheromones are normally used to repress malemale interaction. • HOMOSEXUALITY-yes, it exists in NATURE • Evolutionary Theories for HomosexualityBiological Structures and Male Homosexuality • Some of these examples of "homosexuality" in phylogenetically distant animals may be analogous rather than homologous to human homosexuality, but as we move closer to humans the likelihood of homologous behaviors increases. In mammals many different behaviors have been observed that might be associated with male homosexuality. Among primates homosexual behaviors are particularly diverse. • These include such practices as the mounting of one male by another (e.g. Langurs, pig-tailed macaques, baboons, orangutans, chimpanzees, bonobos) (Sommer 1990; Oi 1991; Lorenz 1963; Yamagiwa 1992; Hayaki et al. 1989), including mounting with anal penetration (e.g. stumptailed macaques, squirrel monkeys) (Sommer 1990; Maple 1977), and mounting with anal penetration and ejaculation (Japanese macaques, rhesus macaques, gorillas) (Sommer 1990; Gadpaille 1980; Edwards and Todd 1991). • HOMOSEXUALITY-yes, it exists in NATURE • Homosexuality is a common occurrence in humans and other species, yet its genetic and evolutionary basis is poorly understood. Here, we formulate and study a series of simple mathematical models for the purpose of predicting empirical patterns that can be used to determine the form of selection that leads to polymorphism of genes influencing homosexuality. Specifically, we develop theory to make contrasting predictions about the genetic characteristics of genes influencing homosexuality including: (i) chromosomal location, (ii) dominance among segregating alleles and (iii) effect sizes that distinguish between the two major models for their polymorphism: the overdominance and sexual antagonism models. We conclude that the measurement of the genetic characteristics of quantitative trait loci (QTLs) found in genomic screens for genes influencing homosexuality can be highly informative in resolving the form of natural selection maintaining their polymorphism. Genetic models of • • homosexuality: generating testable predictions. Gavrilets S, Rice WR. PUBLISHED SEP 2006 • Biological versus nonbiological older brothers and men's sexual orientation. • Bogaert AF. • The most consistent biodemographic correlate of sexual orientation in men is the number of older brothers (fraternal birth order). The mechanism underlying this effect remains unknown. In this article, I provide a direct test pitting prenatal against postnatal (e.g., social/rearing) mechanisms. Four samples of homosexual and heterosexual men (total n = 944), including one sample of men raised in nonbiological and blended families (e.g., raised with half- or step-siblings or as adoptees) were studied. Only biological older brothers, and not any other sibling characteristic, including nonbiological older brothers, predicted men's sexual orientation, regardless of the amount of time reared with these siblings. These results strongly suggest a prenatal origin to the fraternal birth-order effect. • • • • • Homosexuality presents a paradox to evolutionary theory. If we grant that there could be such a thing as a gay gene (or at least some kind of genetic basis to sexual orientation), then how are we to explain the persistence of a gay gene in the human population over time? That is, if male homosexuality typically does not lead to offspring, how do those gay genes survive from one generation to the next? This is not a new issue in evolutionary theory. Edward O. Wilson deals with it in his 1975 text Sociobiology, and as far back as the 1950s evolutionary theorists have been offering explanations for the genetic persistence of homosexuality. Moreover, there are a number of other genetic attributes that present the same paradox of persisting despite their seeming mal-adaptivity (e.g., in developing countries sickle cell anaemia usually kills its carriers before they are able to reproduce, yet its frequency in these populations remains high). • • • • Born gay? How biology may drive orientation By Sandi Doughton Seattle Times science reporter As the culture wars rage over gay rights, a flock of sheep at Oregon State University may help answer a key question behind the controversy: Is homosexuality a matter of choice or biology? • The Corvallis herd includes a group of rams that scientists delicately refer to as "male-oriented." These animals consistently ignore females and bestow all their amorous attentions on members of their own sex. • Researcher Charles Roselli says a decade of study suggests sexual orientation is largely hard-wired into the sheep's brains before birth. Now, he's trying to figure out how that happens, zeroing in on genes and hormones. In a bold test of his ideas, he hopes to engineer the birth of gay rams by altering conditions in the womb. • Sheep aren't people, but the Oregon work adds to a growing body of research that bolsters biological explanations for sexual orientation across species — including humans. Impotence physiological basis for control of penile erection is not totally understood. VIP has been implicated as mediator of penile erection Is released when erection is induced Stimulate erection when administered VIP injected into penis doesn’t work so not a good treatment Nitric oxide (NO) is an important mediator of erections. Viagra maintains NO levels • Erectile dysfunction, sometimes called "impotence," is the repeated inability to get or keep an erection firm enough for sexual intercourse. The word "impotence" may also be used to describe other problems that interfere with sexual intercourse and reproduction, such as lack of sexual desire and problems with ejaculation or orgasm. ED indicates that other problems are not involved. • ED can be a total inability to achieve erection, an inconsistent ability to do so, or a tendency to sustain only brief erections. These variations make defining ED and estimating its incidence difficult. Estimates range from 15 -30 million, depending on the definition used. According to the National Ambulatory Medical Care Survey (NAMCS), for every 1,000 men in the United States, 7.7 physician office visits were made for ED in 1985. By 1999, that rate had nearly tripled to 22.3. The increase happened gradually, presumably as treatments such as vacuum devices and injectable drugs became widely available and discussing ED became accepted. The most publicized advance was the introduction of the sildenafil citrate (Viagra) in March 1998. NAMCS data on new drugs show an estimated 2.6 million mentions of Viagra at physician office visits in 1999, and 1/3 of those mentions occurred during visits for a diagnosis other than ED. What causes ED? an erection requires a precise sequence of events, ED can occur when any of the events is disrupted. The sequence includes nerve impulses in the brain, spinal column, and area around the penis, and response in muscles, fibrous tissues, veins, and arteries in and near the corpora cavernosa. Damage to nerves, arteries, smooth muscles, and fibrous tissues, often as a result of disease, is the most common cause of ED. Diseases—such as diabetes, kidney disease, chronic alcoholism, multiple sclerosis, atherosclerosis, vascular disease, and neurologic disease—account for about 70% of ED cases. Between 35- 50 % of men with diabetes experience ED. • Also, surgery (especially radical prostate and bladder surgery for cancer) can injure nerves and arteries near the penis, causing ED. Injury to the penis, spinal cord, prostate, bladder, and pelvis can lead to ED by harming nerves, smooth muscles, arteries, and fibrous tissues of the corpora cavernosa. • In addition, many common medicines—blood pressure drugs, antihistamines, antidepressants, tranquilizers, appetite suppressants, and cimetidine (an ulcer drug)—can produce ED as a side effect. • What causes ED? • Experts believe that psychological factors such as stress, anxiety, guilt, depression, low self-esteem, and fear of sexual failure cause 1020 %of ED cases. Men with a physical cause for ED frequently experience the same sort of psychological reactions (stress, anxiety, guilt, depression). • Other possible causes are smoking, which affects blood flow in veins and arteries, and hormonal abnormalities, such as not enough testosterone. • • • • • John Rock’s error Countdown to a baby Stem cell article Eyes wide shut article Study guide on web, sex hormone lecture, Hormones for Men, countdown to a baby, and pineal gland lecture.