The Peripheral Blood Smear
advertisement

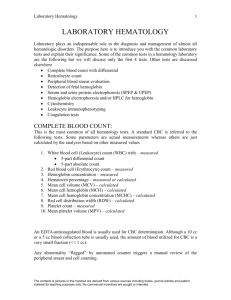
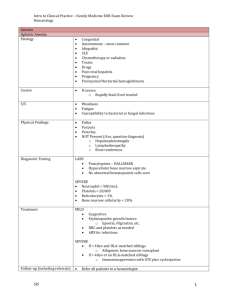
The Peripheral Blood Smear A peripheral blood smear (peripheral blood film) is a glass microscope slide coated on one side with a thin layer of venous blood. The slide is stained with a dye, usually Wright’s stain, and examined under a microscope. Microscopic examination of the peripheral blood is used to supplement the information provided by automated hematology analyzers ("blood cell counters"). Hematology analyzers provide accurate quantitative information about blood cells and can even identify specimens with abnormal cells. However, the precise classification of abnormal cells requires a trained microscopist, a well-made peripheral blood smear, and a light microscope with good optical characteristics. In practice, hematology analyzers of varying sophistication are used for cell counting in all but the smallest hematology laboratories. In addition to providing cell counts and graphical displays of the information recovered, these instruments also provide a warning ("flag") that atypical cells were found and provide a presumptive identification of the abnormality. The instrument operator reviews the information from each specimen and decides if smear preparation and light microscopy are necessary. If not, the information is released to the clinician. Peripheral Blood Smear Preparation The wedge slide ("push slide") technique developed by Maxwell Wintrobe remains the standard method for the preparation of peripheral blood smears (films). The following procedure (Fig. 1) is utilized to prepare a peripheral smear. Place a 1" x 3" glass microscope slide with a frosted end on a flat surface (usually the counter top of a laboratory bench). Attach a label on the slide or write the patient name, specimen identification number, and date of preparation on the frosted surface. Place a 2 - 3 mm drop of blood approximately 1/4" from the frosted slide, using a wooden applicator stick or glass capillary tube. Hold the slide by the narrow side between the thumb and forefinger of one hand at the end farthest from the frosted end. Grasp a second slide ("spreader slide") between the thumb and forefinger of the other hand at the frosted end. Place the edge of the spreader slide on the lower slide in front of the drop of blood (side farthest from the frosted end). Pull the spreader slide toward the frosted end until it touches the drop of blood. Permit the blood to spread by capillary motion until it almost reaches the edges of the spreader slide. Push the spreader slide forward at a 30o angle with a rapid, even motion. Let the weight of the slide do the work. Table 1 Preparation of Peripheral Blood Smear Step 1. Placing a small drop of venous blood on a glass microscope slide, using a glass capillary pipette. A wooden applicator stick can also be used for this purpose. Step 2. A spreader slide has been positioned at an angle and slowly drawn toward the drop of blood. Step 3. The spreader slide has been brought in contact with the drop of blood and is being drawn away. Note layer of blood at the edge of the spreader slide. Step 4. The spreader slide is further pulled out, leaving a thin layer of blood behind. Step 5. The blood smear is nearly complete. Step 6. End result. A glass slide with a wellformed blood film. After drying for about 10 minutes, the slide can be stained manually or placed on an automated slide stainer. Fig. 1. Wedge slide technique for preparation of a peripheral blood smear. A well-made peripheral smear is thick at the frosted end and becomes progressively thinner toward the opposite end. The "zone of morphology" (area of optimal thickness for light microscopic examination) should be at least 2 cm in length. The smear should occupy the central area of the slide and be margin-free at the edges (Fig 2). Fig. 2. Photograph of the peripheral blood smear prepared above. The arrow points to the zone of morphology. Peripheral Blood Smear Examination Peripheral smear examination requires a systematic approach in order to gather all possible information. In addition, all specimens must be evaluated in the same manner, to assure that consistent information is obtained. The following approach is recommended: An examination at low power (10X ocular, 10x objective) is first performed to evaluate the quality of the smear, ascertain the approximate number of white blood cells and platelets, and to detect rouleaux formation, platelet clumps, and leukocyte clumps and other abnormalities visible at low magnification. An optimal area for evaluation at higher magnification is also chosen. This should be an intact portion of the smear free of preparation artifact where the red blood cells are separated by 1/3 to 1/2 of a cell diameter. The red blood cells should stain a pink color, while neutrophils show "crisp" features, with deep blue-purple nuclear material and lilac to pinkish to violet cytoplasmic granules. Optimal preparation and staining of the peripheral blood smear is critical for morphologic examination; an inadequate smear should not be examined. Following low power examination of a peripheral blood smear, the 50X or 100X objective of the microscope is selected (500X or 1000X total magnification when using a 10x ocular) and the area of morphology is examined in a consistent scanning pattern (Fig 3) to avoid counting the same cell(s) twice. A differential count of at least 100 white blood cells (200, 500, or 1000 is even better) is performed, and any abnormal morphology of RBCs, WBCs, and platelets observed during the differential count is recorded. Each morphologic abnormality observed should be quantitated ("graded") separately as to severity ("slight to marked" or "1+ to 4+"). Medical technologists are well trained in the reproducible quantitation of morphologic abnormalities; details are available in medical technology textbooks. A fairly accurate estimate of the white blood cell count (cells/mL) can be obtained by counting the total number of leukocytes in ten 500X microscopic fields, dividing the total by 10, and multiplying by 3000. These estimates should approximate that obtained by the cell analyzer. If the estimate does not match the automated cell count, obtain the original blood specimen, confirm patient identity, repeat the automated analysis, and prepare a new smear. Fig. 3. Scanning technique for peripheral blood differential count and morphologic evaluation. (a) Ten microscopic fields are examined in a vertical direction from bottom to top (or top to bottom). (b) The slide is horizontally moved to the next field (c) Ten microscopic fields are counted vertically. (d) The procedure is repeated until 100 leukocytes have been counted (for a 100-cell count). A peripheral smear must be interpreted in the context of the clinical situation. That is, only limited information can be obtained unless the following information is available with the peripheral smear. The age and sex of the patient must be known, since absolute cell numbers and the significance of some findings vary with age. For example, relative lymphocytosis with NRBCs and atypical lymphocytes would be unusual and pathologic in an adult, but appear in any infant under stress. The red blood cell count (RBC), hemoglobin, hematocrit, mean corpuscular volume (MCV), and red cell distribution width (RDW) cannot be accurately determined by manual smear examination and should be available. The white blood cell count (WBC) and platelet count can be approximated manually, but an automated ("machine") count is helpful. Graphical information provided by the hematology analyzer is helpful but not essential for peripheral blood smear interpretation. Hematology analyzers utilize light scatter, electrical impedance, and other physical parameters to count cells, determine cell size and differentiate different types of blood cells. For example, many modern hematology analyzers measure electrical impedance, light scatter, cell viability, and other parameters during the evaluation process. Light scatter at 0 o roughly corresponds to cell size, 10 o light scatter to cellular internal "complexity," 90 o light scatter to nuclear lobularity, and 90 o depolarized light scatter to cytoplasmic granularity. An example of a light scatter histogram produced by a modern hematology analyzer is shown in Fig 4. Disadvantages of the Peripheral Blood Smear Peripheral blood smear examination provides information that cannot be obtained from automated cell counting. However, peripheral smear evaluation has some limitations and special considerations. These include: Experience is required to make technically adequate smears. There is a non-uniform distribution of white blood cells over the smear, with larger leukocytes concentrated near the edges and lymphocytes scattered throughout. There is a non-uniform distribution of red blood cells over the smear, with small crowded red blood cells at the thick edge and large flat red blood cells without central pallor at the feathered edge. Automated Hematological Evaluation The total red cell count (RBC), RBC size (mean corpuscular volume, MCV), and red cell distribution width (RDW) are determined from analysis of electrical impedance and/or light scattering data by the hematology analyzer. These measurements are used to calculate the hematocrit, MCH, and MCHC. In unusual circumstances the automated hematology analyzer produces cell counts which are falsely increased or decreased. Fortunately, in almost all cases the instruments "flag" the specimen as abnormal so that the operator can verify the results manually or perform necessary corrections. Causes of spurious red blood cell counts include: Very small red blood cells (microcytosis) may be counted as large platelets and result in a falsely decreased RBC. Autoagglutination or cryoglobulins lead to RBC clumping, which may falsely increase the RBC. Spurious elevations in the RBC may also occur in patients with very high WBCs (> 100 x109). Fig. 4. A modern hematology analyzer (Cell Dyn 4000, Abbott Laboratories, Chicago, IL). Sample analysis is performed in the RBC Evaluation Importance of the MCV and RDW The MCV is the median value of the histogram distribution obtained when red blood cell size is plotted against the number of cells ("red cell histogram")(Fig. 5). The MCV, measured in femtoliters (fL, or 10-15 L), is the most important of the red cell indices. It is used to classify anemias as normocytic (normal MCV), microcytic (decreased MCV), or macrocytic (increased MCV). However, the MCV may be falsely elevated in patients with red blood cell agglutination, since the hematology analyzer may identify some of the cell clumps as single cells. In patients with severe hyperglycemia (glucose > 600 mg/dL), osmotic swelling of the red blood cells may also spuriously elevate the MCV. A related parameter, the red cell distribution width (RDW) is the coefficient of variation of the red blood cell distribution histogram. As a quantitative measure of variation in red blood cell size (anisocytosis), the RDW is elevated in iron deficiency anemia, myelodysplastic syndromes, macrocytic anemia secondary to vitamin B12 or folate deficiency, and some malignancies. In contrast, the RDW is usually normal or only mildly elevated in the microcytic anemia of thalassemia. Fig. 5. Red cell distribution histograms. In these histograms, RBC volume (x-axis) is plotted vs. the cell count (number of events counted (y-axis). The mean corpuscular volume (MCV) is the median value of the histogram distribution. The red cell distribution width (RDW) is the coefficient of variation of the curve. Microcytic red cells (a) fall to the left portion of the curve, while macrocytic red cells fall to the right (c). The histogram in the center is from a normocytic, normochromic specimen with an MCV of 88 fL. Measurement of Hematocrit The hematocrit (Hct, "crit") is the ratio of the volume of red blood cells to the volume of whole blood. In the past, the hematocrit was determined by centrifugation of whole blood in a narrow glass tube (capillary blood tube) sealed at one end ("spun hematocrit"). The spun hematocrit is spuriously elevated if plasma becomes trapped in the red cell layer. This phenomenon occurs in patients with polycythemia, macrocytosis, spherocytosis, hypochromic anemias, and RBC fragment syndromes. Improper mixing of the specimen or the addition of excessive anticoagulant can also lead to false Hct values. Since "crit" tubes are also fragile and dangerous to use, spun hematocrits are rarely used today. The automated hematology analyzer calculates the Hct from the RBC and MCV by the following formula: Hct (L/L, %) = RBC (cells/L) x MCV (L/cell) Since the Hct is a calculated value, it is less accurate than either the RBC or Hb, and is affected by errors in either or both of these measurements. The MCV, mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC) are the red blood cell indices. The MCH is the hemoglobin concentration per cell (hemoglobin mass/red blood cell), expressed in picograms per cell (pg, 10-12 g). The MCH is calculated from the hemoglobin and RBC by the following formula: The MCH is decreased in patients with anemia caused by impaired hemoglobin synthesis. The MCH may be falsely elevated in blood specimens with turbid plasma (usually caused by hyperlipidemia) or severe leukocytosis. The MCHC is the average hemoglobin concentration per total red blood cell volume (ratio of hemoglobin mass to RBC volume), as determined from the following equation: The MCHC is decreased in microcytic anemias where the decrease in hemoglobin mass exceeds the decrease in the size of the red blood cell. It is increased in hereditary spherocytosis and in patients with hemoglobin variants, such as sickle cell disease and hemoglobin C disease). Measurement of Hemoglobin Nearly all automated hematology analyzers utilize the cyanomethemoglobin method to measure the hemoglobin content of the red blood cell. In this method, hemoglobin is converted to cyanated methemoglobin (cyanmethemoglobin) by the addition of a solution (Drabkin solution) containing potassium ferricyanide and potassium cyanide. Cyanated methemoglobin maximally absorbs light at 540 nm, and the total amount of hemoglobin is determined by spectrophotometry. The hemoglobin concentration is measured in grams per deciliter (g/dL) of whole blood. Hyperlipidemia, fat droplets (from hyperalimentation), hypergammaglobinemia, cryoglobulinemia, and leukocytosis (> 50 x 109/mL) can result in spurious elevations of hemoglobin concentration. Spurious hemoconcentration or hemodilution, occurring with improper specimen collection, may falsely elevate or decrease hemoglobin concentrations. In addition, the age, sex, and race of the patient must also be considered in the interpretation of hemoglobin levels. Hemoglobin levels fall during the first month of life and remain relatively low until after puberty. The mean male hemoglobin level is 1 - 2 g/dL higher than the mean female level. Blacks of both sexes and all ages have hemoglobin levels which are 0.5 - 1.0 g/dL lower than whites of the same age and sex. White Blood Cell Evaluation The total white blood cell count (WBC, leukocyte count) includes all circulating nucleated hematopoietic cells with the exception of nucleated red blood cells (NRBCs). The WBC is of great importance in the diagnosis and management of patients with hematologic and infectious diseases. It is also used to monitor patients receiving cytotoxic drugs, radiation therapy, and some antimicrobial drugs. The WBC is determined on EDTA-anticoagulated blood. RBCs are removed by lysis, and the total WBC is measured by electrical impedance or light scatter techniques. Unlysed red blood cells, nucleated red blood cells, platelet clumps, large platelets, and cryoglobulins may result in spurious WBC results. If these conditions are detected by the hematology analyzer, the specimen is "flagged" for a manual peripheral smear evaluation. Occasionally, a manual WBC, using a hemacytometer, may be necessary to verify the accuracy of an automated WBC. If NRBCs are present, a relative estimate of their number is obtained by light microscopy and expressed as # NRBCs/100 WBC. Under these circumstances, the total WBC must be corrected by use of the following formula: Differential Leukocyte Count The differential leukocyte count (leukocyte differential, white blood cell differential) is probably the least understood and overutilized of all hematologic assays. Until the 1980’s, the relative number (%) of each type of white blood cell was determined by manual examination of the peripheral blood smear and multiplied by the white cell count to obtain the absolute leukocyte count (cells/mL). Unfortunately, the manual differential is labor intensive, subjective, statistically unreliable (only 100-200 cells are counted), and inaccurate because of nonrandom distribution of cells on the smear (monocytes at the edge, lymphocytes in the middle). Hematology analyzers are more accurate than the manual count for leukocyte elaboration under normal circumstances. For example, the hematology analyzers used in the Hematology Laboratories at WVU Hospitals generates a five-part differential based on electronic impedance, conductivity, and light scatter measurements (Fig. 6). Cell counting with these instruments is rapid, objective, statistically significant (8000 or more cells are counted), and not subject to the distributional bias of the manual count. In addition, the precision of the automated differential makes the absolute leukocyte count reliable and reproducible. Hematology analyzers cannot yet correctly identify all abnormal white blood cells, and manual examination of the peripheral smear is still needed under some circumstances (blasts and immature cells, atypical lymphocytes, leukopenia, etc.). Specimens that meet one or more of abnormal criteria are flagged for manual examination. Depending on the patient population, a manual smear examination is required in only approximately 25% of peripheral smears. Fig. 6. Normal leukocyte differential histogram from a modern hematology analyzer (Cell-Dyn 4000, Abbott Diagnostics). Scatterplot obtained from laser light scatter analysis of white blood cells. y-axis represents data obtained by light scatter at 0o (measure of cell size), while x-axis represents laser light scatter at 7o (cell internal complexity). Each "dot" represents data from a single cell. Clusters of cells represent neutrophils (66.6%), monocytes (8.63%), lymphocytes (22.2%), eosinophils (2.23%), and basophils (0.35%) present in the specimen. The total white blood count was 6.89 x 109/L. Absolute vs. Relative Leukocyte Counts The absolute leukocyte count provides clinical information of much greater value than the relative differential count. In fact, the relative count can be misleading, and the sole use of this parameter can conceal the diagnosis of certain cytopenias or obscure clinically significant trends that are occurring. The absolute neutrophil count, (ANC) and not the relative count, is helpful in monitoring chemotherapy patients, and the absolute neutrophil count is a superior indicator of infection and inflammation. The report of an abnormal blood count is often the first clue to an abnormality of the white cell series; less commonly, the patient presents with an infection or other clinical problem. However, the peripheral blood leukocyte count is only one measure of white cell activity, and several factors must be considered in data interpretation. For example, a patient with a total white blood cell count of 2000/mL and 100 neutrophils/mL has a different problem from a patient with a white blood count of 2000/mL and 100 lymphocytes/mL. Absolute leukocyte numbers must be always be reviewed. In addition, the peripheral blood is only a conduit for leukocytes, and only a small percentage of the total white blood cells in the body are present in the peripheral blood at any one time. Therefore, the total white blood count and absolute leukocyte count must be interpreted in light of the physical findings and other laboratory data. Common causes are summarized in Table I. Table I Common Causes of Altered Leukocyte Counts Decreased Increased Neutrophil Congenital Hereditary neutropenia Acquired Infections Acquired Tissue destruction Bone marrow disease Corticosteroids, lithium Immune reactions Neoplastic growth Drugs Leukemoid reaction Gram-negative septicemia Myeloproliferative disorders Lymphocyte Congenital Acquired Congenital immunodeficiency Viral infection (EBV, hepatitis, disease etc.) Some fungal, parasitic infections Acquired Rare bacterial infection Severe infection (Pertussis) Drugs (Corticosteroids, alkylating) Allergic reactions/drug GI disease sensitivities Immunodeficiency Immunologic disease Monocyte Acquired Mycobacterial infection Acquired Tuberculosis, syphilis Hairy cell leukemia Subacute bacterial endocarditis Corticosteroids Inflammatory responses Recovery phase of neutropenia Myeloproliferative disorders Eosinophil Acquired Acquired Bacterial infection ACTH administration Basophil Acquired Corticosteroids Parasitic infections Drug therapy Hypersensitivity reactions Pulmonary disease Myeloproliferative diseases Acquired Myeloproliferative syndromes Lymphoproliferative disease Hypersensitivity reactions Hodgkin’s disease Some viral infections Myxedema Influence of Age on Leukocyte Count The lymphocyte is the predominant white blood cell in young children, while the neutrophil is predominant in normal adults. Each laboratory is required to establish "normal" leukocyte ranges for different ages, and this information must be displayed on the report from the laboratory. Age-related changes in the cellular composition of the blood must be considered during the interpretation of leukocyte counts. Platelet Evaluation The platelet count is one of several laboratory assays of importance in the functional evaluation of the hemostatic system. A decreased platelet count (thrombocytopenia) can result from a marrow production problem or a peripheral platelet destructive process. Bleeding complications or even death can result in the presence of a severely decreased platelet count. Elevated platelet counts (thrombocytosis) can result from a reactive or neoplastic process. EDTA-anticoagulated blood is preferred for platelet counts, but the specimen must be thoroughly mixed to prevent platelet clumping and falsely decreased platelet counts (spurious thrombocytopenia). However, rare individuals have EDTA-activated, nonpathogenic anti-platelet antibodies and require citrate-anticoagulated blood specimens for platelet counting. Other than platelet clumping, red and white blood cell fragments are most often responsible for interference with accurate platelet counts. Modern hematology analyzers calculate the mean platelet volume (MPV), based on a platelet distribution histogram. The MPV is increased in patients with peripheral platelet destructive processes, in whom young, large platelets are rapidly released from the bone marrow. The MPV is decreased in cases of thrombocytopenia due to marrow suppression. Morphologic Evaluation of Red Blood Cells Normal red blood cells ("normocytes," "discocytes") are round to very slightly ovoid cells with a mean diameter of approximately 7 mm and a central pale area ("area of central pallor") approximately 1/3 the diameter of the cell that gradually fades towards the more deeply stained periphery. The RBC is approximately the same size as the nucleus of a mature lymphocyte. Any deviation in size, volume, or shape represents an abnormal red blood cell. Clinical Importance of RBC Morphology Since different types of abnormal red blood cells arise by different etiologic processes, disease diagnosis can often be made by interpretation of red blood cell pathology in conjunction with CBC data and other clinical and laboratory information. The following diagram (Fig. 5) shows the etiology of the more common abnormal red blood cells, and they are individually discussed below. Classification of RBC Morphologic Abnormalities A summary table of red blood cell morphologic abnormalities is included on another page (go there). Acanthocytes Acanthocytes ("spur cells, spicule cells") are spheroid RBCs with a few large spiny (thorny) projections. There are usually 5-10 spicules per cell, which show irregular spacing and thickness. Acanthocytes must be differentiated from echinocytes, which have shorter and more regular spicules (see below). Occasional acanthocytes can be seen after splenectomy, in patients with alcoholic cirrhosis, and in hemolytic anemias caused by pyruvate kinase (PK) deficiency. microangiopathic hemolytic anemia, autoimmune hemolytic anemia, sideroblastic anemia, thalassemia, severe burns, renal disease, McLeod phenotype, or infantile pyknocytosis. The majority of erythrocytes form acanthocytosis in the rare disease abetalipoproteinemia. Therefor, serum lipid evaluation is recommended if large numbers of acanthocytes are seen in the absence of an obvious clinical cause. Agglutination True agglutination is irregular clumping and agglutination of red blood cells into grapelike clusters. True agglutination must be differentiated from the rouleaux formation (pseudoagglutination) seen in patients with paraproteins or marked hypergammaglobulinemia or fibrinogenemia, which produces more regularly spaced clusters of red blood cells adhering side-to-side ("coin stacks," see below). True red cell agglutination usually indicates the presence of a cold reactive anti-red blood cell antibody ("cold agglutinin") found in cold agglutinin syndrome or paroxysmal cold hemoglobinuria, although some warm-reactive autoantibodies with wide temperature specificity may produce similar agglutination. True agglutination and pseudoagglutination cannot always be differentiated by light microscopy, but the Coomb’s test, cold agglutinin titer, and serum/urine protein analysis can provide additional information. Basophilic stippling Basophilic stippling is the occurrence of fine, medium, or coarse blue granules uniformly distributed throughout some red blood cells. Fine stippling may be associated with polychromatophilia, while coarse stippling usually indicates impaired erythropoiesis. Heavy metal poisoning (e.g. lead and arsenic), hemoglobinopathies, thalassemias, sideroblastic anemias, pyrimidine-5’-nucleotidase deficiency, and other diseases should be excluded when coarse basophilic stippling is found. Bite cells Bite cells (degmacytes) are RBCs with peripheral single or multiple arcuate defects ("bites"). They are usually accompanied by at least a few blister cells (RBCs with vacuoles or markedly thin areas at periphery of membrane), acanthocytes, and schistocytes. Bite cells are associated with oxidant stress to the red blood cell. They can be found in normal individuals receiving large quantities of aromatic drugs (or their metabolites) containing amino, nitro, or hydroxy groups, or in patients with red-cell enzymopathies involving the pentose phosphate shunt (most notably G-6-PD deficiency, pyruvate kinase deficiency) during acute hemolytic episodes following exposure to oxidant stress. If indicated, a Heinz body test, G-6-PD level, and other studies of red blood cell metabolism may be indicated. Blister cells Blister cells are red blood cells with vacuoles or markedly thin areas at periphery of membrane. These cells are characteristic of glucose-6-phosphate dehydrogenase (G-6PD) deficiency and other conditions imposing oxidant stress on the erythrocyte. Codocytes Codocytes ("target cells") are thin, hypochromatic cells with a round area of central pigmentation. Codocytes are characteristically seen after splenectomy, and in patients with thalassemia, and certain hemoglobinopathies (hemoglobin SS, SC, CC, EE, AE, sickle cell-thalassemia). They are also found in association with iron deficiency anemia, liver disease, and familial lecithin-cholesterol acyltransferase (LCAT) deficiency. If indicated, hemoglobin electrophoresis, liver function evaluation, serum iron studies, serum lipid profile and/or other studies may be indicated. Dacrocytes Dacrocytes ("tear drop cells") are red blood cells in the shape of a teardrop. Microcytosis and hypochromia usually accompany them. Dacrocytes are characteristically seen in relatively large numbers in patients with myelophthisic anemia (particularly myelofibrosis with myeloid metaplasia), but can be found in moderate numbers in megaloblastic anemia, beta-thalassemia, renal failure, tuberculosis, Heinz body disease, acquired hemolytic anemia, hypersplenism, and other hematologic diseases. Teardrop cells are pathologic and usually indicate significant bone marrow dysfunction. Clinical correlation and patient follow up is essential. Drepanocytes Drepanocytes ("sickle cells") are curved, irregular red blood cells with pointed ends, which are characteristic of the "sickle" hemoglobinopathies. Diseases with Hb S (sickle cell anemia, hemoglobin SC disease, hemoglobin S-beta-thalassemia, hemoglobin SD disease, hemoglobin Memphis/S disease) are the usual cause, but drepanocytes can also be seen in other hemoglobinopathies (especially Hb I, Hb C-Harlem, Hb C Capetown). A sickle cell screen and/or hemoglobin electrophoresis may be indicated. Echinocytes/Burr Cells Echinocytes ("sea urchin cells") are red blood cells with multiple tiny spicules (10-30) evenly distributed over the cell surface. These cells result from exposure of the red cell to fatty acids, lysolecithin, amniotic compounds, elevated pH, and other substances. They occur post-splenectomy, after the administration of heparin, in the hemolyticuremic syndrome, and in hepatitis of the newborn, pyruvate kinase deficiency, phosphoglycerate kinase deficiency, uremia, and malabsorption states. Burr cells ("crenated cells") are similar in appearance, but show an uneven distribution of spicules. Burr cells are characteristically seen in uremia, where they represent damaged or fragmented red blood cells. Fig. 7. Representative examples of red blood cells with abnormal morphology. Elliptocytes Elliptocytes are cells with an elliptical shape, while ovalocytes have an oval shape. Severe elliptocytosis (> 10% elliptocytes) is characteristic of hereditary elliptocytosis, but can be prominent in thalassemia, sickle cell trait, and Hb C trait. Elliptocytic hemolytic anemia (< 10% has been reported in association with cirrhosis, decreased erythrocyte glutathione, and with glucose-6-phosphate deficiency. Other diseases where elliptocytosis occurs include iron deficiency anemia, megaloblastic anemia, myelophthisic anemia, and mechanical trauma. Rare elliptocytes (< 1%) occur in normal peripheral blood smears. If clinically indicated, osmotic fragility evaluation, hemoglobin electrophoresis, and studies of red blood cell metabolic activity may be indicated for further evaluation of patients with elliptocytosis. Howell-Jolly bodies Howell-Jolly bodies are small (1 mm) dense, perfectly round basophilic red cell inclusions which represent nuclear material derived from nuclear fragmentation ("karyorrhexis) or incomplete nuclear expulsion during normoblastic maturation. HowellJolly bodies produced in non-diseased individuals are effectively removed by the spleen and are not visible in the circulation. However, Howell-Jolly bodies are readily identified in splenectomized patients and may also be seen in smaller numbers in patients with megaloblastic anemia, severe hemolytic processes, hyposplenism, and myelophthisitic anemia. Hypochromia Hypochromia is a decreased amount (MCH) and concentration (MCHC) of hemoglobin in red blood cells. In the peripheral blood smear, hypochromic cells have an expanded central zone of pallor. Small hypochromic red blood cells (microcytes) are usually present, and the mean corpuscular volume (MCV) is decreased. Microcytosis and hypochromia are characteristic of iron deficiency anemia and other microcytic, hypochromic anemias [anemia of chronic disease, hereditary hemoglobinopathies with diminished globin synthesis (thalassemias, hemoglobin E, hemoglobin H), red blood cell enzyme deficiencies (sideroblastic anemias, lead poisoning, pyridoxine deficiency)]. Serum iron studies, erythrocyte sedimentation rate (ESR), hemoglobin electrophoresis, bone marrow examination, and serum and urine lead quantitation are other laboratory studies may be indicated. Fig. 8. Comparison of normal peripheral blood smear and smear from a patient with severe microcytic, hypochromic anemia. Hyperchromia Hyperchromia is an increase in the red blood cell hemoglobin concentration (MCHC > 36 g/dL). Since it is usually associated with spherocytosis, peripheral smear examination reveals many spherocytes and microspherocytes. Consideration of hereditary spherocytosis is recommended, but spherocytes are also seen in patients with isoimmune and autoimmune hemolytic anemias, Heinz body hemolytic anemia, hereditary pyropoikilocytosis, and severe burns. If indicated, an osmotic fragility assay, Coombs’ test, serum bilirubin, LDH, and haptoglobin, and other laboratory assays may be indicated. Keratocytes/ schistocytes Keratocytes ("horn cells, helmet cells") and schistocytes ("fragmented cells") are damaged red blood cells. Such damage characteristic occurs from fibrin deposits (DIC, microangiopathic hemolytic anemia, thrombotic thrombocytopenic purpura (TTP), prosthetic heart valves, severe valvular stenosis, malignant hypertension, or march hemoglobinuria. However, keratocytes and schistocytes also occur in normal newborns and in patients with bleeding peptic ulcer, aplastic anemia, pyruvate kinase deficiency, vasculitis, glomerulonephritis, renal graft rejection, severe burns, iron deficiency, thalassemia, myelofibrosis with myeloid metaplasia, hypersplenism and postsplenectomy, and other diseases. Clinical correlation is recommended, with the appropriate diagnostic studies. These cells are pathologic and should never be ignored. Knizocytes Knizocytes ("pinch bottle cells") are characteristically seen in patients with hemolytic anemia, including hereditary spherocytosis. An osmotic fragility assay, Coombs’ test, serum bilirubin, LDH, and haptoglobin, and other laboratory assays may be indicated. Macrocytes Oval macrocytes ("macroovalocytes, megalocytes") are large oval red blood cells (> 8.5 mm) with an elevated MCV (> 100 fL, frequently > 120 fL) and normal MCH. The presence of these cells suggests impaired bone marrow DNA synthesis, and may indicate a vitamin B12 or folate deficiency. Serum vitamin B12 or folate levels are usually indicated and a bone marrow examination may be needed. Round macrocytes are slightly to moderately larger than normal (macrocytosis, MCV >95 fL but usually < 120 fL) and are round in shape. This finding suggests impaired bone marrow impaired DNA synthesis, stress erythropoiesis, or excessive surface membrane. Possible clinical causes include liver disease (obstructive jaundice, alcoholism), impaired DNA synthesis from chemotherapy or inherited diseases, myeloproliferative disorders, myelodysplastic syndromes, or splenectomy. Bone marrow examination, liver function studies, and other laboratory assays if clinically indicated. Fig. 9. Comparison of normal peripheral blood smear and smear from a patient with severe microcytic, hypochromic anemia. Microcytes Microcytes are small red blood cells (MCV < 80 fL) with decreased amounts of hemoglobin formed as a result of iron deficiency and defective hemoglobin synthesis, imbalance of globin chains, or defective porphyrin synthesis. Possible clinical causes of microcytosis include iron deficiency anemia, thalassemia, the anemia of chronic disease, lead poisoning, and sideroblastic anemias. Nucleated red blood cells Nucleated red blood cells (NRBCs, normoblasts) are immature red blood cells. In an adult, the presence of NRBCs indicates markedly accelerated erythropoiesis and/or severe bone marrow stress. Clinical conditions associated with peripheral normoblastosis include acute bleeding, severe hemolysis, myelofibrosis, leukemia, myelophthisis, and asplenia. The presence of NRBCs in the peripheral blood of an adult always indicates a significant disease process, the etiology of which must be delineated. NRBCs in the peripheral blood of an infant indicates significant stress but does not have the ominous significance of features of those in an adult. Poikilocytosis Poikilocytosis is variation in red blood cell shape, seen in many disorders. Polychromasia Polychromasia ("polychromatophilia") is the occurrence of slightly immature red blood cells, which are larger than normal (increased MCV) and have a blue-gray coloration. Polychromasia is due to the presence of ribosomal protein in immature red blood cells, which pick up the basophilic component of the Wright-Giemsa stain. Small numbers of these cells (0.5 - 2%) are normally present in the peripheral blood and signify the presence of erythropoietic activity in the bone marrow. They are increased in states of increased erythropoietic activity in response to anemia or the iatrogenic administration of erythropoietin or another marrow stimulatory agent. The MCV may increase slightly in response to significant polychromasia. Decreased polychromasia is seen with hypoproliferative marrow states. Rouleaux formation Rouleaux formation ("pseudoagglutination") is a linear arrangement of RBCs ("coinstack") caused by an increased blood concentration of fibrinogen, globulin, or paraproteins. Associated clinical disorders include acute and chronic inflammatory disorders, Waldenstrom’s macroglobulinemia, and multiple myeloma. Serum and urine protein analysis should be performed in the absence of an acute or chronic inflammatory disease to determine if a paraprotein is present. Spherocytes Spherocytes are small (< 6.5 mm), dense spheroidal RBCs with normal or decreased MCV and absent central pallor. Hereditary spherocytosis is likely if large numbers of spherocytes are present and other forms of abnormal RBCs are absent. Small numbers of spherocytes, in combination with other abnormal RBCs, are seen in patients with isoimmune and autoimmune hemolytic anemias, Heinz body hemolytic anemia, hereditary pyropoikilocytosis, microangiopathic hemolytic anemia, hypersplenism and post-splenectomy, myelofibrosis with myeloid metaplasia, hemoglobinopathies, malaria, liver disease, recent transfusions, and severe burns. An osmotic fragility assay, Coombs’ test, serum bilirubin, LDH, and haptoglobin, and other laboratory assays may be indicated. Stomatocytes Stomatocytes are uniconcave red blood cells with a slit-like area of central pallor. A predominance of stomatocytes is characteristic of hereditary stomatocytosis (a type of hemolytic anemia). Small numbers of stomatocytes (usually in association with other abnormal RBCs) occur in patients with acute alcoholism, cirrhosis, obstructive liver disease, advanced malignancy, severe infections, Rhnull disease, treated acute leukemia, and other diseases. Morphologic Evaluation of White Blood Cells Clinical Importance of WBC Morphology Light microscopy is of greatest value in confirming the automated white blood cell count and performing a manual differential count. However, specific morphologic abnormalities of leukocytes occur, and can provide evidence of disease processes. Classification of WBC Morphologic Abnormalities Alder-Reilly granules Alder-Reilly granules are large, coarse, dark purple, azurophilic granules that occur in the cytoplasm of most granulocytes. These are characteristically found in the AlderReilly anomaly and in patients with mucopolysaccharidoses. Auer rods Auer rods are needle- or rod-shaped, eosinophilic structures which occur in the cytoplasm of immature leukocytes (blasts) and more mature cells in some patients with acute myelogenous leukemia (AML). These structures are formed from coalescing primary (azurophilic) granules. Although Auer rods occur singly in AML FAB subtypes M1, M2, and M4, cells with numerous Auer rods are common in the hypergranular form of AML FAB M3 to form "faggot" cells. Chédiak-Higashi granules Chédiak-Higashi granules are very large red or blue granules that appear in the cytoplasm of granulocytes, lymphocytes, or monocytes in patients with the ChédiakSteinbrinck-Higashi syndrome. Döhle bodies Döhle bodies are variably sized (0.1 to 2.0 um) and shaped, blue or grayish-blue cytoplasmic inclusions usually found near the periphery of the cell. Dohle bodies are lamellar aggregates of rough endoplasmic reticulum, which appear in the neutrophils, bands, and metamyelocytes of patients with infection, burns, uncomplicated pregnancy, toxic states, or during treatment with hematologic growth factors such as G-CSF. May-Hegglin anomaly Neutrophils contain small basophilic cytoplasmic granules which represent aggregated ribosomes. Leukopenia and large platelets are also found. An autosomal dominant trait, the May-Hegglin anomaly is associated with a mild bleeding tendency, but not by an increased susceptibility to infection. Neutrophilic hypergranulation (toxic granulation) Small dark blue to purple granules resembling primary granules appear in the cytoplasm of methmyelocytes, bands, and segmented neutrophils during inflammatory states, burns, and trauma, and upon exposure to hematopoietic growth factors such as granulocyte-colony stimulating factor (G-CSF). Toxic granulation is usually accompanied by a "shift to the left" in the neutrophilic population, and by the presence of vacuolations in the cytoplasm (toxic vacuolations) and Dohle bodies. Neutrophilic hypogranulation XXX Neutrophilic hypersegmentation Increased lobulation of granulocyte nuclei (neutrophilic hypersegmentation) is a characteristic finding in megaloblastic anemia, but can also be seen as an inherited autosomal dominant trait (hereditary hypersegmentation of neutrophils). Neutrophilic hyposegmentation Single or bi-lobed neutrophils (Pelger-Huët cells) can be inherited (Pelger-Huët anomaly), or acquired (pseudo-Pelger-Huët cells) in patients with malignant myeloproliferative disorders (including preleukemia and myelodysplastic syndromes) and infections or tumors which have metastasized to the bone marrow. Large, purple or dark-blue azurophilic granules in the cytoplasm of neutrophils, bands, and metamyelocytes are characteristically seen in patients with severe infection, septicemia, toxic states, and chemical poisoning. Cytoplasmic vacuolation is seen as well. Morphologic Evaluation of Platelets Clinical Importance of WBC Morphology Light microscopy is of greatest value in confirming the automated platelet count and performing a manual differential count in patients with very high or very low platelet counts where automated counting is inaccurate. However, care morphologic evaluation may reveal abnormalities which can support other observations. Classification of WBC Morphologic Abnormalities Platelet hypogranularity Many small, reddish-purple granules are normally present in the cytoplasm of the platelet. These granules, which vary in size and shape, represent dense bodies, alphabodies, and lysosomes. Hypogranular platelets, as the name implies, have little, if any, of the purple-red granules found in normal platelets. These granules may be decreased in number or absent in patients with myeloproliferative diseases and myelodysplastic syndromes. In these disorders, platelet hypogranulation is usually accompanied by abnormalities in platelet size and shape, anemia, leukocytosis or leukopenia, and abnormalities in leukocyte morphology. Large and giant platelets Platelets are normally 1.5 to 3 microns in diameter. However, platelet size can increase in patients with increased platelet turnover from bleeding or stress, and in the myeloproliferative and myelodysplastic disorders. Large platelets are 3 to 7 microns (roughly the diameter of a normal RBC), while giant platelets are larger than red cells. Morphology may appear normal or abnormal. Platelet satellitism In this unusual phenomenon, normal platelets adhere to the surface of neutrophils, or, rarely monocytes, to form "platelet rosettes." Platelet satellitism is associated with blood specimens anticoagulated with EDTA, and disappears when heparin-anticoagulated blood is collected from the same patient. Although an innocuous finding, significant platelet satellitism may cause spurious thrombocytopenia, since the cell-bound platelets are not counted with the platelet fraction of the blood specimen. References and Additional Reading Expert Panel on Cytometry. Reference method for the enumeration of erythrocytes and leucocytes. International Council for Standardization in Haematology. Clin. Lab. Haematol. 16(2):131-138, 1994. Bain, B.J. and Cavill, I.A. Hypochromic macrocytes: are they reticulocytes? J. Clin. Pathol. 46(10):963-964,1993. Bellows, C.F., Salomone, J.P. et al. What's black and white and red (read) all over? The bedside interpretation of diagnostic peritoneal lavage fluid. Am. Surg. 64(2):112118,1998. Bessman, J.D. More on the RDW. Am. J. Clin. Pathol. 84(6):773, 1985. Braun, J., Lindner, K. et al. Percentage of hypochromic red blood cells as predictor of erythropoietic and iron response after i.v. iron supplementation in maintenance haemodialysis patients. Nephrol. Dial. Transplant. 12(6):1173-1181,1997. Buchanan, G.R., Holtkamp, C.A. et al. Formation and disappearance of pocked erythrocytes: studies in human subjects and laboratory animals. Am. J. Hematol. 25(3):243-251, 1987. Clodfelter, R.L., Jr. The peripheral smear. Emerg. Med. Clin. North. Am. 4(1):59-74, 1986. Corazza, G.R., Ginaldi, L. et al. Howell-Jolly body counting as a measure of splenic function. A reassessment. Clin. Lab. Haematol. 12(3): 269-75, 1990. Eldibany, M.M., Totonchi, K.F. et al. Usefulness of certain red blood cell indices in diagnosing and differentiating thalassemia trait from iron-deficiency anemia. Am. J. Clin.Pathol. 111(5):676-82,1999. England, J.M. Future needs and expected trends in peripheral blood cell analysis: erythrocyte histograms. Blood Cells 11(1):61-76,1985. Fossat, C., David,M. et al. New parameters in erythrocyte counting. Value of histograms. Arch. Pathol. Lab. Med. 111(12):1150-1154,1987. Fraser, C. G., Wilkinson, S.P. et al. Biologic variation of common hematologic laboratory quantities in the elderly. Am. J. Clin. Pathol. 92(4): 465-470,1989. Harkins, L. S., Sirel, J.M. et al. Discriminant analysis of macrocytic red cells. Clin. Lab. Haematol. 16(3): 225-234,1994. Isaacs, D., Altman, D.G. et al. Racial differences in red cell indices. J. Clin. Pathol. 39(1): 105-109,1986. Joyner, R. E. and Brooks. M.J. Evaluation of the automated leucocyte count and differential from the Cell-Dyn 3500 in sickle cell disease. Clin. Lab. Haematol. 17(4):329-333, 1995. Keenan, W. F., Jr. Macrocytosis as an indicator of human disease. J. Am. Board Fam. Pract. 2(4):252-256,1989. Kim, S. K., Cheong, W.S. et al. Red blood cell indices and iron status according to feeding practices in infants and young children. Acta Paediatr. 85(2):139-144,1996. Kvinesdal, B.B. and Jensen, M.K. Pitted erythrocytes in splenectomized subjects with congenital spherocytosis and in subjects splenectomized for other reasons. Scand. J. Haematol. 37(1):41-43,1986. Lawrence, C., Fabry, M.E. et al. Red cell distribution width parallels dense red cell disappearance during painful crises in sickle cell anemia. J. Lab. Clin. Med. 105(6):706710, 1985. Lopez, B. L., Griswold, S.K. et al. The complete blood count and reticulocyte count--are they necessary in the evaluation of acute vasoocclusive sickle-cell crisis? Acad. Emerg. Med. 3(8):751-757,1996. Lurie, S. Changes in age distribution of erythrocytes during pregnancy: a longitudinal study." Gynecol. Obstet. Invest. 36(3):141-144,1993. Manfredini, R., Salmi, R. et al. Haematological profile in cancer patients: analysis of circadian pattern. J. Int .Med. Res. 22(6):343-349,1994. Meytes, D., Leshno, D. et al. Persistent abnormalities in red cell parameters following treatment of lymphoma. Leuk. Lymphoma 15(3-4):341-345,1994. Michaels, L. A., Cohen, A.R. et al. Screening for hereditary spherocytosis by use of automated erythrocyte indexes. J. Pediatr. 130(6):957-960,1997. Monzon, C. M., Beaver, B.D. et al. Evaluation of erythrocyte disorders with mean corpuscular volume (MCV) and red cell distribution width (RDW). Clin. Pediatr. (Phila) 26(12):632-638,1987. Reinhart, W. H. and Chien, S. Red cell rheology in stomatocyte-echinocyte transformation: roles of cell geometry and cell shape. Blood 67(4):1110-1118,1986. Roberts, G. T. and El Badawi,S.B. Red blood cell distribution width index in some hematologic diseases. Am. J. Clin. Pathol. 83(2):222-226,1985. Rodgers, M. S., Chang, C. C. et al. Elliptocytes and tailed poikilocytes correlate with severity of iron- deficiency anemia. Am. J. Clin. Pathol. 111(5): 672-675, 1999. Rosenmund, A., Kochli, H.P. et al. Sex-related differences in hematological values. A study on the erythrocyte and granulocyte count, plasma iron and iron-binding proteins in human transsexuals on contrasexual hormone therapy. Blut 56(1): 13-17, 1988. Sassier, P. and Couzineau, P. (1986). Statistical analysis of red blood cell distribution: its importance in recognizing spuriously elevated platelet counts. Am. J. Clin. Pathol. 86(3): 407-411, 1986. Seppa, K., Sillanaukee, P. et al. Abnormalities of hematologic parameters in heavy drinkers and alcoholics. Alcohol Clin. Exp. Res. 16(1): 117-121, 1992. Siebers, R. W., Carter, J.M. et al. Interrelationship between platelet count, red cell count, white cell count and weight in men. Clin. Lab. Haematol. 12(3): 257-262, 1990. Simel, D. L., DeLong, E.R. et al. Erythrocyte anisocytosis. Visual inspection of blood films vs automated analysis of red blood cell distribution width. Arch. Intern. Med. 148(4): 822-824, 1988. Tatsumi, N., Tsuda, I. et al. Size distribution curves of blood cells in thalassemias and hemoglobin H diseases." Southeast Asian J. Trop. Med. Public Health 23 Suppl 2: 7985, 1992. Yoo, D. and Lessin, L.S.. Drug-associated "bite cell" hemolytic anemia. Am. J. Med. 92(3): 243-248, 1992.